54
|
wileyonlinelibrary.com/journal/clr Clin Oral Impl Res. 2018;29(Suppl. 18):54–92. Accepted: 1 May 2018DOI: 10.1111/clr.13282
S U P P L E M E N T A R T I C L E
The effect of antiresorptive drugs on implant therapy:
Systematic review and meta‐analysis
Andreas Stavropoulos
1| Kristina Bertl
1,2| Peter Pietschmann
3|
Nikolaos Pandis
4| Morten Schiødt
5| Björn Klinge
11Department of Periodontology, Faculty of Odontology, University of Malmö, Malmö, Sweden
2Division of Oral Surgery, School of Dentistry, Medical University of Vienna, Vienna, Austria
3Institute of Pathophysiology and Allergy Research, Center of Physiology and Pathophysiology, Medical University of Vienna, Vienna, Austria
4Department of Orthodontics and Dentofacial Orthopedics, School of Dental Medicine, Department of Orthodontics, University of Bern, Bern, Switzerland
5Department of Oral & Maxillofacial Surgery, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
Correspondence
Andreas Stavropoulos, Department of Periodontology, Faculty of Odontology, University of Malmö, Malmö, Sweden. Email: andreas.stavropoulos@mah.se Funding information
Danish Innovation Foundation
Abstract
Objectives: A considerable portion of the adult population has received and/or is receiving treatment with antiresorptive drugs (ARDs). It is thus relevant to assess possible side effects of ARD intake in connection to various aspects of implant ther‐ apy. The aim of this study was to answer the focused question “In patients with sys‐ temic intake of ARDs, what is the outcome and complication rate of implant therapy including associated bone grafting procedures comparing to patients without sys‐ temic intake of ARDs?”
Materials and Methods: Original studies fulfilled predefined inclusion criteria (e.g., case series, cohort studies, case–control studies, and controlled and/or randomized controlled clinical trials; retro‐ or prospective design; and ≥10 patients with systemic intake of ARDs). Various patient‐, medication‐, and intervention‐related parameters [i.e., implant loss, grafting procedure complication/failure, peri‐implant marginal bone levels/loss, medication‐related osteonecrosis of the jaws (MRONJ), and peri‐ implantitis] were extracted, and meta‐analyses and quality assessment were performed.
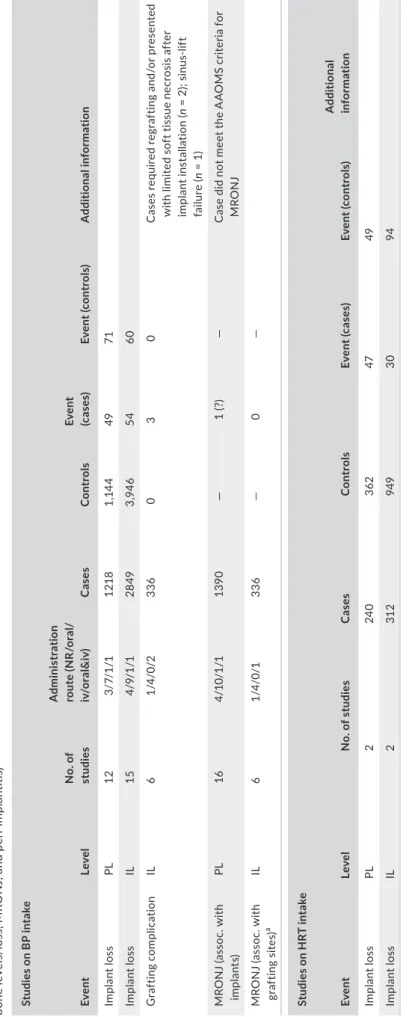
Results: Twenty‐four studies with bisphosphonate (BP) intake (mainly low dose for osteoporosis treatment) and seven studies on hormone replacement therapy (HRT), including ≥10 patients, and controls not taking the medication were identified. Furthermore, seven studies on MRONJ associated with implants were included. Meta‐analyses based on four studies reporting on patient level and eight studies re‐ porting on implant level showed no significant differences in terms of implant loss between patients on BPs (mainly low dose for osteoporosis treatment) and controls. Furthermore, low‐dose BP intake did not compromise peri‐implant marginal bone levels. Based on two studies, no negative effect of HRT was observed on the implant level, while HRT appeared to exert a marginally significant negative effect regarding implant survival on the patient level and regarding peri‐implant marginal bone levels. Based on six studies reporting single‐patient data, MRONJ in patients on BP for os‐ teoporosis appeared in 70% of the cases >36 months after start of drug intake, while in patients with cancer, MRONJ appeared in 64% of the cases ≤36 months after first BP intake.
This is an open access article under the terms of the Creative Commons Attribution‐NonCommercial License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
1 | INTRODUCTION
Drugs counteracting bone resorption, coined antiresorptive drugs (ARDs), interfere with bone metabolism with the aim to decrease abnor‐ mal bone remodeling and/or increased bone resorption. ARDs, despite differences in their mechanisms of action, in general, decrease bone remodeling and resorption by inhibiting differentiation and normal function of osteoclasts (OCLs), and/or increase their apoptosis (Baron, Ferrari, & Russell, 2011). ARDs are thus most commonly/primarily used in the treatment of osteoporosis and primary and metastatic skeletal malignancies, to prevent events such as fractures, and limit pain and metastatic spread; ARDs are also used in less frequent diseases such as Paget’s disease of the bone and osteogenesis imperfecta.
The most widely known ARDs are the bisphosphonates (BPs), a group of drugs introduced >30 years ago. Currently used nitrogen‐ containing BPs (e.g., alendronate, risedronate, ibandronate, pamid‐ ronate, and zoledronate) bind readily to hydroxylapatite and are deposited into the bone. They exert antiresorptive action by inhib‐ iting OCL progenitor development and disturbing OCL function (i.e., recruitment, adhesion, and activity), while also reducing OCL lifes‐ pan; a direct inhibiting effect on osteoblasts has also been suggested (Baron et al., 2011; Stepan, Alenfeld, Boivin, Feyen, & Lakatos, 2003). The administration route influences skeletal uptake of BPs and thus indirectly the dose; specifically, intravenously (iv) administered BPs (e.g., pamidronate and zoledronate) are bound in very large quan‐ tities and are used mainly in the management of malignancies and Paget’s disease of bone, and only in rather limited extent for oste‐ oporosis treatment, while orally administered BPs (e.g., alendronate and risedronate) are bound in significantly smaller quantities (<1% of orally administered BPs is absorbed from the gastrointestinal tract) and are predominantly used in the treatment of osteoporosis and rarely, in some types of cancers, for the prevention of secondary osteoporosis. Relatively recently, another treatment option for os‐ teoporosis has been oral administration of strontium ranelate (SrR),
which—although the exact mechanisms of action are not completely understood—seems to interfere with bone metabolism by decreasing OCL progenitor differentiation and OCL activity, and increasing their apoptosis, while it also increases osteoblast (OB) progenitor differ‐ entiation and OB activity and survival (Bonnelye, Chabadel, Saltel, & Jurdic, 2008; Buehler, Chappuis, Saffar, Tsouderos, & Vignery, 2001). Currently, SrR use appears to be gradually abandoned, because it has been suspected of having a higher risk of adverse cardiovascular events (European Medicines Agency, 2013), although a very recent study did not confirm this (Martín‐Merino et al., 2018).
Treatment of osteopenia and osteoporosis has also been pursued by targeting estrogen deficiency, which is a major cause for these conditions during menopause. Estrogen deficiency upregulates sev‐ eral cytokines, including receptor activator of nuclear factor kappa B ligand (RANKL), while it downregulates others, including osteoprote‐ gerin (OPG). Thus, hormone replacement therapy (HRT) with direct estrogen supplementation exerts its antiresorptive effect predomi‐ nantly through regulating RANKL production by the OB and thereby influencing OCL. Additionally, estrogen has a direct effect on OCL pre‐ cursors by reducing their responsiveness to RANKL and also on OB by stimulating their proliferation and reducing their apoptosis (Stepan et al., 2003). HRT with estrogen is currently prescribed in rather lim‐ ited extent, mostly for the management of climacteric symptoms, due to the risk of adverse cardiovascular events (Wong et al., 2017). A somehow similar treatment approach is the administration of selective estrogen receptors modulators (SERMs; e.g., raloxifene and bazedoxi‐ fene), which are drugs acting on the estrogen receptor and having a se‐ lective estrogenic effect on bone tissue, or by administering calcitonin that binds to its OCL receptor and interferes with normal cell function, including secretion of proteolytic enzymes (Carter & Schipani, 2006).
More recently, a new generation of “biological” ARDs has been introduced based on monoclonal antibodies targeting various mech‐ anisms relevant to bone remodeling. The most widely used is denos‐ umab (Reginster et al., 2014), which is a fully humanized antibody of Conclusion: Low‐dose oral BP intake for osteoporosis treatment, in general, does not compromise implant therapy, that is, patients on ARDs do not lose more implants nor get more implant‐related complications/failures comparing to implant patients with‐ out BP intake. There is almost no information available on the possible effect on im‐ plant therapy of high‐dose BPs or other widely used ARDs (e.g., denosumab), or on the success or safety of bone grafting procedures. Patients with high‐dose ARD in‐ take for management of malignancies, patients on oral BP over a longer period of time, and patients with comorbidities should be considered as high‐risk patients for MRONJ.
K E Y W O R D S
antiresorptive drugs, bisphosphonates, dental implants, hormone replacement therapy, medication‐related osteonecrosis of the jaws, systematic review
RANKL. Denosumab exerts its antiresorptive effect by blocking the binding of RANKL to RANK, and thus interfering with OCL differen‐ tiation, and, in contrast to BPs, does not bind to bone. Denosumab is administered subcutaneously (sc) and in various intervals depend‐ ing on its treatment purpose (i.e., for osteoporosis or malignancies) (Reginster et al., 2014). Recent market analyses estimated about >40% of current osteoporosis treatments are with denosumab (Global Osteoporosis Market & Drugs Analysis 2010–2015, 2011). Similar approaches regard the use of cathepsin K (CatK) inhibitor (odanacatib) and c‐Src kinase inhibitor (saracatinib) or the use of an antisclerostin monoclonal antibody (romosozumab).
In perspective, current estimates indicate that about 15% of the population >50 years of age in the European Union (EU) has osteo‐ porosis; this translates into ca. 23.5 million women and 6.0 million men in the year 2015 and, when considering demographic trends, into ca. 27.5 million women and 7.0 million men in the year 2025 (Hernlund et al., 2013). Despite the fact that consumption may vary significantly among countries/regions, due to differences in prescription rates depending on the regulatory framework and/or treatment uptake, as well as the appearance of newer ARDs (e.g., denosumab), BPs appear still the most prevalent drugs for osteo‐ porosis treatment within the EU. In this context, even if patients with osteoporosis are currently not treated with BPs, the majority has most likely received BPs in the past; based on market shares (Hernlund et al., 2013), it was estimated that oral BPs covered about 70% of osteoporosis treatment in 2010. Thus, as a consider‐ able number of patients attending a dental clinic are suffering from osteoporosis, and a major portion of them has received and/or is receiving treatment with ARDs, it is important to consider possible side effects; specifically, dentoalveolar procedures, including den‐ tal implant and bone augmentation therapies, might be affected by drugs interfering with bone remodeling. In particular, a specific side effect of ARDs associated with dentoalveolar procedures is osteonecrosis of the jaws; this condition, recognized already for more than a decade ago regarding BPs, is characterized by exposed bone or bone that can be probed through an intra‐ or extraoral fis‐ tula in the maxillofacial region and that has persisted for >8 weeks. Currently, the condition is termed “medication‐related osteone‐ crosis of the jaws” (MRONJ), to reflect the fact that similar lesions can be associated with several ARDs and not exclusively with BPs.
Various available reviews on this topic generally agree that still relatively little information is available in regard to possible effects of ARDs on relevant aspects of implant therapy, such as implant failure rate, marginal bone loss, and MRONJ development. Further, there is no comprehensive review regarding the possible effect of ARDs on the failure of grafting procedures and/or on peri‐implanti‐ tis. Thus, the aim of the current review was to systematically assess the literature and perform a meta‐analysis when possible, to answer the following focused question: “In patients with systemic intake of ARDs, what is the outcome of implant therapy in terms of rates of implant loss, failure of grafting procedures, peri‐implant marginal bone levels/loss, MRONJ, and/or peri‐implantitis compared to pa‐ tients without systemic intake of ARDs?”
2 | MATERIAL AND METHODS
2.1 | Protocol and eligibility criteria
The present systematic review was performed following the criteria of the Preferred Reporting Items for Systematic Reviews and Meta‐ analyses (PRISMA; Liberati et al., 2009; Moher, Liberati, Tetzlaff, & Altman, 2009). The literature was systematically searched for origi‐ nal studies fulfilling the following inclusion criteria: (a) English or German language; (b) case series, cohort studies, case–control stud‐ ies, and controlled and/or randomized controlled clinical trials (CTs/ RCTs); (c) retro‐ or prospective design; (d) ≥10 patients with systemic intake of ARDs; (e) clearly reported relevant clinical data (please see data extraction section); and (f) full text available. Studies were ex‐ cluded if (a) not meeting all inclusion criteria; or (b) local application of ARDs.
2.2 | Information sources and literature search
Electronic search was performed in Medline (PubMed), EMBASE (Ovid), and CENTRAL (Ovid)—last search 05/09/2017 and no date restriction used, using relevant search terms (see Appendix 1). Additionally, screening of the reference lists of previous reviews and included full texts and forward search via Science Citation Index of included papers were conducted.2.3 | Data collection and extraction
Two authors (KB, AS) independently checked title, abstract, and finally full text on the predefined eligibility criteria. Studies with abstracts with unclear methodology were included in full‐text as‐ sessment to avoid exclusion of potentially relevant articles. One author (KB) repeated the literature search. In case of ambiguity, con‐ sensus through discussion was achieved regarding the final selection of studies to be included.
From the included studies, one author (KB) extracted twice the following data when available: (a) study design; (b) no. of cases (i.e., patients with ARD intake) and—when available—controls (i.e., sub‐ jects without ARD intake), implants, and grafting procedures; (c) patient characteristics (i.e., systemic diseases/comorbidities, other relevant medication intake, age, gender, and smoking status); (d) in‐ dication for ARD intake, type, and administration details; (e) implant follow‐up time; (f) reported outcome parameters (i.e., implant loss, grafting procedure complication/failure, peri‐implant marginal bone levels/loss, MRONJ, and peri‐implantitis); and (g) MRONJ details (i.e., localization, attributable triggering factor, and time between medication intake or triggering factor and MRONJ development).
2.4 | Synthesis of results—Statistics
Implant loss was defined as the primary outcome parameter; failure of the grafting procedure (i.e., additional need for grafting or pre‐ cluding implant installation), marginal bone loss, MRONJ, and peri‐ implantitis were defined as secondary outcome parameters.
Random‐effects meta‐analyses, separately for each ARD type, were implemented to calculate from the included cohort and case– control studies pooled estimates at the patient and/or implant level. All statistical analyses were performed using Stata (StataCorp LLC, USA).
2.5 | Quality assessment
2.5.1 | Newcastle‐Ottawa‐Scale
Two authors (KB and AS) independently evaluated the methodologi‐ cal and reporting quality of the included studies applying Newcastle‐ Ottawa‐Scale (NOS; Wells et al., 2016), however, with some of the original items modified/adapted to fit the research question herein as follows: (1) selection: (a) selection of controls/nonexposed cohort was awarded with a star, if the controls have been derived from the same office and (b) the item “outcome of interest was not present at start of study” for cohort studies was discarded, as the outcome of interest to include studies in the present review was “implant loss”; (2) comparability: smoking status and/or any augmentation procedure were judged as the most relevant parameters; and (3) exposure: (a) regarding adequate length of follow‐up, if ARD intake started prior to implant installation, then for long‐term outcomes (e.g., late implant loss), ≥5 years was required, while ≤1 year after prosthetic restoration was accepted for short‐term outcomes (e.g., early implant loss); if implant installation occurred before ARD in‐ take, then ≥3 years follow‐up since start of intake was required; (b) the item “nonresponse rate” was not judged for case–control studies if the data were based on medical records only; and (c) the item “ad‐ equacy of follow‐up of cohorts” was not judged for retrospective or cross‐sectional cohort studies. Thus, studies could herein achieve a maximum of 8 or 9 stars; for reasons of comparability, a percentage of awarded stars out of the possible maximum number of stars for each specific study was calculated. Further, the percentage of posi‐ tive scored studies for each specific item was calculated. In case of ambiguity, consensus through discussion was achieved.
2.5.2 | Basic reporting items in Drugs and Implants
A purpose‐made tool containing a list of items considered as neces‐ sary for meaningful reporting of ARD studies in oral implantology was constructed, and studies were assessed for quality of report‐ ing. Three dimensions were defined (a) subject‐, (b) medication‐, and (c) intervention‐related; the various items in each dimension were adapted to each specific ARD group (Appendix 2). Reporting of the various items was judged separately for each cohort of cases and controls, as well as for the cohorts of cases and controls presenting with a complication/event (i.e., implant loss, grafting procedure com‐ plication/failure, peri‐implant marginal bone levels/loss, MRONJ, and peri‐implantitis). The frequency of reported items per study/ cohort as percentage of the total number of items, as well as the percentage of positive scored studies/cohorts for each specific item, was calculated.3 | RESULTS
3.1 | Study selection
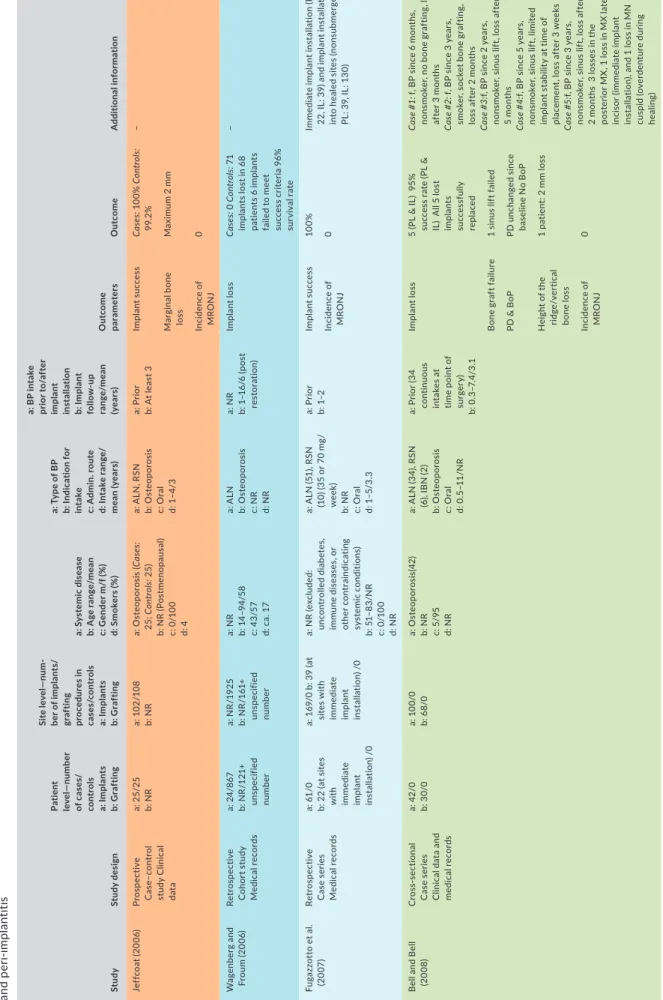
Appendix 3 presents the flowchart of the literature search. Out of 4,093 originally identified studies, 3,815 were excluded based on the title and 221 based on the abstract. Three records from for‐ ward search via the Science Citation Index and no records from reference lists of previous reviews or later included full texts were additionally identified; thus, 60 articles were selected for full‐ text review. Twenty‐four articles were excluded for various rea‐ sons (Appendix 4); finally, 36 articles were included. The included studies were grouped into “studies on BP intake” (n = 24; Table 1) (Al‐Sabbagh, Robinson, Romanos, & Thomas, 2015; Al‐Sabbagh, Thomas, Bhavsar, & De Leeuw, 2015; Bell & Bell, 2008; Bell, Diehl, Bell, & Bell, 2011; Famili, Quigley, & Mosher, 2011; Fugazzotto, Lightfoot, Jaffin, & Kumar, 2007; Goss, Bartold, Sambrook, & Hawker, 2010; Grant, Amenedo, Freeman, & Kraut, 2008; Jeffcoat, 2006; Kasai, Pogrel, & Hossaini, 2009; Khoury & Hidajat, 2016; Koka, Babu, & Norell, 2010; Martin et al., 2010; Memon, Weltman, & Katancik, 2012; Mozzati et al., 2015; Shabestari et al., 2010; Siebert, Jurkovic, Statelova, & Strecha, 2015; Suvarna et al., 2016; Tallarico, Canullo, Xhanari, & Meloni, 2016; Wagenberg & Froum, 2006; Wagenberg, Froum, & Eckert, 2013; Yajima, Munakata, Fuchigami, Sanda, & Kasugai, 2017; Yip, Borrell, Cho, Francisco, & Tarnow, 2012; Zahid, Wang, & Cohen, 2011), “studies on HRT intake” (n = 7; Table 2) (August, Chung, Chang, & Glowacki, 2001; Koka et al., 2010; Koszuta, Grafka, Koszuta, Łopucki, & Szymańska, 2015; Minsk & Polson, 1998; Moy, Medina, Shetty, & Aghaloo, 2005; de Souza et al., 2013; Yip et al., 2012), and “studies on MRONJ associated with implants” (n = 7; Table 3) (Giovannacci et al., 2016; Holzinger et al., 2014; Jacobsen et al., 2013; Kwon et al., 2014; Lazarovici et al., 2010; Pogrel & Ruggiero, 2017; Troeltzsch et al., 2016). Two studies (Koka et al., 2010; Yip et al., 2012) contributed with data on both BP and HRT intake, while two studies (Wagenberg & Froum, 2006; Wagenberg et al., 2013) are based on the same study population. No studies reporting on SERMs, calcitonin, denosumab, SrR, c‐Src, CatK, and sclerostin in‐ hibitors, fulfilling the inclusion criteria, were identified.
3.2 | Study characteristics
Tables 1‒3 present general and more detailed characteristics on (a) study design; (b) no. of cases and controls, implants, and grafting procedures; (c) patients’ characteristics (i.e., relevant systemic dis‐ eases/comorbidities or medication intake, age, gender, and smoking status); (d) indication for type and administration details of ARD; (e) implant follow‐up time; (f) reported outcome parameters (i.e., implant loss, grafting procedure complication/failure, peri‐implant marginal bone levels/loss, MRONJ, and peri‐implantitis); and (g) MRONJ details of included studies. Table 4 presents a summary of studies reporting exact figures (numbers) on the above‐mentioned outcome parameters.
T A B LE 1 C ha ra ct er is tic s o f i nc lu de d s tu di es r ep or tin g o n t he e ff ec t o f B P i nt ak e o n i m pl an t l os s, g ra ft in g p ro ce du re c om pl ic at io n/ fa ilu re , p er i‐i m pl an t m ar gi na l b on e l ev el s/ lo ss , M RO N J, an d p er i‐i mp lan tit is St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion Je ff co at ( 20 06) Pros pe ct iv e C as e– con tr ol st ud y C lin ic al dat a a: 2 5/ 25 b: N R a: 10 2/ 10 8 b: N R a: O st eo po ro si s ( Ca se s: 25 ; C ontr ol s: 2 5) b: N R ( Po st m en op au sa l) c: 0 /1 00 d: 4 a: A LN , R SN b: O st eo po ro si s c: O ra l d: 1– 4/ 3 a: P rio r b: A t l ea st 3 Im pla nt s uc ce ss Ca se s: 10 0% C ontr ol s: 99. 2% – Mar gi na l b on e los s M ax im um 2 m m Inc idenc e o f M RO N J 0 W ag en be rg a nd Fr ou m ( 20 06) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s a: 2 4/ 86 7 b: N R /1 21 + uns pe cif ie d nu m be r a: N R /1 92 5 b: N R /1 61 + uns pe cif ie d nu m be r a: N R b: 1 4– 94 /5 8 c: 4 3/ 57 d: c a. 1 7 a: A LN b: O st eo po ro si s c: N R d: N R a: N R b: 1 –1 6/ 6 ( po st re st or at ion ) Im pla nt lo ss Ca se s: 0 Co ntr ol s: 7 1 im pl an ts l os t i n 6 8 pa tie nt s 6 i m pl an ts fa ile d t o m ee t su cc es s c rit er ia 9 6% su rv ival ra te – Fu ga zz ot to e t a l. (2 007 ) Ret ros pe ct iv e C as e s er ie s M edic al re co rd s a: 6 1/ 0 b: 2 2 ( at s ite s w ith im m ed iate im pla nt ins ta lla tio n) / 0 a: 1 69 /0 b : 3 9 ( at si te s w ith im m ed iate im pla nt ins ta lla tio n) / 0 a: N R ( ex cl ud ed : un con tr ol le d d iab et es , imm une d ise ase s, o r ot he r c on tr ain dic at in g sy st emic c on di tio ns ) b: 5 1– 83 /N R c: 0 /1 00 d: N R a: A LN ( 51 ), R SN (1 0) ( 35 o r 7 0 m g/ w ee k) b: N R c: O ra l d: 1– 5/ 3. 3 a: P rio r b: 1– 2 Im pla nt s uc ce ss 10 0% Im m ed iate im pl ant in st al lat io n ( PL : 22 , I L: 3 9) a nd i m pl an t i ns ta lla tio n in to h ea le d s ite s ( no ns ub m er ge d; PL : 3 9, I L: 1 30 ) Inc idenc e o f M RO N J 0 B el l a nd B el l (2 00 8) C ros s‐ se ct io na l C as e s er ie s C lin ic al d at a a nd m edic al re co rd s a: 4 2/ 0 b: 3 0/ 0 a: 1 00 /0 b: 6 8/0 a: O st eo po ro si s( 42 ) b: N R c: 5 /9 5 d: N R a: A LN ( 34 ), R SN (6) , I B N ( 2) b: O st eo po ro si s c: O ra l d: 0 .5 –1 1/ N R a: P rio r ( 34 co nt in uo us in ta ke s a t tim e p oi nt o f su rg er y) b: 0 .3 –7 .4 /3 .1 Im pla nt lo ss 5 ( PL & I L) 9 5% su cc es s r at e ( PL & IL ) A ll 5 l os t im pla nt s su cc es sf ull y repl ac ed Ca se # 1: f, B P s in ce 6 m on th s, no ns m ok er , n o b on e g ra ft in g, l os s af te r 3 m on th s Ca se # 2: f, B P s in ce 3 y ea rs , sm ok er , s oc ke t b on e g ra ft in g, lo ss a ft er 2 m on th s Ca se # 3: f, B P s in ce 2 y ea rs , no ns m ok er , s in us l if t, l os s a ft er 5 m on th s Ca se # 4: f, B P s in ce 5 y ea rs , no ns m ok er , s in us l if t, l im ite d im pl an t s ta bi lit y a t t im e o f pl ac emen t, l os s a ft er 3 w eek s Ca se # 5: f, B P s in ce 3 y ea rs , no ns m ok er , s in us l if t, l os s a ft er 2 m on th s 3 l os se s i n t he po st er io r M X , 1 l os s i n M X l at er al in ci so r (im m edi at e i m pla nt in st al la tio n) , a nd 1 l os s i n M N cu sp id (o ve rd en tu re d ur in g he al ing ) B on e gr af t f ai lu re 1 s in us l if t f ai le d PD & B oP PD u nc ha ng ed s in ce ba sel ine N o B oP H ei gh t o f t he ridg e/ ve rt ic al bo ne lo ss 1 p at ie nt : 2 m m l os s Inc idenc e o f M RO N J 0 (C on tinues )
T A B LE 1 (Co nti nue d) St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion G ra nt e t a l. (2 00 8) C ros s‐ se ct io na l C oh or t s tu dy Q ue st io nn ai re and p ar tly cli ni ca l d at a a: 1 15 /3 43 b: 32 /N R a: 4 68 /1 45 0 b: 32 /N R a: N R b: > 40 /N R c: 0 /1 00 d: N R Ca se s: a: D ia be te s ( 2) , Pr ed ni so lo ne i nt ak e ( 3) b: N R /6 7. 4 c: 0 /1 00 d: N R a: P rio r: A LN ( 66) , RS N ( 21 ), I B N ( 2) A ft er : N R b: N R c: O ra l d: N R /3 .2 a: P rio r (3 3 > 3 ye ar s, 56 < 3 y ea rs ) an d a ft er ( 26) b: N R Im pla nt s uc ce ss Ca se s: 2 l os se s ( IL an d P L; b ot h d ue t o no no ss eo in teg ra ‐ tio n, o ne su cc es sf ull y repl ac ed ) Co ntr ol s:1 4 lo sse s Ca se # 1: M X p re m ol ar , B P s in ce >3 y ea rs b ut n ot a ny m or e a t t im e po in t o f s ur ge ry o r t he re af te r Ca se # 2: M N m ol ar , B P s in ce >4 y ea rs Inc idenc e o f M RO N J 0 K as ai e t a l. (2 00 9) Ret ros pe ct iv e C as e– con tr ol st ud y M ed ic al re co rds a: 1 1/ 40 b: N R a: 3 5/ 16 1 b: N R a: O st eo po ro si s (C as es: 11 , C ontr ol s: 4 ) (ex clu de d: u nc on tr ol le d di ab et es , r he um at ic di se as e u nd er c or tic oi d m edic at io n) b: > 3 6/ N R; Ca se s: 5 2–7 3 c: 0 /1 00 d: 0 a: A LN b: O st eo po ro si s c: O ra l d: A t l ea st 3 /N R a: P rio r b: Ca se s: 5. 3–1 2. 2/ 7 Im pl an t l os s/ su cce ss Ca se s: 5 l os se s i n 3 pat ie nt s/ 85 .7 % su cc es s r at e Co ntr ol s: 7 lo sse s/ 95 .7 % su cc es s r ate Ca se # 1: 2 l os se s i n t he a nt er io r M X ( la ck o f i nt eg ra tio n) Ca se # 2: 2 l os se s i n p os te rio r M N (a ft er 3 3 m on th s) Ca se # 3: 1 l os s i n t he a nt er io r M X (a ft er 1 1 m on th s) Inc idenc e o f M RO N J 0 G os s e t a l. (2 010 ) Ret ros pe ct iv e C oh or t s tu dy Q ue st io nn ai re am on g den tis ts an d m ed ic al re co rds a: 5% /c a. 1 6 000 b: NR‐ a: N R /c a. 2 8 0 00 b: N R a: N R b: N R c: N R d: N R Ca se s w ith a l os s: a: O st eo po ro si s ( 6) , os te op oros is & di ab et es + s te ro id in ta ke ( 1) b: 4 9– 75 /6 5. 7 c: 2 9/ 71 d: N R a: N R b: N R c: N R d: N R Ca se s w ith a l os s: a: A LN ( 4) , R SN ( 2) , A LN & RS N ( 1) b: O st eo po ro si s c: O ra l d: 3 –1 0/ 5. 2 ( 3) , 0 .2 5 (1 ), 5 ( 2) , 5 .2 ( 1) a: N R b: N R Ca se s w ith a l os s: a, b : 3 l os se s du e t o no no ss eo inte ‐ gr at io n ( B P in ta ke p rio r t o im pla nt ins ta lla tio n) ; 6 lo ss es a ft er su cc ess ful inte gr at io n f or 1. 5– 20 y ea rs (B P i nt ak e af te r i m pl an t ins ta lla tio n) Im pla nt lo ss 7 ( PL ) a nd 9 ( IL ) Fa ilu re r at e 0 .8 9% (P L) – m ( 2) /f ( 5) , m ea n a ge : 6 5. 7 ( ra ng e: 49 –7 5) ; 1 w ith s te ro id s a nd di ab ete s Inc idenc e o f M RO N J A m on g t he 7 p at ie nt s w ith a n i m pl an t lo ss , 5 h av e b ee n re po rt ed w ith lo ca liz ed t o ex te ns iv e O N J K ok a e t a l. (2 010 ) Ret ros pe ct iv e C as e– con tr ol st ud y ( ?) M ed ic al re co rd s a nd inte rv ie w a: 5 5/ 82 b: N R a: 1 21 /1 66 b: N R Ca se s: a: D ia be te s ( 10 ), H RT (e st rog en ; 3 1) , s te ro ids (5 ) b: 5 0– 93 /7 1 c: 0 /1 00 d: 4 Contr ol s: a: D ia be te s ( 8) , H RT (e st rog en ; 4 8) , s te ro id s (5 ) b: 5 0– 89 /6 6 c: 0 /1 00 d: 11 a: N R b: O st eo po ro si s (3 2) , O st eo pe ni a (18 ), o r n ot sp ec ifi ed (5 ) c: N R d: <3 ( 16) , 3 –5 ( 20 ), >5 ( 19 ) / N R a: P rio r b: N R Im pla nt lo ss Ca se s: 1 l os s/ 99 .2 % su cc es s r at e ( IL ) Co ntr ol s: 3 l os se s i n 2 p at ie nt s/ 98 .2 % su cc es s r at e ( IL ) C as e ( 1) : 8 2 ye ar s, n on sm ok er , ad dit io na l H RT , os te op oros is , A LN ( 70 m g/ w ee k) f or 6 y ea rs C on tr ol s ( 2) : 6 5/ 76 y ea rs , 1 sm ok er , b ot h H RT Inc idenc e o f M RO N J 0 (C on tinues )
St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion M ar tin e t a l. (2 010 ) C ros s‐ se ct io na l C as e s er ie s Q ue st io nn ai re and p ar tly m edic al re co rd s a: 5 89 /0 b: N R /0 a: N R /0 b: N R /0 a: N R b: N R c: N R d: N R Pa tie nt s w ith i m pl an t los se s: a: S te ro id s ( 1) , n o di ab et es b: N R /7 0 c: 0 /1 00 d: 2 c ur re nt , 3 f or m er sm ok er s ( n) a: A LN (9 5% ), R SN , IB N b: Pa tie nt s w ith im pl ant los se s: O st eop or os is or os te op oro tic fr ac tu re pr ev ent io n c: O ra l d: > 1/ N R a: P rio r a nd af te r b: N R Im pla nt lo ss 16 ( PL ) 2 6 ( IL ) 4 w ee ks t o 1 1 ye ar s af te r i ns ta lla tio n Ea rly l os se s: 8 P L/ 8 IL L at e l os se s: 1 0 PL /18 I L (2 p at ie nt s ha d b ot h e ar ly a nd la te l os se s) Im m ed ia te ( 1) a nd de la ye d ( 15 ) pl ac emen t Pa tie nt s w ith l os se s: a ll A LN d ue t o os te op or os is f or 3 –6 9 m on th s pr io r ( 12 ) a nd a ft er ( 4) i m pl an t in st al la tio n, s m ok er s ( 2) , f or m er sm ok er s ( 3) , a nd s te ro id s ( 1) M X (8 P L/ 12 I L) : 3 a nt er io r, 9 po st er io r M N (9 P L/ 14 I L) : 5 ante rio r, 9 p os te rio r Inc idenc e o f M RO N J 0 ( am on g t he i m pl an t lo ss es ) 1 p at ie nt (s m ok er ; 4 l os se s i n th e a nt er io r M N 4 ye ar s a ft er pl ac emen t; i m pl an ts pl ac ed 5 m on th s af te r b eg in ni ng o f AL N tr ea tm en t) : os te om ye lit is a nd ex te ns iv e b on e ne cr osi s su rr ou nd ing th e im pla nt s Sh ab es ta ri e t a l. (2 010 ) C ros s‐ se ct io na l C as e s er ie s C lin ic al d at a a: 2 1/ 0 b: 5/ 0 a: 4 6/ 0 b: N R /0 a: E xc lu de d: d ia be te s, im m un e de fic ienc y b: 4 2– 79 /5 3 c: 0 /1 00 d: N R a: A LN ( 35 –7 0 m g/ w ee k) b: O st eo po ro si s c: O ra l d: 1 .7/ N R a: P rio r ( 7) a nd af te r ( 14 ) b: 4 .2 /0 .6 –8 .1 Im pla nt lo ss 0 – Inc idenc e o f per i‐i m pl an tit is 0 6 .3 % s ho w ed 3 expo sed th re ad s B el l e t a l. ( 20 11 ) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s a: i n t ot al : 6 55 b: N R /r ep or te d bu t w ith ou t sp ec ifi c nu m be rs a: 2 4/ 89 8 b: N R /r ep or te d bu t w ith ou t sp ec ifi c nu m be rs a: N R b: N R /c a. 5 9 c: C a. 4 2/ 58 d: C a. 1 3 a: N R b: N R c: N R d: N R a: N R b: 0 .2 5–7 .7 5/ 1. 6 Im pla nt lo ss Ca se s: 0 Co ntr ol s:1 5 (a ft er 1 –1 0 m on th s) – T A B LE 1 (Co nti nue d) (C on tinues )
St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion Fa m ili e t a l. (2 011 ) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s a: 2 2/ 98 b: N R a: 7 5/ 27 2 b: N R a: O st eo po ro si s (C as es: 2 2, Co ntr ol s: 5 ), os te oa rt hr iti s ( 1) b: > 50 /N R c: 0 /1 00 d: N R a: A LN ( 15 ), R SN (4 ), I B N (1 ), A LN an d I B N ( 2) b: O st eo po ro si s c: O ra l d: 0 .5 –1 ( 6) , 1 –5 (9 ), >5 ( 5) , u nk no w n (2 ) / N R a: N R b: N R Im pla nt lo ss Ca se s: 1 a t se co nd‐ st ag e su rg er y ( PL a nd I L; su cc es sf ull y repl ac ed ) Ca se s: 98 .7 % s uc ce ss r at e (IL ) – Inc idenc e o f M RO N J 0 Za hi d e t a l. (2 011 ) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s a: 2 6/ 27 4 b: N R a: 5 1/ 61 0 b: i n t ot al 1 73 a: O st eo po ro si s ( 8% o f th e s tu dy p op ul at io n) b: 1 7– 87 /5 6 c: 3 7/ 63 d: 9 a: A LN , I B N b: O st eo po ro si s c: N R d: 0 .5 –1 6 ( 11 n ot av ai lab le ) / NR a: P rio r b: 0 .17 –6 .5 /2 .17 Im pla nt lo ss 19 i n t ot al ( su cc es s ra te 9 7. 1% ) 3 im pl an ts i n c as es [s uc ce ss r at e: 9 4. 1% (IL ) / 88 .5% ( PL )] Lo ss es i n t ot al : a nt er io r ( 2) , po st er io r (17 ) Lo ss es i n c as es : Ca se # 1: 7 2 ye ar s, f , 1 st M N ‐m ol ar , A LN ( 70 m g p er w ee k fo r u nk no w n p er io d) , l os s a ft er 7 w eek s, s uc ce ss fu l r epl ac ed Ca se # 2: 7 5 ye ar s, f , M N c an in e, IB N ( 15 0 m g p er m on th f or un kn ow n p er io d) , l os s a ft er 8 w eek s, s uc ce ss fu l r epl ac ed Ca se # 3: 7 5 ye ar s, f , i m m ed ia te im pl an t a t 2 nd M X‐ pr em ol ar , A LN si nc e 4 y ea rs , n o i ni tia l s ta bi lit y, lo ss a ft er 4 w eek s, no t r epl ac ed Mar gi na l b on e los s In t ot al : 7 1 i m pl an ts w ith “ 1– 8 t hr ea d ex pos ure ” Ca se s: 13 i m pl an ts w ith “t hre ad e xp os ure ” ou t o f 5 1 O R 3 .3 w ith B P u se Inc idenc e o f M RO N J 0 M em on e t a l. (2 012 ) Ret ros pe ct iv e C as e– con tr ol st ud y M ed ic al re co rds a: 10 0/ 10 0 b: N R a: 1 53 /1 32 b: c a. 44 / ca . 4 4 Ca se s: a: D ia be te s ( 3) b: 4 6– 91 /6 6 c: 0 /1 00 d: 3 Contr ol s: a: D ia be te s ( 4) b: 4 7– 90 /6 3 c: 0 /1 00 d: 5 a: A LN ( 72 ) R SN (2 3) , I B N ( 5) b: O st eo po ro si s c: O ra l d: < 1 ( 20 ), 1 –3 ( 19 ), >3 ( 15 ), un sp ec ifi ed ( 46) / NR a: P rio r b: U nt il st age ‐t wo su rg er y 4– 6 m on th s Ea rly im pla nt lo ss / Im pla nt s uc ce ss Ca se s: 1 0 l os se s ( IL ) /9 3. 5% s uc ce ss r at e Co ntr ol s: 6 l os se s (IL ) / 95 .5% s uc ce ss rate Im pl an t l os se s: A LN ( 6) , R SN ( 1) , an d I B N ( 3) Mar gi na l b on e le ve l(a ss es se d i n a f ra ct io n o f t he st ud y p op ulat io n 4– 6 m on th s po st ‐o p a t se co nd ‐s ta ge su rg er y) Ca se s: 0 .8 7 m m Co nt ro ls : 0 .9 2 m m No d iff er enc e be tw ee n g ro up s N o ef fe ct o f B P t yp e an d dur at ion in tak e N o e ff ec t o f im pl ant lo cat io n W ag en ber g et a l. ( 20 13 ) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s a: N R /5 41 b: N R /1 21 + uns pe cif ie d nu m be r a: 3 5/ 11 51 b: N R /1 61 + uns pe cif ie d nu m be r a: N R b: 1 2– 88 /5 9 c: 4 3/ 57 d: c a. 1 5 a: A LN b: O st eo po ro si s c: N R d: N R a: N R b: 1 –22/ 10 Mar gi na l b on e los s Ca se s: 0 .6 1 m m Co ntr ol s: 0 .5 3 m m O ve ra ll: 0 .5 2 m m , <1 .5 m m i n 9 0% (IL ), > 3 m m i n 2 .5% (IL ) N o s ig ni fic an t e ff ec t o f B P i nt ak e T A B LE 1 (Co nti nue d) (C on tinues )
St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion Y ip e t a l. ( 20 12 ) Ret ros pe ct iv e C as e– con tr ol st ud y M ed ic al re co rds a: 2 0/ 31 7 b: N R a: i n t ot al 1 181 b: N R a: H RT ( 36) , d ia be te s ( 20 ), th yro id d is ord er s, ca rdi ov as cula r di se as es b: ≥ 40 /5 7 c: 0 /1 00 d: 1 5 a: A LN , R SN b: O st eo po ro si s c: O ra l d: N R a: N R b: 0 .3 –1 1. 9/ 6 Im pla nt lo ss O R 2 .7 o f B P u se f or im pl an t l os s C as es w er e m or e l ik el y or al B P u se rs (9 .7 % ) th an c on tr ol s ( 4. 0% ; p = 0.0 4) No s ig ni fic an t i nt er ac tio n b et w een B P u se a nd i m pl an t l oc at io n St ra tif ie d a na ly se s: as so ci at io n be tw ee n B P u se a nd i m pl an t l os s w as s tr on ge r a nd s ig ni fic an t i n M X ( ad ju st ed O R 2 .6 ; 9 5% C I 1. 4– 5. 0) , w hi le o f l es s m ag ni tu de an d n on si gn ifi ca nt i n M N (a dj us te d O R 1 .4 ; 9 5% C I 0.5 – 3 .7) A l‐S ab bagh , Th om as , e t a l. (2 01 5) C ros s‐ se ct io na l C oh or t s tu dy Inte rv ie w a: 3 9/ 37 6 b: N R a: i n t ot al : 9 63 b: N R a: O st eo po ro si s (C as es: 3 9, C ontr ol s: 2 0) , di ab et es ( 43 ) b: N R /5 9. 4 c: 4 2/ 58 d: 11 .1 a: N R b: O st eo po ro si s c: N R d: N R a: N R b: N R /6 Im pla nt s uc ce ss 84 .9 % s uc ce ss ( PL ) N o e ff ec t o f B P ( PL ) 89 .4 % s uc ce ss ( IL ) N o u se o f B P ( O R 9. 22 ; 9 5% C I, 1 .8 49 , 45 .9 75 ) a ss oc ia te d w ith p oo r i m pl an t ou tc om e ( IL ) Ca se s: 35 ( 89 .7 % ) s uc ce ss , 4 ( 10 .3 % ) f ai lu re (P L) Co ntr ol s: 318 (8 4. 6% ) s uc ce ss , 5 8 (1 5. 4% ) f ai lu re ( PL ) – Im pl an t l os s 10 ( 2. 4% ; P L) 2 5 (2 .6 % ; I L) Inc idenc e o f M RO N J 0 A l‐S ab bagh , Ro bin so n, et a l. ( 20 15 ) C ros s‐ se ct io na l C oh or t s tu dy Inte rv ie w a: 2 0/ 18 3 b: N R a: 4 6/ 46 9 b: N R a: O st eo po ro si s (C as es: 2 0, Co ntr ol s: 9) b: 2 1– 90 /5 5. 5 c: 4 1/ 59 d: Ca se s: 0 a: N R b: O st eo po ro si s c: O ra l d: ≥ 3 a: N R b: 0. 84 –1 0/ 7.0 5 Im pl an t f ai lu re 0 – Inc idenc e o f M RO N J 0 T A B LE 1 (Co nti nue d) (C on tinues )
St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion M oz za ti e t a l. (2 01 5) Ret ros pe ct iv e C as e s er ie s M edic al re co rd s a: 2 35 /0 b: N R /0 a: 1 26 7/ 0 b: 5 4/0 a: D ia be te s ( 21 ), C or tic os te ro ids (2 4) b: 4 8– 79 /6 1 c: 0 /1 00 d: 2 2 a: A LN ( 14 1) , R SN (4 5) , I B N ( 68 ) b: O st eo po ro si s c: O ra l d: 0 .6 –7 .3 /3 .4 a: P rio r b: M in im um 2 , up t o 1 0 Im pla nt lo ss ‐ 1 6 I L/ 15 P L S uc ce ss ra te : 9 8. 7% ( IL ) /9 3. 2% ( PL ) A ll l os t 1– 3 m on th s a ft er su rg er y A ll su cc es sf ull y repl ac ed Im pl ant los se s: 5 1– 77 y ea rs o ld , sm ok er s (9 ), 3 d ia be te s ( 3) , co rt ic os te ro id s ( 3) , A LN ( 6) , R SN (5 ), I B N ( 4) , B P i nt ak e 2– 82 m on th s, M X a nt er io r ( 3) / po st er io r (9 ), M N a nt er io r ( 2) / po st er io r ( 2) , i m m ed ia te l oa di ng (1 ),s in us l if t ( 7) , a nd i m m ed ia te pl ac em en t (9 ) S ig ni fic an t r is k fa ct or s: R SN , d ia be te s, co rt ic os te ro ids , a nd s m ok in g Inc idenc e o f M RO N J 0 Si eb er t e t a l. (2 01 5) Pros pe ct iv e C as e– con tr ol st ud y ( ?) C lin ic al dat a a: 1 2/ 12 b: N R a: 6 0/ 60 b: N R a: N on e ( ex cl ud ed : st ero ids ) b: > 54 c: 0 /1 00 d: 0 a: Z LN ( 5 m g o nc e pe r y ea r) b: O st eo po ro si s c: i v d: 2– 3 a: P rio r b: 1 Im pl an t s ur vi val 10 0% A ll i m pla nt s im m edi at e im pla nt in st al la tio n i n t he a nt er io r M N Inc idenc e o f M RO N J 0 K ho ur y & H id aj at (20 16 ) Ret ros pe ct iv e C as e s er ie s M edic al re co rd s a: 1 5/ 0 b: 1 5/ 0 a: 7 1/ 0 b: 6 1/ 0 a: O st eo po ro si s ( 15 ) b: 5 5– 72 /N R c: 0 /1 00 d: 0 a: O ra l: A LN , R SN , IB N , C LN i v: I B N b: O st eo po ro si s c: O ra l a nd i v d: 0 .2 5–1 0/ N R a: P rio r b: 3 –6 Im pla nt lo ss ‐ 1 ( im m ed ia te ly lo ad ed ; a ft er 5 m on th s) , su cc es sf ull y repl ac ed Im pla nt s in se rt ed s im ult an eo us ly (2 8) o r 3 m on th s a ft er au gm en ta tio n ( 43 ), s ec on d‐ st ag e su rg er ie s a ft er 3 m on th s a nd pros th et ic re st or at io ns a ft er 4– 8 w ee ks Mar gi na l b on e los s N o m aj or b on e l os s No p er i‐i m pl an titi s Inc idenc e o f M RO N J 0 O ut co m e gr af ting In co m pl et e h eal ing of t he g ra ft ed b on e an d n ec es si ty o f re gr af ting d ur ing im pla nt in st al la tio n (2 ) L im ite d s of t tis su e n ec ro si s a ft er im pla nt in st al la tio n (2 ) U ne ve nt fu l he al in g a t d on or si te s T A B LE 1 (Co nti nue d) (C on tinues )
St udy St ud y d es ig n Pa ti en t le ve l—n um be r of c ase s/ con tr ol s a: I m pl an ts b: G ra ft in g Si te le ve l— num ‐ ber o f i mp lan ts / gr af ti ng pr oc edu res in ca se s/ con tr ol s a: I m pl an ts b: G ra ft in g a: S ys te m ic d is ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: T yp e o f B P b: I nd ic at io n f or in ta ke c: A dm in . r ou te d: I nt ak e r an ge / m ean (y ear s) a: B P i nt ak e pr io r t o/ af te r im pla nt ins ta lla ti on b: I m pl an t fo llo w ‐u p ran ge /m ean (ye ar s) O ut come par am et er s O ut come A dd it iona l i nf or m at ion Su va rn a e t a l. (2 016 ) Ret ros pe ct iv e C as e s er ie s M edic al re co rd s a: 1 12 /0 b: 5 5/ 0 a: 1 40 /0 b: 82 /0 a: N R b: N R c: 3 0/ 82 d: N R a: A LN ( 40 ), R SN (1 0) , I B N ( 8) b: N R c: N R d: N R a: P rio r b: M in im um o f 3 Im pla nt lo ss 10 ( IL a nd P L) Su cc es s r at e 9 2. 9% 3 l os se s w ith in 1 m on th , 2 l os se s w ith in 2 m on th s, 2 los se s w ithi n 6 m on th s, a nd 3 los se s w ithi n 3 w ee ks Im pl an t l os se s: 8 i n f ( 3 p at ie nt s: sm ok er s, b on e g ra ft in g; 2 pa tie nt s: B P s in ce 1 y ea r, no ns m ok er s, s in us l if t; 3 p at ie nt s: B P s in ce 3 y ea rs , s m ok er s, s in us lif t) , 2 i n m ( B P s in ce 5 m on th s, no ns m ok er s, n o b on e g ra ft in g) , 70 % i n p os te rio r M X Mar gi na l b on e los s 0 Inc idenc e o f M RO N J 0 Ta lla ric o e t a l. (2 016 ) Pr os pe ct iv e C as e se rie s C lin ic al dat a a: 3 2/ 0 b: N R /0 a: 9 8/ 0 b: N R /0 a: N R b: 4 6– 80 /6 5 c: 0 /1 00 d: n o “ he av y s m ok er s (> 10 c ig ar et te s/ day )” a: A LN ( 70 m g p er w ee k) b: O st eo po ro si s c: O ra l d: >3 /N R a: P rio r ( at l ea st 3 ye ar s, b ut dr ug h ol id ay s fo r 6 m on th s be fo re a nd 4– 6 m on th s af te r i m pl an t ins ta lla tio n) b: 3 –6 /4 Im pl an t s ur vi val 1 i m pl an t l os s 9 9% su rv iv al r at e a ft er 3 ye ar s Im pl an t l os s o cc ur re d b ef or e pr os th et ic r es to ra tio n a nd i n M X Mar gi na l b on e los s m ea n: 1 .3 5 m m ( af te r 3 ye ar s) Ya jim a e t a l. (2 017 ) Ret ros pe ct iv e C oh or t s tu dy M edic al re co rd s (?) a: 1 1/ 14 b: N R a: 2 5/ 28 b: N R a: O st eo po ro si s (C as es: 11 , C ontr ol s: 14 ) (e xc lu de d: s te ro id s a nd di ab et es ) C on tr ol s: 8 SE RM a nd 6 P TH i nt ak e b: Ca se s: > 60 / 70 ; Co ntr ol s: > 60 / 67 c: 0 /1 00 d: 0 a: A LN b: O st eo po ro si s c: O ra l d: 1 –3 ( 5) , > 3 ( 6) a: P rio r b: Ca se s: 3 .2 ; Co ntr ol s: 5. 2 Im pla nt lo ss Ca se s: 3 ( IL & P L) w ith in 1 y ea r C on tr ol s: 0 Ca se # 1: 6 8 ye ar s, f , m ol ar ( M N ), B P s in ce 1 y ea r C as e # 2: 6 7 ye ar s, f, p re m ol ar ( M N ), B P s in ce 4 y ea rs Ca se # 3: 7 5 ye ar s, f , m ol ar ( M N ), B P s in ce 5 y ea rs Inc idenc e o f M RO N J 0 N ote s. , r et ro sp ec tiv e c as e s er ie s; , c ro ss ‐s ec tio na l c as e s er ie s; , p ro sp ec tiv e c as e s er ie s; , r et ro sp ec tiv e c oh or t s tu dy ; , c ro ss ‐se ct io na l c oh or t s tu dy; , pr os pe ct iv e c oh or t s tu dy; , r et ro sp ec tiv e c as e–c on tr ol s tu dy ; , c ro ss ‐se ct io na l c ase –c on tr ol s tu dy; , p ro sp ec tiv e c as e–c on tr ol s tu dy . A LN , a le nd ro na te ; B oP , b le ed in g o n p ro bi ng ; B P, b is ph os ph on at e; C LN , c lo dr on at e; C I, c on fid en ce i nt er va l; f , f em al e; H RT , h or m on e r ep la ce m en t t he ra py ; I B N , i ba nd ro na te ; I L, i m pl an t l ev el ; i v, i nt ra ve no us ; m , m al e; M N , m an di bl e; M RO N J, m ed ic at io n‐ re la te d o st eo ne cr os is o f t he j aw ; M X , m ax ill a; N R , n ot r ep or te d; O R , o dd s r at io ; P D , p ro bi ng p oc ke t d ep th ; P L, p at ie nt l ev el ; P TH , p ar at hy ro id h or m on e; R SN , ris ed ro na te ; S ER M , s el ec tiv e e st ro ge n r ec ep to r m od ul at or ; Z LN , z ol ed ro na te . In co ns is te nc ie s i n t he n um be rs a m on g t he c ol um ns i n t hi s t ab le a re d ue t o i nc on si st en ci es i n t he o rig in al p ap er s. T A B LE 1 (Co nti nue d)
T A B LE 2 C ha ra ct er is tic s o f i nc lu de d s tu di es r ep or tin g o n t he e ff ec t o f H RT i nt ak e o n i m pl an t l os s, g ra ft in g p ro ce du re c om pl ic at io n/ fa ilu re , p er i‐i m pl an t m ar gi na l b on e l ev el s/ lo ss , M RO N J, an d p er i‐i mp lan tit is St ud y Stu dy d esig n Pa tie nt le ve l—n um be r of c as es / con tr ol s a: I m pl an ts b: G ra ft in g Si te l ev el — nu m be r o f im pla nt s/ gr af tin g pr oc edu res in ca se s/ co nt ro ls a: I m pl an ts b: G ra ft in g a: S ys te m ic dis ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: H RT p ro du ct de ta ils (c on te nt , do sa ge) b: I nd ic at io n f or H RT i nt ak e c: A dmini st ra tio n ro ut e d: D ur at io n ran ge /m ean (ye ar s) a: H RT i nt ak e pr io r t o/ af te r im pla nt in st al la tion b: I m pl an t fol lo w ‐u p r an ge / m ean (y ear s) O ut co m e par am et er s O utc om e A dd iti ona l in for ma tion M in sk a nd P ol so n (19 98 ) Re tros pe ct iv e Co ho rt s tud y M edic al re co rds a: 2 5/ 91 b: N R a: 7 1/ 37 9 b: N R a: E xc lu de d: s te ro id s, me ta bo lic d iso rder s b: 5 1– 91 /N R c: 0 /1 00 d: Ca se s: 22 imp lan ts ; Co ntr ol s: 1 04 im pla nt s a: N R b: N R c: N R d: N R a: P rio r b: N R Imp lan t lo ss Ca se s: 8 ( 11 .3 % ; IL ) Co ntr ol s: 2 8 (7 .4 % ; I L) O nl y ea rly fa ilu re s Sm oki ng ap pe ar ed t o si gn ific an tly in cre as e t he fa ilu re r at e am on g c ase s A ug us t e t a l. (2 00 1) Re tros pe ct iv e Co ho rt s tud y M edic al re co rds a: 7 5/ 16 8 b: 0 a: 2 41 /5 70 b: 0 a: E xc lu de d: c on cu rr en t ill ne ss , m et ab ol ic b one di se as e, B P, o r ra lo xi fe ne in ta ke b: Ca se s:3 3–7 9; Co ntr ol s: 5 0–9 6 c: 0 /1 00 d: 0 a: E st ro ge n b: O st eop or os is c: N R d: N R a: P rio r b: U nt il i m pl an t ex po su re Imp lan t lo ss Ca se s: 2 2 ( 9. 1% ; IL ) Co ntr ol s: 6 6 (1 1. 6% ; IL ) — M oy e t a l. ( 20 05 ) Re tros pe ct iv e Co ho rt s tud y M edic al re co rds a: 1 61 /3 04 b: N R a: N R b: N R a: N R b: 1 2– 94 /N R c: 4 1/ 59 d: N R a: E st ro ge n b: N R c: N R d: N R a: P rio r b: U p t o 2 0 Imp lan t lo ss Ca se s: 4 4 ( 27 .3 % ; PL ) C ontr ol s: 49 (1 6. 1% ; P L) H RT : RR 2 .5 5 f or im pla nt fa ilu re (c ompar ed to he al th y pat ie nt s) ‐ K ok a e t a l. ( 20 10 ) Re tros pe ct iv e C ase –c on tr ol st ud y ( ?) M edic al re co rds & inte rv ie w a: 7 9/ 58 b: N R a: i n t ot al 2 87 b: N R a: D ia be te s ( 18 ), st er oi ds ( 10 ), os te op oros is (3 2) , os te op en ia ( 18 ), a nd B P ( 55 ) o f a ll par tic ipan ts b: 5 0– 93 /N R c: 0 /1 00 d: 7 a: E st ro ge n b: O st eop or os is c: N R d: N R a: P rio r b: N R Imp lan t lo ss Ca se s: 4 i m pl an ts in 3 p at ie nt s Co ntr ol s: 0 Ca se # 1: 8 2 ye ar s ol d, n on sm ok er , B P i nt ak e s in ce 6 ye ar s Ca se # 2: 76 y ea rs o ld , non sm ok er C as e #3: 6 5 ye ar s o ld , sm oke r (Con tinues )
St ud y Stu dy d esig n Pa tie nt le ve l—n um be r of c as es / con tr ol s a: I m pl an ts b: G ra ft in g Si te l ev el — nu m be r o f im pla nt s/ gr af tin g pr oc edu res in ca se s/ co nt ro ls a: I m pl an ts b: G ra ft in g a: S ys te m ic dis ea se b: A ge r an ge /m ea n c: G en de r m /f ( % ) d: S m ok er s ( % ) a: H RT p ro du ct de ta ils (c on te nt , do sa ge) b: I nd ic at io n f or H RT i nt ak e c: A dmini st ra tio n ro ut e d: D ur at io n ran ge /m ean (ye ar s) a: H RT i nt ak e pr io r t o/ af te r im pla nt in st al la tion b: I m pl an t fol lo w ‐u p r an ge / m ean (y ear s) O ut co m e par am et er s O utc om e A dd iti ona l in for ma tion de S ou za e t a l. (2 013 ) Re tros pe ct iv e Co ho rt s tud y M edic al re co rds a: 1 3/ 18 0 b: 0 a: 61 /6 61 b: 0 a: O st eo po ro si s ( 6) , D ia be te s ( 5) o f a ll par tic ipan ts b: N R /5 0. 3 c: 3 5/ 65 d: 8 .3 a: N R b: N R c: N R d: N R a: P rio r b: 1– 8. 75 /N R M ar gi na l b one lo ss ( ≥2 m m ) Ca se s: 2 6 ( 42 .6 % ; IL ) Co ntr ol s: 18 9 (2 8. 6% ; I L) — Yi p e t a l. (2 012 ) Re tros pe ct iv e C ase –c on tr ol st ud y M edic al re co rds a: 3 6/ 30 1 b: N R a: i n t ot al 1 18 1 b: N R a: B P ( 20 ), d ia be te s ( 20 ), th yroi d d is ord er s, ca rdi ov as cula r di se ase s b: ≥ 40 /5 7 c: 0 /1 00 d: 1 5 a: N R b: N R c: N R d: N R a: N R b: 0 .3 –1 1. 9/ 6 Imp lan t lo ss N o s ig ni fic an t dif fe re nt di st rib ut io n be tw ee n c as es an d c on tr ol s — K os zu ta e t a l. (2 01 5) Pros pe ct iv e Co ho rt s tud y C lin ic al d at a a: 2 0/ 51 b: N R a: N R b: N R a: N R b: N R c: 0 /1 00 d: N R a: L ow d os es o f es trog en s b: N R c: N R d: N R /2 .6 a: P rio r b: N R /0 .5 Im pl an t s uc ce ss rate Ca se s: 7 5% ( PL ) Co ntr ol s: 9 2.9 % (P L) — M ar gi na l b one le ve l A ve ra ge : c as es 25 % , c on tr ol s 15 % R an ge : ca se s 17 .5 –1 00 % , co nt ro ls 10 –2 0% Si gn ific an t co rre la tio n be tw ee n bo ne lo ss a nd H RT N ote s. , r et ro sp ec tiv e c as e s er ie s; , c ro ss ‐s ec tio na l c as e s er ie s; , p ro sp ec tiv e c as e s er ie s; , r et ro sp ec tiv e c oh or t s tu dy ; , c ro ss ‐se ct io na l c oh or t s tu dy; , pr os pe ct iv e c oh or t s tu dy; , r et ro sp ec tiv e c as e–c on tr ol s tu dy ; , c ro ss ‐se ct io na l c ase –c on tr ol s tu dy; , p ro sp ec tiv e c as e–c on tr ol s tu dy . B P, b is pho sp ho na te ; f , f em al e; H RT , ho rm on e r ep lac emen t t her ap y; IL , i m pl an t l ev el ; m , m al e; N R , no t r ep or te d; P L, p at ien t l ev el. In co ns is te nc ie s i n t he n um be rs a m on g t he c ol um ns i n t hi s t ab le a re d ue t o i nc on si st en ci es i n t he o rig in al p ap er s. T A B LE 2 (Co nti nue d)
T A B LE 3 C ha r a ct er is tic s o f t he i nc lu de d s tu di es r ep or tin g o n f ea tu re s o f m ed ic at io n‐ re la te d o st eo ne cr os is o f t he j aw a ss oc ia te d w ith i m pl an t a nd /o r a ug m en ta tio n p ro ce du re s St udy N um be r o f pa tien ts (n umb er of im pla nt s) a: A ge r an ge / m ea n ( yea rs ) b: G en der m / f (n) c: S m ok er s (n) C om or bidi tie s an d/ or o th er re le va nt m ed ic at io n in ta ke re po rt ed (y es / no ) M RO N J loc al iz at ion a: I nd ic at io n, t yp e, d os ag e a nd ad minis tr at io n r ou te b: I nt ak e p rio r t o/ af te r s ur ge ry In ta ke t im e a nd t im ef ra m e b et w ee n va rio us ti me po in ts Tri gg eri ng fa ct or Laz ar ov ic i et a l. ( 20 10 ) 27 a: N R /7 0 b: 7 /2 0 c: 2 Ye s Po st er io r M N ( 15 ), an te rio r M N ( 5) , po st er io r M X ( 4) , an te rio r M X ( 3) a: O ra l f or o st eo po ro si s ( 11 )— A LN 70 m g/ w ee k o r 1 0 m g/ da y ( 11 ) i v f or mal igna nt d is ea se (1 6)— ZLN 4 m g ev er y 3 –4 w ee ks ( 7) , P M N 9 0 m g ev er y 3 –4 w ee ks ( 5) , P M N 9 0 m g ev er y 3 –4 w ee ks + Z LN 4 m g e ve ry 3– 4 w ee ks ( 4) b: p rio r a nd a ft er B P‐ M RO N J: A LN ( 68 m on th s) , Z LN (1 6. 4 m on th s) , P M N ( 50 .2 m on th s) , PM N + Z LN ( 53 m on th s) I ‐M RO N J: w ith in 6 m on th s ( 6) , m ea n 1 6. 2 m on th s ( B P p rio r t o I) Imp lan t su rg er y ( 6) , im pla nt pr es en ce/ sp on tane ou s (21 ) G ro up 1 — B P p rio r to I 2 3 a: A LN ( 10 ), Z LN ( 5) , P M N ( 5) , PM N + Z LN ( 3) b: p rio r B P‐ I: 0 –1 08 m on th s I ‐M RO N J: 0 –5 3 m on th s B P‐ M RO N J: 1 0– 11 5 m on th s G ro up 2 — B P a ft er I 4 a: A LN ( 1) , Z LN ( 2) , P M N + Z LN ( 1) b: a ft er I‐ B P: 2 2– 12 5 m on th s B P‐ M RO N J: 1–1 56 m on th s Ja co bse n et a l. ( 20 13 ) 12 + 2 w ith m et as ta si s o r in fil tr at io n o f mal igna nt un de rly ing di se as e ( 23 im pla nt s) a: N R b: 3 /1 1 c: N R No 4 M X , 8 M N s ite s [p os te rio r M N ( 5) , po st er io r M X ( 4) , an te rio r M N ( 3) ] 1 in c om bin at io n w ith a s in us l ift ( 2 pa tie nt s w ith m et as ta sis / in fil tr at io n N R) a: O st eo po ro si s ( 5) — A LN o ra l ( 2) , P M N (1 ), I B N i v ( 1) , A LN + P M N ( 1) i v f or mal igna nt d is ea se s ( 9)— ZLN (8 ), P M N + Z LN ( 1) b: N R B P‐ M RO N J: 3 8 m on th s f or 7 p at ie nt s w ith m al ig na nt d is ea se , 5 0 m on th s f or 5 p at ie nt s w ith o st eo po ro si s I ‐M RO N J: 2 0. 9 m on th s (1 7 m on th s f or 7 p at ie nt s w ith m al ig na nt di se as e, 2 5. 6 m on th s f or 5 p at ie nt s w ith os te op oros is ) ( 2 p at ie nt s w ith m et as ta si s/ in fil tr at io n: N R) N ot s pe cif ie d (C on tinues )