Participation of patients with
schizophrenia
Systematic overview on participation in
community and health care decisions of
people with schizophrenia
Examensarbete i psykiatri Malmö universitet 15 hp Hälsa och samhälle Socialpsykiatriprogrammet 205 06 Malmö
2
Participation of patients with
schizophrenia
Research on participation in community and
health care decisions of people with
schizophrenia
3
Abstract
Aim: This study is to examine the experience of participation in the community and health care decisions of people with schizophrenia.
Method: A systematic overview is conducted in this report with qualitative and quantitative approach to the empirical data. The main data searching is carried out in PsyInfo and Google Scholar. 6 articles are selected totally.
Results: Participation in society and health care agencies plays an important role for the recovery of the schizophrenia.
Conclusion: Participation can contribute to the recovery of schizophrenia. There are more and more studies and people discussing the importance of helping these people with schizophrenia back to the society. And the patients themselves also feel better and the symptoms are more manageable though participating in social activities. It puts demands on the health care agencies to design the implements. There is also a need for more effort to educate both the patients and the health care staffs.
4
Contents
Abstract………3 Contents………4 1.Introduction………...5 1.1 Community participation………51.2 Participation in the health care………7
1.3 Phenomenological approach………7
2.Theory………9
3. Aim and research questions………..9
4. Method………..10
4.1Design………..10
4.2 Criteria and search strategy………11
4.3 Ethic consideration……….11
4.4 Data analysis………...12
5. Result……….13
5.1 Summary……….……….15
6. Result discussion……….………...16
6.1Experience participation in community………16
6.2 Experience participation in the treatment process………...……17
6.3 The key to recovery progress………...………17
6.4 Transferability………..17
7. Method discussion………..18
7.1Qualitative and quantitative studies, integration verses separation…………..18
7.2 Limitation of the systematic overview……….18
8. Conclusion………..18
9. References………..19
Table 1. Search word in English and Swedish………...11
Table 2. Summary of data searching………..12
Table 3. GRADE evidence system……….13
Table 4. Summary for the selected articles………15
5 1.Introduction
Schizophrenia is widely considered to be the most severe and disabling mental illness and 20 million people suffer from it worldwide (WHO, 2019-10-4). There are 1,500 to 2,000 people have become schizophrenics every year and about 30,000 to 40,000 people have diagnoses schizophrenia in Sweden. And it was estimated until 2015 that only 5- to 7% av these people have worked in an open market (Socialstyrelsen, 2018-9-6). In general, people with schizophrenia have difficulties in participating in social life (e.g. work). This means that it is a great cost for the health care and social support, low income for the individuals, and this not yet accounts in the price of people and their close ones suffering from
schizophrenia. Besides of participating in social life, there is also a discussion about people with schizophrenia participating in policy decisions and
interventions they need. WHO (World Health Organisation) has pointed out (2019-10-4) that people with schizophrenia are prone to human rights violations inside the health institutions. Deinstitutionalizing is the new direction of the reform of psychiatry. The basic argument of this antipsychiatry movement was that psychiatric mental illness is not only medical in nature but social, political, and legal: Society defines what schizophrenia or depression is, and not nature (Shorter, 1997). The purpose of reformation of the psychiatry is to give the possibilities to people with psychiatric dysfunctions to participate in the social life as all others (Bogarve et. al, 2012). The point of participating in the social life, and even in decision-making in the service support, is that participation plays an important role in the recovery process. Patricia Deegan, a psychologist with own experiences of being schizophrenic, simply but strongly states that “community is not just a place”( Bogarve et. al, 2012). She means that participating in the social life is not only about physically going back to the society, but also being part of the society. Even though participation is a new direction of the recovery journey for schizophrenic people, yet still there are many difficulties on the way. WHO has also pointed out (2019-10-4) that people with schizophrenia are experiencing discriminations in the community. Stigma and discrimination can lead to limit access to health care, education and employment and so on. To increase the level of the patient’s participation in health care and in the society can be a great meaning for their recovery. In this report, the people with schizophrenia are named as “client” or “patient”. This is because of different studies or different health agents using different concept and working towards different directions. 1.1 Community participation
There may be different approaches to look at the psychiatric disorder, mental illness, whatever schizophrenia is called. Schizophrenia is considered to be the most serious and devastating mental disease. It is characterized both by the more classic, so called positive symptoms of auditory hallucinations(i.e., hearing voice) , delusions(i.e., false but stubbornly held beliefs), and formal disorder(i.e., not making sense when you talk) and by the so-called negative symptoms of withdrawal, isolation, apathy, and a lack of energy, pleasure, or
interest( Davidson, 2003) Emile Kraeplin(Davidson 2003) , who first identified ‘schizophrenia’, assumed schizophrenia was an organic disorder that attacked the person’s brain, leaving those afflicted with little hope for a life beyond
neurobiological degeneration and irreversible dementia. In this model, it means that schizophrenia is caused by neurobiological disorder and there is not much hope for recovery biologically. In the early twentieth century, schizophrenia was considered to be caused by interaction of biological factors, stressful life events
6
and also capability to cope with the stress. Despite of the considering of social environment in this model, it doesn’t allow the possibility for people with schizophrenia to recover. The illness and its underlying vulnerability will persist for the remainder of the person’s life, it is believed, requiring active treatment and rehabilitation for the person will preserve any remaining areas of independent functioning (Davidson 2003). This kind of understanding of schizophrenia as a neurobiological disorder has dominated for a century, even until now in some countries. Many researches focused on correlation between mental symptoms and brain structures according to the theories above. The underlying assumption was that a specific part of the brain or the connection between different brain regions was dysfunctional. This biological theory also formed the social policy,
community health care and public’s attitudes towards people with schizophrenia. Based on the perception that these people lose their mind to the illness and they can not recover, others need to decide for them and others have to make decisions for them. People assume that these people are not normal so that they establish a life in the society. Part of this, it is about if schizophrenic people can actually build a normal life; the other part is if the symptoms can be controlled. French philosopher and social theorist Michel Foucault’s Madness and
Civilization, published in 1961, argued that mental illness was a social and
cultural invention of the eighteenth century. Psychoanalyst Thomas Azasz, in his book The Myth of Mental Illness, he argued that the notion of psychiatric illness was “scientifically worthless and socially harmful” (Shorter, 1997). His book raised the question that why people were locked in the asylum if mental illness didn’t exist. Sociologist Erving Goffman’s work Asylum, published in 1961, he interpreted the asylum was a prison that wasted people’s life and “ it’s something that must be ‘done’ or ‘ mark’ or ‘put’ or ‘pulled’…” The underlying assumption was that the patients could not take control over their lives in the asylum.
Goffman described it as that the closed system in asylum had destroyed and taken the patient’s life. The works of Foucault, Szasz and Goffman inflamed the
deinstitutionalization at 1960s. Thousands of individuals with serious mental illness, such as schizophrenia, who in hospitals began to be discharged to
fledgling and underfunded community-based service. Anti-psychiatry movement had flourished in nineteenth century and late twentieth century it began an
argument that psychiatric disorder was not medical illness but related to social and political contexts. The society defines what schizophrenia or depression is, not nature. If the psychiatric illness is socially constructed, it must be deconstructed in the interest of freeing deviants, free spirits and exceptional creative people from the stigma of being “pathological” (Shorter 1997). It implied that mental illness, such as schizophrenia, was caused by social factors and such brain disease was not real. People with serious mental illness have experienced significant diversity in the courses and outcomes of these mental illness (Larry, et.al.2009) It implied that mental illness, such as schizophrenia, was caused by social factors. And then returning to the community became the new direction of recovery of mental illness, such as schizophrenia.
1.2Participation in the health care decisions
Sherry Arnstein, was working as a special assistant to the assistant secretary at the U.S. Department of Housing, Education, and Welfare (HUD), she brought forth the influential “ladder of citizen participation” model (see figure 1). The purpose of this model is to describe participation of the citizen in different levels. The first two steps manipulation and therapy are considered to be nonparticipation. In this
7
level, the clients are involved in the activities that are diverted their attention from their own problem. The clients have no influence on this level. For example, the clients need to accept what the clinic decides what it is good for them. Step three, four and five are considered to be symbolic participation. These three steps include information, consultation and placation (Englander & Invarsdotter, 2017). Three steps can provide limited influence for the clients. When the clients
participate to develop their individual plans, they are informed and given advice. The staff doesn’t care about the clients’ opinions and individual needs. It means that the clients can not really participate in the decision-making. The last three steps, Arnstein means that the citizens have real influence on the last three steps. The clients can participate in the process of decision-making formally and their opinions are taken seriously.
Figure 1
Shared decision-making is a method that can potentially contribute to the participation and recovery in the psychiatric care and support (Englander & Ingvarsdotter, 2017) It is a general method that develops participation in all decisions that relate to the clients. Placing the clients as the center of all decision-makings is the key to the door of recovery. Shared decision-making is the process of cooperation between the clients and the service agencies.
1.3 Phenomenological approach
Biological research has brought forth a growing sense of mental disorder is no longer a fault, no longer at fault to have a brain disease. And it is a third-person perspective of understanding mental disorder. Seeing schizophrenia is a brain disease is just the beginning of desintitulization. Most of psychiatric research begins with the premise that people with schizophrenia are different from the rest of us (Davidson 2003). That will say the research give out the message to the public that schizophrenia is different, at least it is a different disease. That may, however, lead the research or our knowledge of schizophrenia in a confusion. If
8
we think these people are no longer people like the rest of us, it is less possible to get approach to true experience of schizophrenia. What can we learn more from the patient’s perspective of schizophrenia? Parnas and Gallagher consider that the nature of mental disorder is to be primarily constituted by the patient’s anomalies of experience, expression, and existence that typically involve suffering and dysfunction. It means that mental disorder is consisted of a series of phenomena. Kirmayer (2017) suggests that mental symptom is hybrid object, which consists of subjective mental symptoms and objective mental symptoms. Mental symptom is considered as a hybrid object, which consists of different materials, or elements from divers types of backgrounds, or from admixtures of organic/biological and sociocultural components (Berrios & Markova,2017).Based on this perception, Kirmayer (2017) points out that mental symptoms present as subjective
complaints, whether volunteered or elicited(e.g., depressed mood, anxiety, hearing voices and so on) and symptoms that are determined by the clinician as objective signs/behaviors(e.g., flight of ideas, psychomotor retardation and so on).
Subjective mental symptoms consist of phenomena such as complaints of anxiety, fatigue, hearing voices, compulsory to do something and so on. Phenomena are heterogeneous and even normal people can relate themselves to some of the symptoms, such as worries, tiredness e.t.c.. Subjective mental states must refer to people are aware of (Kirmayer, 2017). That will say that mental symptoms are presenting of the internal states. If a person tells that he/she hears voices, this person is interpreting an internal state. Kirmayer means that all the subjective phenomena are based on an awareness of something. And schizophrenia has the similar mental states, but they hear things that other people don’t, they see things that other people don’t. From awareness to mental symptoms, a lot of internal and external factors can contribute to form the interpretation of the mental states. The internal factors relate to individual personality, educational, and life experiences and so on. External factors, such as upbringing, society and culture will interact with internal ones to influence the interpretation of mental states. There is a third factor. It is that how the individuals interact with other people, especially with a clinician. The neurobiological signaling will thus correspond to particular state of awareness. To give it meaning, this state of awareness must first be subject to the layers of interpretative processes. Such processes will in turn depend on and reach out to discussed diverse aspects of each individual and their sociocultural
background (Kirmayer,2017). It means that the mental state needs to be interpreted in a sociocultural background. Like subjective mental symptoms, objective mental symptoms also have a hybrid structure. It includes a series of clinical phenomena that are named/constructed/shaped by factors operating via the clinician’s interpretation (Kirmayer,2017) Objective mental systems indicate that neurobiological state configurated by cultural proceed of the individual and clinician. In this case, it means ‘diagnosis’. It is how the individual and clinician identify the mental symptoms as diagnosis. Apart from the clinician’s
sociocultural background, their clinician experience, the context in which the interview takes place, and so forth, there will be personal experiences and biases(e.g., past traumas or emotional connections), all of which will be
contributing to the way in which a clinician will identify, interpret, and name a particular “behavior” or “sign” (Kirmayer,2017). It means that definition of a particular symptom which can be affected by the experiences and sociocultural background of the clinician. In order to understand the symptoms, it is important to have knowledge of the individual sociocultural background, clinician’s expertise, experience and how these factors interact with each other. Subjective experience can not be faithfully assessed by structured interrogation that allows
9
only affirmative or negative responses, that is, in the manner of a performed structured interview (Kirmayer, 2017) It means that schizophrenia can be
understood better in a certain background combining with the person’s individual experience, instead of through a structured interview designed for all.
2.Theory: phenomenological approach schizophrenia and experience of participation
With the help of transcendental reduction, we can have a closer view of
intersubjectivity. We usually assume things according to our own experience and from our own point of view. In this case we can not understand the others in the their reality. Phenomenological approach gives a closer look to the world of schizophrenic people. We place ourselves in their world and have a picture of the illness from their perspective. Intersubjectivity is to experience another person based on apperceiving another person’s experience. Intersubjectivity is critical to construct and reconstruct the interpersonal interaction when we meet a patient and try to understand him/her from his/her perspective. To understand another person is an inferential process to answer the question of how the other feels and what the other experiences. Mealou-Ponty points out that to observe another person is not to recognize ‘another myself’. ‘Another myself’ would imply that our own reflections have been registered in our understanding onto the other. With considering of the phenomenological approach, Thomas J. Csordas suggest four elementary methodological rules that are intersubjective inference of experiential immediacy-observe voice, anticipate surprises, and respect reflexivity, to
understand the others. These four rules imply an empathic way to observe and interact with the patient. Temporality is relevant to time dimension which subjects to alternation of psychiatric disorder. The experience of time is to catch a sense of the temporal period of the psychiatric disorder. Intentionality is to the extent that we understand if the conditions of psychiatric illness is permanent or episodic, and whether the life trajectory should be interrupted by the life events and plans. No matter which dimension or which life trajectory, it is about the how patient understand their psychiatric disorders and what realistic or unrealistic possibilities and goals towards the future. But Csordas has not explained clearly how
intentionality related to or affect the development life trajectory. Larry Davidson (2012) performed a phenomenological approach to schizophrenia by analyzing the patients’ narrative. This study provides a particular good illustration of the unique contributions of a phenomenological approach of qualitative research on the experience of schizophrenia. The research analyze the experience of people with schizophrenia involving themselves in the social activities. Davidson(2012) suggests the focus of recovery interventions should return to the person himself or herself as the crucial role in the recovery process. Understanding the role of the person as a subject of experience in a certain context is a key to understand how schizophrenia affect the person.
3. Aim and Research Questions
The aim of this report is to examinate the experience of participation in the community and health care decisions of people with schizophrenia.
To describe the correlation between schizophrenia and participation, it is about how these two variables interact with each other and how much they relate to each other. Participation is to participate in social life and clinical decisions. Social life is about daily life, social relationship, work, such social activities. Clinical
10
implements within health care. The questions may also bring forth the factors that can affect the participation. The questions are going to be presented with
qualitative studies(narratives) and quantitative studies (numbers and statistic). The following questions are going to conduct the purpose of this research:
How do the people with schizophrenia experience participation? What do the people with schizophrenia think about participation? How does participation facilitate recovery of schizophrenia? 4.Method
In this report, systematic overview is used as research method. Science research is based on the current science studies as well as the empirical studies. Systematic overview is a way to summarize the empirical data systematically. Systematic overview can summarize what has been done and what has been proved and what need to be done more in the future. In this report, systematic overview can have a big picture of researches that have been done about participation and recovery, and what kind of experiences that the patients have. In the reviewed articles, it may contain quantitative studies can study the causality. How participation
facilitate recovery process. It may also contain qualitative studies which can study how patients experience the participation and increase the understanding of the concept of schizophrenia and participation. Some reviewed articles may have semi-structured interview study design.
4.1 Design
The systematic overview is including the following steps which are recommended by The Guidance of Systematic Overview (The Public Health Agency of Sweden, 2017):
1. Preparation – performing a preparatory mapping and identifying research questions, literature search terms, and selection criteria
2. Searching – developing a search strategy and performing the literature search according to the preparation
3. Judging relevance – excluding irrelevant studies based on the article’s title, abstract, and, potentially, full text
4. Assessing quality – evaluating the trustworthiness of relevant studies based on generally accepted standards for quantitative and qualitative research
5. Presenting the studies – visualizing and documenting the literature search, the judgment of relevance, and the assessment of quality
6. Synthesis – drawing conclusions from the results of the various studies through meta-analysis or meta-synthesis or through narrative analysis
7. Valuing the scientific foundation – evaluating the evidence and formulating an opinion based on the previous methodological steps
11
Table 1 Search word in English and Swedish (translated from the English)
English Participation recovery Schizophrenia
Swedish Deltagande återhämtning Schizofreni
4.2 Criteria and search strategy
Participating in the social life and clinical decisions under treatment process has been important in the last 20 years. Thus the research is going to search the studies since 2000. The most studies happened in western world therefore studies that was written in English is considered. This report is also hopefully used in Sweden and therefore studies in Swedish will also be reviewed. Comparing the Swedish model and the other western world. Participants in the studies focus on people over 18 years old no matter how long time they have been diagnosed. Searching process is divided into four steps, which in every step criteria, validity and quality will be discussed. The qualitative studies should describe the
experience of participation of people with schizophrenia. The quantitative studies identify the correlation between participation and recovery from schizophrenia. And searching will be processed in the database of Malmö University’s
recommendation, which connects to different platform of studies. There are seven platforms under the title “socialpsykiatri-artiklar och databaser (social psychiatry-articles and data base)”. They are Psycinfo, Cinahl, PubMed, Google scholar, Sociological Abstracts, SwePub, Svemed+. Psycinfo, Google scholar, SwePub and SveMed+ are selected databases. Psyinfo includes articles in psychiatry, psychology and adjacent subjects. Its articles are more specific about psychiatry and psychology. Google Scholar is widely connected to different scientific
research platforms, as it describes itself, all the articles are already overviewed by the website. Swepub and SveMed+ are the Scandinavian data base within
medicine and health care with references to Scandinavian journals. Included qualitative studies will focus on experience of schizophrenia and participation meanwhile the quantitative studies will research on correlation.
Search word “schizophrenia participation” gave 2587 result in PsycInfo. First selection of peer view is based on the titles. In PsycInfo, a lot of the articles were filtered with the reason of not relating to participation or schizophrenia. And then some articles were filtered further on because of the writing language is German, Russian and Danish. And then overview of the abstract filtered the articles that were only about biological research on schizophrenia and no mention on participation (See table 2).
The criteria of inclusion of both qualitative and quantitative studies, it is written either in Swedish or English.
4.3 Ethic consideration
All the selected articles should be overviewed ethically. All the materials are fetched on line, it is difficult to do a judgement how the researches are done at the time.
12 Table 2 Summary of data searching
PsyInfo Date Search word Peer
reviewed Read abstracts Read articles Selected articles 1. 2020-8-27 Participation recovery 2587 2. 2020-8-27 Schizophrenia recovery 3935 3. 2020-8-27 Schizophrenia participation 1587 310 37 4 4. 2020-8-27 Deltagande återhämtning 0 5. 2020-8-27 Schizofreni återhämtning 0 6. 2020-8-27 Schizofreni deltagande 0 Google Scholar 2020-8-27 Participation recovery 3070 2020-8-27 Participation recovery schizophrenia 864 2020-8-27 Social Participation recovery schizophrenia 1180 2020-8-27 Schizophrenia participation 1320 126 18 2 4.4 Data Analysis
In this report, GRADE (Grading of Recommendations, Assessment, Development and Evaluations) system is selected to analyse the quality of the selected articles, which is recommended by SBU (Swedish Agency for Health Technology
Assessment and Assessment of Social Service) GRADE is an evidence evaluating system, which is developed by the GRADE working group that SBU participates. GRADE is an evidence grading system that includes four levels ‘high’,
‘moderate’, ‘low’ and ‘very low’ (SBU, 2016). ‘High’ means that the result is stable. There is low risk that a similar new study will have a different result. ‘Moderate’ means that the risk is at a medium level. ‘Low’ indicates that the result repeats if all the criteria in the studies can strictly fulfilled. ‘Very low’ indicates that more researches need to be done to prove the result.
13 Table 3. GRADE evidence rating system
Rating Rating in Swedish Study design
High Starkt Randomized Clinical Trial (RCT)
Moderate Måttlig starkt
Low Begränsat Observation studies; Cohort- and
case management studies
Very low Otillräckligt Case studies
5. Result
Search word is “schizophrenia participation” ‘schizofreni
deltagande(schizophrenia participation)’ SveMed+gave 6 results(2020-8-27). But none of the articles fit into the criteria. SwePud is also a Scandinavian data base for health care. SwePub gave 2 result. None of the articles were selected. Psycinfo gives 1586 results (2020-8-27) 4 articles were selected. There is no found in the Scandinavian researches that relates to this report. Participants are mainly people with schizophrenia in the selected articles. And there are only adults included in these articles. Google Scholar includes literatures that are claimed that are reviewed by google. It links to many scientific literature platforms. The same search work ‘schozphrenia participation’ gave 645,000 results (2020-8-19). Some results are overlapped with PsycInfo. The search word ‘schizophrenia
participation recovery’ narrowed down the result to 98,200. Some articles are accessed with payments. 2 articles are selected eventually. In total 6 articles are selected. These 6 articles match the criteria and aim for this report. Considering the grade of evidence rating system, these 6 articles use RCT as study design. According to the rating system recommended by SBU, studies with RCT design, the evidence level is high. It means that the result is more stable and reliable. The selected articles take place in US and Canada among Western and Asian. Participants are with domestic and foreign backgrounds. Quantitative and
qualitative studies have been used in the selected articles. Qualitative study uses method such interview, observation and so on, which can get closer to the participants’ world and understand schizophrenia and participation as a
phenomenon. Quantitative study can identify the correlation between participation and recovery (see Table 4).
Malgorzata &Katarzyna (2011) study to find out the patient’s opinions about psychoeducation in schizophrenia. The study was done in Poland and there are 169 patients participated. The result shows that 84% of the patient think more information about their illness can help them cope with the symptoms so that they can improve their daily life. And the result also shows that emotional atmosphere is important under the therapeutic sessions and more means can the patient involved in participation during the treatment.
Thomas et al. (2019) perform a qualitative study to examine the correlation between participation in the community and neurocognition among people with serious mental illness in US. The researcher has selected 168 adults with
14
amount community participation and improving verbal memory. Finding suggests that participation in the community improves neurocognitive functions.
A semi-structured qualitative and quantitative study conducted by Roberts et al. (2000) is to examine how patients and psychiatrists view ethically of importance of biomedical research participation in US. 136 people participate and 63 av them are with schizophrenia and 73 are others with serious mental illness and
psychiatrists. The result indicates that patients have a feeling of hope when they involve in psychoeducation as part of the treatment. Meanwhile the psychiatrists underestimate the willingness of the patients to participate the autonomous decision making.
Virdee et al.(2017) conducts a longitudinal study to explore the community participation and recovery amongst South Asian origin in Canada. 10 people with schizophrenia participate the research. Three interviews take place within 3 months. 19 service providers and community members are also interviewed. The result indicates that community participation is a key component of recovery for people with schizophrenia.
Burn-Lynch et al. (2016) perform a quantitative study to explore correlation between community participation and quality life of people with serious mental illness in US. There are 606 participants. The result suggests positive correlation between community participation and quality of life. The participation facilitates the recovery process and vice versa.
A semi-structured study by Patterson et al. (2011) examines the patients’ perception of recovery by placing them in the community. There are 86 participants with schizophrenia or schizophrenia-effective disorder. The result suggests that 82% participants believe recovery being possible and 52% think that they are in recovery, no matter they are willing or compulsory placing in the community.
15
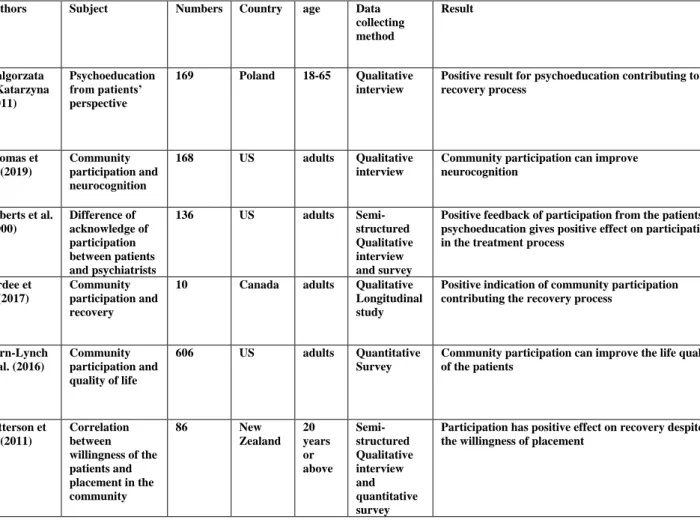
Table 4 Summary for the studies on correlation between participation and recovery of schizophrenia
Authors Subject Numbers Country age Data
collecting method Result Malgorzata &Katarzyna (2011) Psychoeducation from patients’ perspective 169 Poland 18-65 Qualitative interview
Positive result for psychoeducation contributing to recovery process Thomas et al. (2019) Community participation and neurocognition 168 US adults Qualitative interview
Community participation can improve neurocognition Roberts et al. (2000) Difference of acknowledge of participation between patients and psychiatrists 136 US adults Semi-structured Qualitative interview and survey
Positive feedback of participation from the patients, psychoeducation gives positive effect on participation in the treatment process
Virdee et al.(2017)
Community participation and recovery
10 Canada adults Qualitative
Longitudinal study
Positive indication of community participation contributing the recovery process
Burn-Lynch et al. (2016) Community participation and quality of life 606 US adults Quantitative Survey
Community participation can improve the life quality of the patients Patterson et al. (2011) Correlation between willingness of the patients and placement in the community 86 New Zealand 20 years or above Semi-structured Qualitative interview and quantitative survey
Participation has positive effect on recovery despite of the willingness of placement
5.1 Summary
The results highlight in particular in how participation affects recovery for schizophrenia and what kind of participation can contribute to a successful rehabilitation. The patients have positive experience of recovery through participation in the community and health agencies. Participation gives positive result in the way that the social relationships make the patients happy.
Psychoeducation is considered to be one of the interventions that patients actively participate in the treatment process. Psychoeducation may increase the level of decision making of the patients. Four of the studies indicate strong evidence that participation in the community has positive effect on recovery. Two of studies even identify participation in the community improving of the biological functions. One study has identified that good relationship between patients and therapists improves the effect of treatments. Two studies identify psychoeducation can help the patient increase the knowledge of mental diseases, which
contributing for them to handle their symptoms. One of the studies shows that 85% of the patients thinking positive about psychoeducation. Two studies identify share decision making having positive effect on motivating the patients take part in the treatments.
16 6.Result Discussion
6.1Experience participation in community
Thomas et al. (2019) performed the study to show significant effect of community participation, which improve their verbal and cognitive functions. Patients has experienced positive change during the recovery process. In the studies of Virdee et al. (2012) and Patterson et al.(2011), patients thinks that life quality is improved and the results in the study of Burn-Lynch et al.(2016) In all these studies,
patients live in among other people which can expand their social lives. Most of them have felt improvement and are positive about the community life. Davidson suggests that the only way for people with schizophrenia feel less isolated and alone is to be with people, real or imagined, who care or accept the people despite of his or her illness(Davidson, 2003, s.164) All people need to feel they belong to someone, somewhere or something, so do the people with schizophrenia. The mental illness has taken away the people’s identity as a person. They have lost many other dimensions of their lives as an extend of living schizophrenia. People have experienced some degree of improvement in their condition almost
invariably identify another person as having been of crucial important process of recovery (Davidson, 2003, s. 161)
6.2 Experience participation in the health care decisions
Study of Malgorzata& Katarzyna(2011) shows that psychoeducation can give patients more information about their illness and have a better involvement in the treatments. And study of Roberts et al. (2000) shows that share decision making is important for the patients take part in the treatments. The people with
schizophrenia participate in the decision-making under the recovery process is much about power sharing with the service agent. Although the patients and the psychiatrists have different perception of sharing power of making decisions, but both psychiatrists and patients agree that share decision making is important (Roberts et al. 2000). At the center of psychiatry as a clinical discipline is the human encounter between patient and clinician. This relationship includes the process of empathy, identification and emotional connection based similarity, but also the recognition of difference, otherness, or alterity (Kirmayer 2017). From 1950s onward, empathy became a keyword in the professional worlds of
psychiatry and clinical psychology, spurred on by the recognition that the effort to listen to closely and track another’s experience was a key element in successful psychotherapy(Kirmayer 2017) In order to understand the subjective world of the schizophrenic people, empathy help build the bridge between two different worlds. Of course, understanding the others is more than just empathy, but empathy provides a way to explore the phenomenological encounter. Clinical understanding demands attention to multiple sources of knowledge, each with its own epistemology and methods of inquiry (Kirmayer, 2017). Empathy is usually fertilized by the interest and willing to engage in the other. ‘Seeing from the other’s view’ and it is an art of understanding the other by putting away one’s own experience. How much the health care takers understand the patient can affect the decision of in which level things the patients can decide for themselves. Although it is important to understand the patient, not all the factors of causes of the patient’s behavior and experience are included in their narratives. Some factors are outside the patient’s awareness. For example, the patients do not have enough knowledge to decide, or the patients are unable to decide because of their psychological impair.
17 6.3 The key to recovery progress
Going back to the society, being with friends, families and colleagues,
participating the social relationships help them to find back the lost part of life. Davidson (2003) pints out that social relationships that can contribute to recovery should be equal and mutual. People with schizophrenia should be able to
recognize themselves and find their identity in a such relationship. Community participation expands the patients’ social network and enhance their social
activities. On the other hand, understanding schizophrenia symptoms in different context is important for the patient participate in the share decision making in the service agents. So that the service provider can understand the narratives and description of people’s symptoms. How people understand schizophrenia is how people define schizophrenia and how to get along with the schizophrenic people. People in different context express themselves differently. This may be helpful when we try to tolerate the people with schizophrenia. It simply is a matter of uncovering the motivational relationships at play in shaping the experiences in question or rending explicit the motivational horizon, that is the implicit context in which these experiences take place (Davidson, 2003) Davidson means that it is especially important to understand schizophrenia in the context. Seeing the patients as ‘other’ than an “object” is the practice of phenomenological approach. The results should also be considered to be the body of knowledge that underpins the strategies to implement the participation, such as how the health care staffs build a happy and contributing relationship with the patients.
6.4 Transferablity
The studies on participation included in the results were carried out in USA, Canada, Australia and Sweden, mainly in USA. At the date that this overview was carried out, there were not so many studies was done in Sweden, even
Scandinavian countries. This factor diminishes the possibility of transferability of the result in the Swedish circumstances. Mainly the cultural context is shifted that can affect the way of implements and even the health care and political system are different. The results from Sweden can be transferable. However, transferring the results to general population is less possible because this study is focusing on people over 18 years old and no more than 60 years old. This study is to introduce the importance of participation to the recovery of people with schizophrenia. Although most of the studies are not done in Sweden but still there are similar factors to the target groups. For example, schizophrenia itself as a mental disease and participation itself as an implement, in general, are universal.
7. Method Discussion
Systematic overview is to overview and critique the previous studies, extract and analyse the data that is included in the review. It is a secondary data analysis to ask and answer some important questions within social science. Secondary
analysis can provide a view of trending and new emerging research of the subject. The data bases that are used this report are platforms for scientific reports and recommended by Malmö University. Systematic overview is often significantly cheap and quick to complete since the first-hand date is collected by others. The data is usually already prepared and reviewed by the writers. But if the data is not collected by one’s own, it is difficult to control the validity and quality of the data. It might happens that problems occur during the data collection will not be
known. There is also risk that the data is not reliable or not constructed as needed. In some cases, extra variables may need to be brought up to complete with the
18
current ones in the available data. There are many platforms can be searched around. Wide range of data resources is available.
7.1 Qualitative and quantitative studies, integration verses separation Qualitative study is to explain the social phenomenon as an experience.
Quantitative study is to measure and calculate effect and outcome. Mixed methods research offers powerful tools for investigating complex processes and systems in health and health care. (Fetters MD et al., 2013) Several advantages can accrue from integrating the two forms of data. The qualitative data can be used to assess the validity of quantitative findings. Quantitative data can also be used to help generate the qualitative sample or explain findings from the qualitative data (Fetters MD et al., 2013). Qualitative inquiry can inform development or
refinement of quantitative instruments or interventions or generate hypotheses in the qualitative component for testing in the quantitative component (Fetters MD et al., 2013). For example, if a quantitative study indicates a positive effect of
participation, then a qualitative study can research in what way and how the patients experience the participation contributing the recovery process. Integration of two methods can enhance the quality of the result and provide a
multi-perspective view of a phenomenon in the health care.
Although there are many potential benefits of integration of two methods, Bryman (2007) brings up the question that how much the components of qualitative and quantitative studies can illuminate each other? In another word, the components of qualitative and quantitative researches may not be designed to integrate each other. And the findings may not be integrated. Bryman (2007) also points out that it is not so sure of how much the two methods “genuinely integrate”. For example, if the qualitative components follow the hypotheses based on the quantitative components, there is an intent to build qualitative studies on the quantitative studies. Then the findings of a mixed method might not be extended. 7.2 Limitation of the systematic review
This systematic overview doesn’t not suggest the participation are affected by the recovery process and in which level the patients can recover. The results don’t point out the efficiency of participation to recovery.
8. Conclusion
Recovery is partly about getting the power back and control one’s own life. People with schizophrenia need to participate in decision of their treatments and social life, which is a way to gain control over their lives. Participation in the social and political life help the patient to recovery in their own definition. Understanding the world of the schizophrenia, taking the cultural background in considering. There are a lot of studies of schizophrenia. Most of them are about how to understand the symptoms and point out the importance of participation for people with schizophrenia. Practical interventions of participation are not often researched. There should be more means and interventions to be researched.
References
Bill Burns-Lynch, MA, LPC, CPRP, Eugene Brusiloviskiy, MUSA, and Mark S. Salzer, PHD, (2016) An empirical study of the relationship between community
19
participation, recovery, and quality of life of individuals with serious mental illness, Isr J Psychiatry Relat Sci, Vol 53
Bogarve C, Ershammar D, Rosenberg D, (red.) Rehabilitering och stöd till
återhämtning vid psykiska funktionshinder: Mölighetens metoder för en ny praktik, Stockholm, Gothia Fortbildning
Bryman, A. (2007). Barriers to integrating quantitative and qualitative research. Journal of mixed methods research, 1(1), 8-22.
Englander M.& Invarsdotter K., Socialpsykiatrins grunder: människors villkor, Falkenberg, Press Team Sweden AB
Fetters, M. D., Curry, L. A., & Creswell, J. W. (2013), Achieving integration in mixed methods designs—principles and practices. Health services
research, 48(6pt2), 2134-2156.
Gallagher S(2012) Phenomenology, UK, Palgrave Macmillan
Kirmayer.L., Lemelson R. & Cummings C. (2017), Re-Visioning
Psychiatry-Cultural phenomenology, critical neuroscience, and global mental health, UK,
Cambridge University Press
Malgorzata & Katarzyna, (2011), The participation of patients with schizophrenia
in psychoeducation-The analyses from the patient’s perspective, Archives of Psychiatry and Psychotherapy, Vol 12, Iss2, 67-72
Polit, F.D. & Beck, C. (2018). Essentials of Nursing Research – appraising
evidence for nursing practice. Philadelphia: Wolters Kluwer Health.
SBU, (2016), Evidensgradering, >https://www.sbu.se/globalassets/ebm/metodbok/sbushandbok_kapitel10.pdf#:~:t ext=SBU%20anv%C3%A4nder%20det%20internationellt%20utarbetade%20GR ADE%C2%AD%20systemet%20%5B1%2C2%5D,via%20GRADE%20Working %20Group%20d%C3%A4r%20%C3%A4ven%20SBU%20ing%C3%A5r.<HTM L(2020-10-07)
Shorter E.,(1997) A history of psychiatry-from the era of the asylum to the age of
Prozac, Canada, Wiley & Sons, Inc
Tess Patterson, Richard Mullen, Christopher Gale, Andrew Gray,(2011)
Compulsory community treatment and patients’ perception of recovery in schizophrenia, Sage Journal, Vol 19, Iss5, s.431-433
The Public Health Agency of Sweden, Guidance of systematic litterature
overview, Article number: 01841-2016-3.3-1, s.14
Thomas, Elizabeth C, Gretch, McCormick, Bryan, Salzer, Mark C(2019), An
exploration of linear and curvilinear relationships between community participation and neurocognition among those with serious mental illness,
Psychiatric Rehabilitation Journal, Vol 42, Iss.4 , s.358-365 Topor A, (2009) Socialpsykiatri, Malmö, Bonniers
Virdee, Gursharan, , Frederick, Tyler, Tarasoff, Lesley A, McKenzie, Kwame, Davidson, Larry, et al.(2017), Community participation within the context of
recovery: Multiple perspectives on South Asians with Schizophrenia, International
20
Weiss Roberts, Laura, Warner, Teddy D, Brody, Janet L,(2000), Perspectives of
patients with schizophrenia and psychiatrists regarding ethically important aspects of research participation, The American Journal of Psychiatry, Vol 157,
Iss1, s.67-74
WHO,(2016), Schizophrenia,