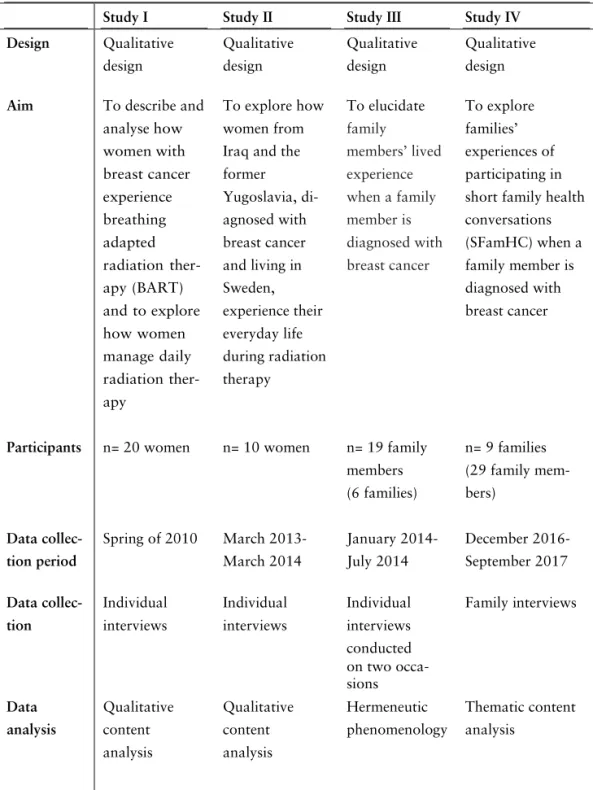
On a journey for survival : everyday life during radiation therapy from the perspectives of women with breast cancer and their families
160
0
0
Full text
(2)(3)
(4)
(5)
(6)
(7)
(10)
(11)
(12)
(13)
(16)
(17)
(18)
(19)
(20)
(21)
(22)
(23)
(24)
(25)
(26)
(27)
(28)
(29)
(30)
(31)
(32)
(33)
(34)
(36)
(37)
Figure

Related documents
There were basically used: The European Organisation for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLQ-C30) , the Cervix Cancer Module (QLQ-CX24),
De kvinnor som genomgått en total mastektomi uttryckte en känsla av att inte ha varit lika delaktiga i beslutet kring sin behandling, samt hade i större utsträckning en
The present thesis explored the effect of light pressure effleurage massage in women with breast cancer in six main domains; nausea, anxiety, depression, quality of life, stress
However, regarding no family history of cancer and family history of ovarian cancer, lesser agreement was observed in the reports from relatives (κ=0.54 and κ=0.78,
The results of this comparison showed that proton treatments could improve target coverage and reduce normal tissue burden and the integral dose in both gated and
The legend of Table I should read ”[…] study, presented as percentage of the prescribed dose or the total volume of the specified structures.”.
techniques including proton therapy for breast
To evaluate the effect in women with BCa and hot flushes of 12 weeks of acu- puncture or two years of hormone therapy on both the number of hot flushes per unit time and the level
