How might we decrease the amount of information
lost between and during night shifts through
implementing a digital alarm register?
Julia Brandt
Interaktionsdesign Bachelor
22.5HP VT/2020
Abstract
This thesis explores the digital opportunities at a mobile workplace in elderly home care by analyzing the existing information and communication flow that happens between and during shifts in everyday practice using a user-centric approach. The fieldwork analysis reveals that a combination of media, both verbal, digital and paper-based is used throughout the shift to pick up and pass on information. With an ageing population that requires care from home, to sustain and improve the quality of care, my research indicates an evident need of supporting home care workers whilst being out of office.
The research question is: “How might we decrease the amount of information lost between and during night shifts through implementing a digital alarm register?” which evolved from one out of four design opportunities.
The main participants and focus throughout this study are the end-users, night shift home care workers at two different locations in the Malmö municipality. By involving the users early in the process, having a rich fieldwork process and putting emphasis on “support” rather than “replacement” resulted in a mobile application tool presenting relevant patient information, current alarms and alarm history.
Acknowledgements
I would like to show my greatest gratitude towards my supervisor Elisabet M. Nilsson for her valuable guidance and support throughout this thesis. Thank you for always being available and taking your time!
I would also like to thank the home care workers that participated in both interviews, discussions and usability test.
Table of Contents
Abstract ... 2 Acknowledgements ... 3 1 Introduction ... 5 1.1 Problem/topic ... 5 1.2 Research question ... 61.3 Aim and purpose ... 6
1.4 Motivation ... 6
1.5 Scope and delimitations ... 7
2 Background ... 7
2.1 Ageing in Sweden ... 7
2.2 Home care ... 8
2.3 Existing technology ... 8
2.4 For the home care workers ... 9
3 Previous research ... 10
3.1 eHealth ... 10
3.2 CSCW ... 11
4 Methods ... 13
4.1 User-centric design (UCD) ... 13
4.2 The Double Diamond ... 13
4.3 Literature review ... 14 4.4 Field studies ... 14 4.5 Data analysis ... 15 4.6 Ideation methods ... 17 4.7 Ethical consideration ... 19 5 Design process ... 19 5.1 Field studies ... 20
5.2 The essentials of a night shift worker ... 20
5.3 Five thematics ... 24
5.4 Identifying design opportunities ... 26
5.5 Early concept sketches ... 28
5.6 Prototyping #1 ... 31
5.7 Prototyping #2 ... 33
6 Result ... 35
7 Discussion and Conclusion ... 38
7.1 Using a user-centric approach ... 38
7.2 CSCW and eHealth ... 38
7.3 The significance of prototyping ... 39
7.4 Critical reflection ... 40
7.5 Implication for future research ... 40
7.6 Conclusion ... 41
1 Introduction
1.1 Problem/topic
Recent demographics show that the population is getting older. Nonetheless, in Sweden, where the median life expectancy today is 83 years, one of the highest numbers in the world, along with a striking decline in child births, there is a call for societal changes. Numbers suggest that an estimated 30% of our population will be 65 years of age or older in 2028. Not only are we getting older, we are staying healthier for longer with the support of an advancing health care. However, despite staying healthy we cannot avoid the health-related diseases that comes with ageing, and elderly health care expenses are estimated to rise with 240% up until 2040. To tackle the demographic changes whilst providing good service and care for the elderly, the government of Sweden have invested 200 million SEK to support digitization of health care, which is the greatest investment in eHealth to date. Sweden is aiming to become the world’s leading country of digitization in health and social care by 2025, but there is a long way to go.
When it concerns Swedish home care, many municipalities already have digital tools up and running to support health care professionals in their daily activities. There have been discussions however, concerning for whom the tools are actually beneficial. In October 2019, the home care application, PluGo, run in Gothenburg was criticized by Arbetsmiljöverket (Sverige Radio, 2019) for having an opposite effect on the work environment, leading to an untenable, stressful workplace with personnel risking their health to accommodate new procedures. The application did not consider the distances between patients nor bathroom breaks, creating tension amongst home care staff that refuse to work under such circumstances. Working in home care today, has somewhat of a bad reputation and therefore not enough people, not to mention qualified sub-nurses, are applying for jobs in home care. Numerous municipalities are experiencing high turnover in staff and many employees on
Figure 1. Estimated population demographics in 2060. Figure 2. Population demographics in
sick leave due to stress related injuries which increases recruitment costs and decreases quality of care (Målqvist & Lundin, 2015).
Introducing technology in the workplace requires thorough field research studies to become a long-term success (Erlingsdottir & Sandberg, 2016). This thesis project therefore examines the home care situation in Malmö, focusing on night shift workers, with the aim of finding a design solution that may support and improve day-to-day work life.
1.2 Research question
“How might we decrease the amount of information lost between and during night shifts through implementing a digital alarm register?”
1.3 Aim and purpose
The aim of this thesis project is to research and observe home care, a mobile workplace that will experience digitization in the near future and provide insights to possible developers and researchers within the field of eHealth and CSCW (Computer Supported Collaborative Work). The project, an iterative design process with the user in focus, explores and prototypes design solutions for supporting and improving the work life situation for night shift workers in home care. It focuses primarily on the needs of the caregivers, their relationships, communication practices, information exchange, documentation routines and the existing tools that they use today.
1.4 Motivation
Why Home Care?
Working as a sub-nurse within elderly care in Sweden was the most common profession in 2016, with over 138000 employees (Winqvist, 2018). Home care as an organization has been neglected for years despite reports from both employees, patients and relatives. It simply does not liv up to the quality of care the Swedish government pledge (Kalla Fakta, 2020). Kvarboendeprincipen (Socialstyrelsen, 2011), a part of the Elderly Reform Act, has been significant to elderly care politics in Sweden, and it values the individual living at home for as long as he or she wishes to. They suggest that health and social services should be moved to the people instead and receive individualized care according to one’s specific needs. Approximately 329000 elderly had some kind of help provided by social services in 2019 (Socialstyrelsen, 2020).
Why focus on night shift home care workers?
I have personally worked in home care for the past three summers and have first-hand experience on the home care situation in Malmö. Since beginning my Bachelor’s degree in Interaction Design, I have started to observe my workplace from a designer’s point of view, seeing possibilities where my field may be of use. I value my workplace and my colleagues and would like to see a change of attitude when approaching digitization in home care. I have worked morning, evening and night shifts, and I experience that night shift workers in particular are in a more vulnerable position as they are fewer in staff without office managers present.
1.5 Scope and delimitations
My experience from having worked in this field, will inherently play a role when I explore this topic. I will however strive to learn from and see the challenges from a designer's point of view: that is, to perform a truthful study with the extensive field research that this topic acquires and learn from the perspective of a designer. The priority of this thesis is to find a way to improve the home care workers’ situation of today with the Swedish eHealth goals that are set to 2025, and therefore future technologies will not be accounted for. Likewise, I will not be calculating the costs of implementing the concept as I will not deliver a finished product, nor have I considered other stakeholders. An outcome of the project is a deliverable that is produced from the needs of the end-users, home care night shift workers. However, I will point out the possible concerns for future work in the discussion. Additionally, due to exceptional circumstances under COVID-19 I did not have the opportunity to arrange larger group discussions and co-design practices with the home care workers, which I believe could have enhanced the credibility and quality of this project.
2 Background
In this chapter I will provide a background about what it is like to age in Sweden, what is offered and the existing technology that is used in home care.
2.1 Ageing in Sweden
The municipalities in Sweden provide home care both to the elderly and people with disabilities (Socialstyrelsen, 2011). With demographics that present a growing ageing population there is an expectant increase of elderly people that will require home care in the near future (Socialstyrelsen, 2019). According to The Global Age Watch Index (Mellgren, 2013), Sweden is still ranked to have the best living conditions for elderly. The average Swede is not affected by age related diseases until past the age of 78, and every tenth person born today is estimated to reach an age of at least 100 years (Ennart,
2011). When health, education, income, satisfaction and employment are measured, Sweden is in a leading position (Mellgren, 2013). Despite ranking high in well-being, there is a need for improvement and the quality of care varies between the municipalities. Today, 71% of elderly people above the age of 65 who live at home are using home care services (Socialstyrelsen, 2019). The amount of elderly people that require extensive home care, that is 25 hours per week or more, is estimated to increase from 300 000 to 450 000 people in less than 20 years (Forzati & Mattsson, 2014).
2.2 Home care
Receiving help in the home has been a priority since home care was introduced in Sweden in the 1950’s, to ease the workload for relatives living with their elders (Winqvist, 2018). Home care is offered everywhere in Sweden and is not geographically bound. The services that are offered can be divided into two main categories: service tasks and personal care (Winqvist, 2018). Cleaning, buying groceries and laundry are some of the service tasks that home care offers. Personal care can include getting dressed and undressed, preparing meals, personal hygiene and going for walks. The municipalities strive for the elderly to live as independently as they can and obtain a good quality of life in their own home. Moreover, an emphasis is put on individualized care, meaning that the caretakers are involved in the planning of their home care. It is built upon a mutual dialog and open communication between caretaker and staff. Time, continuity and flexibility are crucial for providing functional home care.
“Mutual caring relationships increase the opportunities for older persons to decide in accordance with their own
needs, to be free to decide whether or not they want to hand over to professional carers to decide for them, or to
decide for themselves or together with their carers.” (Winqvist, 2018, p.20.)
2.3 Existing technology
Efforts have been made in the last years to implement advanced digital services in home care (Forzati & Mattsson, 2014). These devices have first and foremost been developed to increase the safety of patients living at home. A by-product of these devices is to reduce the amount of physical visits from home care staff, thus saving time. As testified by the home care workers that I have been in contact with, there are a few digital services that are used today. There are new intelligent robotic systems today that could, for instance, execute certain routines such as personal hygiene without any home care staff being present. However, these are far from being implemented in Sweden and as mentioned, the focus of this thesis project is on today’s tools and technologies.
Sensors, cameras and
safety alarms
To ensure safety for elderly people that might suffer from dementia, sensors (Forzati & Mattsson, 2014) can be placed close to the bed and sound an alarm when there is any movement in the room during the night. Another solution that is used are remote cameras that
are activated once or twice during the night to confirm that the patient is in bed. This is an alternative for patients who easily wakes up from physical visits. Another way of ensuring that the elderly will not wander off in the middle of the night is door alarms. These small devices are activated from the outside and if the door is opened, it will alert an alarm receiving central. The fourth and final device is the most common one, a personal safety alarm (Malmö Stad, 2020). The tiny alarm has the appearance of a watch and is worn either around the patient’s wrist or as a necklace and provides a 24/7 service. In order to use it, press the red button, and help awaits.
Alarm center
All of the devices described above, in the event of being activated, automatically calls the alarm center. The alarm center receives the alarms, from all devices. Every patient who has a sensor, camera or alarm has an additional tiny speaker (See Figure 3) placed somewhere in their home. When the alarm center is alerted, they can talk with the patient through the speaker which also has a microphone. Later, the alarm center will call the assigned home care team to inform them about the alarm.
2.4 For the home care workers
The municipality of Malmö is currently using analogue solutions when it comes to the scheduling and handling of keys for entering patients’ homes. A few examples of digital solutions developed to be used by home care workers are in mentioned, but these are not used in Malmö and I cannot confirm how well they work.
Figure 3. Safety alarm and a speaker that is installed in the home of a patient (2019).
Figure 4. Viva Omsorg application, used in a car (Atea, 2018).
Viva Omsorg
Viva Omsorg (Atea, 2018) is an application that you use on a mobile tablet and is produced to be used by home care staff (See Figure 4). The tablet is carried by the home care worker when visiting patients to reduce time spent in front of the computer. The application contains information about patients such as address, relatives to call and a photograph of the patient. The employee can also see upcoming visits and information can be sorted according to needs. Documentation that otherwise is written at the office can be done in the patient’s home or in between visits.
Phoniro
Phoniro (See Figure 5) is an app that provides keyless home care. In the app, the employee will have the possibility of unlocking the doors of home care patients. By using digital locks, the home care workers do not have to carry heavy keychains nor does the patient need to worry about their keys being lost. With the same app, one can open medicine lockers, laundry rooms and gates (Phoniro, n.d.).
3 Previous research
Chapter two defined what it is like to age in Sweden and what is offered when you need help. It also described the most common technology used in home care today. Chapter three will be looking at previous research that is relevant to this project.
3.1 eHealth
The emerging field of eHealth is changing our view on healthcare as we know it and Erlingsdottir & Sandberg (2016) suggests that we can all expect to use an eHealth device at some point in our lives.
Figure 5. Phoniro digital lock, with an app (Phoniro, n.d)
eHealth is a can be defined as:
“An emerging field in the intersection of medical informatics, public health and business, referring to health
services and information delivered or enhanced through the Internet and related technologies. In a broader sense,
the term characterizes not only a technical development, but also a state-of-mind, a way of thinking, an attitude,
and a commitment for networked, global thinking, to improve health care locally, regionally, and worldwide by
using information and communication technology.” (Eisenbach, 2001, p. 1)
The Swedish government has formulated a national vision for eHealth where they identify three target groups that should be further examined: 1) individual citizens, 2) decision makers, and 3) healthcare and social care professionals. Erlingsdottir and Sandberg (2016) talks about the latter in their publication about eHealth opportunities and challenges. One of the major potentials of implementing eHealth is to increase efficiency by avoiding unnecessary actions. In some cases, some tasks are not possible to perform without an IT-based system which many times requires more thinking than should be necessary.
Achieving sustainable supportive systems in healthcare is a challenge, even though there are plenty successful implementations. Erlingsdottir and Sandberg (2016) claim that one of these challenges is to avoid poor integration with the actual work environment in which the tool will be implemented and used. Additionally, not much research has been done on the effects on the work environment after introducing the new tool. Erlingsdottir and Sandberg (2016) propose that the main focus when developing successful eHealth solutions for healthcare professionals should be on what people can do and not what computers can do. Frustration caused by outdated IT systems in combination with bad interface design can cause more harm than good. They suggest embracing the advancement of interaction design and user-centered design to aim for universal use. The concept of “situation-induced disabilities” draws attention to temporal impairments such as divided attention, walking, low levels of light and cold temperatures (Wobbrock, 2019). This concept concerns health care professionals in particular, who most likely will use a device in combination with other work tasks. Devices will not always be used in front of a desk and or by an average able-bodied person and therefore we should design accordingly if we want to achieve efficiency.
3.2 CSCW
Computer Supported Collaborative work, CSCW, has a long history of contributing to the healthcare sector through research and implementation of
technology to support healthcare professionals (Fitzpatrick & Ellingsen, 2013). CSCW examines how healthcare settings can be supported by digital systems designed to improve communication, information sharing and coordination, both asynchronous and real time collaboration. General ICT papers (Information and Communication Technology) are often measured in quantitative outcomes such as lowering costs or shorter hospital stays. CSCW on the other hand focus more on the qualitative data and values the complex findings through ethnographic research making it difficult to generalize insights that are relevant beyond a specific setting (ibid).
Mobility work is a concept that has become increasingly of interest in the field of CSCW when pointing out the limitation of deskbound computers (Bardram & Bossen, 2005). It can be used to understand why, when and how mobility occurs and to aid designers who develop computer support for people on the move. Bardram and Bossen (2005) talk about mobility in four different aspects; resources, places, knowledge and persons, meaning that mobility work involves the right combination of people, artefacts and information at the right time, highlighting that every artefact has its own place and purpose (ibid). They also point out that one almost never requires all information at once, but the essential information for a specific task and therefore it is important to not overwhelm users.
Recent CSCW research has focused on shift changes and patient handovers and the information that is assembled to pass on to the next shift. Tang & Carpendale (2007) point out in their observational study that information flow during shift changes between nurses at a hospital involves a diversity of media. The information is both communicated verbally, through electronic health records, paper-based patient care summaries, on whiteboards, charts and diagnostic results, all of which have their specific purposes. Numerous studies address the significance of whiteboards for facilitating social, spatial and temporal awareness that provide a glanceable overview (Fitzpatrick & Ellingsen, 2013). In addition to that, nurses have their own way of arranging different types of information on parallel documentation, informal notes that they carry with them (Tang & Carpendale, 2007). Bardram & Bossen (2005) also point out that the most recent information is provided verbally and stored mentally during shift changes due to the typical delay that comes with written information, which is a challenge for CSCW. Fitzpatrick & Ellingsen criticize the fact that there are few examples of technology prior to CSCW that has been implemented in a healthcare setting and remained fully integrated. The advantage of CSCW is that it promotes working from the inside out, instead of the opposite and encourages a participatory design approach. Designing interactive systems, which are structured for multiple purposes while at the same time being as flexible and collaborative as physical paper defines the complexity of working for digitization in healthcare.
As pointed out, recent CSCW research have had hospital settings as its primary focus, whilst eHealth is an attitude towards digitization in healthcare in general. I used the studies done in hospital settings, more specifically mobility work and information flow including both spatial and temporal
aspects, when doing my fieldwork research in home care. Additionally, CSCW studies emphasize that the focus should be on “supporting” the healthcare professionals, which I strived for in my project, rather than “replacing” them.
4 Methods
The previous chapter talked about research related to the field of healthcare and digitization. In the following I present the methods that have been applied to reach the aim of this project and answer the research question. A description of the methods is provided as well as why these methods have been selected, and how and when they are used.
4.1 User-centric design (UCD)
A user-centered design approach centers around gaining deep understanding of its users, empathizing with them. Still and Crane (2007) propose that instead of users evaluating a product at the end of a process, involving them from the beginning can contribute to a richer design process and a better product. Designing for use in context, keeping it simple and being transparent are a few of the UCD commandments that are suggested by Still and Crane (2007). In this project, UCD is the core of my design process. I began involving the users early on in the project and let the insights from the fieldwork research and usability tests guide my progress. The users served, in a sense, as part of my design team with whom I discussed and critiqued my design decisions during usability tests. Still and Crane (2007) suggest that the UCD process for developing a mobile application should look similar to the development of any other types of products. The interface of a mobile is significantly smaller than a deskbound computer and a common mistake that many designers do is to overwhelm users with information. Still and Crane (2007) advise a straight-forward approach to ”reduce, minimize and simplify” content on mobile applications. Do not assume anything about your users; focus instead on understanding them, not thinking that you already do.
4.2 The Double Diamond
The double diamond design process model provides a visual overview of how a design process can be conducted (Design Council, 2019). It illustrates “divergent” and “convergent” thinking and tackles a design process through four structured stages divided into two phases. It is an innovative framework that helps designers to tackle complex design challenges and focuses on understanding users, visually communicate ideas and collaborate. The double diamond encourages reflection and iteration to discover underlying problems
early on in the process. In the process of this thesis, the discover and define phases included desk research, field studies, analyzing the data and finding design opportunities. The discovery phase focused on empathizing with the user group and being attentive to the opportunities that I find, by focusing solely on the user group, home care employees, and finding their pain points would be the treasure of the first phase in the process. As suggested by the Design Council (2019), the project began very broad and empathized having an open mind towards the insights from the fieldwork. As I moved on to analyzing the fieldwork, I started defining the opportunities that I could work with. During the develop phase, I was open towards an iterative process with the users and made several prototypes with readjustments as I headed to the final usability test.
4.3 Literature review
To perform a true and liable case study I had to learn about Swedish home care and the goals of providing care at home. To get to know the contexts of eHealth and home care in Swedish settings I have used data from official papers provided by the government. In accordance with Muratovski (2016), I have also read both academic papers, journals and articles, and studied documentaries concerning the subject, to become knowledgeable within the area of research. To get a truthful picture of what home care in Sweden is today and the struggles that the organization is facing I gathered existing data to critically review. Literature reviews were conducted both before and during the project as an addition to the field research that was conducted.
4.4 Field studies
Three methods were used for field studies: semi-structured interviews and participatory observation (Muratovski, 2016). These methods are a few of many in the field of how to conduct ethnographic research. Ethnography is a research practice that enables the researcher to understand people in their typical environment (Muratovski, 2016). Through qualitative research, one aims to understand the nature of certain situations and settings: the relationship between people, systems or organizations. In this thesis, the environment in which I conducted the field studies was at the workplace, with my participants being home care workers. The area of interest was to analyze the existing information and communication flow that happens between and during shifts in everyday practice. I also aimed to discover the problems home care staff encounter during their shifts, their everyday struggles, concerns and opinions.
Participatory observation
Participatory observation allows the researcher to explore the nonverbal expressions of feelings and interaction between people and objects. It provides a holistic view of a community and one might be able to observe situations
that the interviewee discusses or chooses not to discuss in interviews. In this thesis, the observation was executed before the semi-structured interviews in order to understand the organization, the language and their work better, thus being able to ask relevant questions using proper terms. Participant observation is a branch of observation methods and is the beginning step in ethnographic data collection (Kawulich, 2005). It is suggested to determine what should be observed ahead of the observation in order to eliminate the irrelevant data. In this thesis, the participant observation focused on how the home care workers interact, with patients, nurses and other home care workers. What happens during a shift? Additionally, extra care was put into observing the objects they use regularly, how and when information is exchanged. Notes were taken during the observation and analyzed afterwards. The insights from the participant observation were considered when writing the interview questions and allowed me to collect data that I otherwise would have been unaware of.
Semi-structured interviews
The participatory observations were followed by semi-structured interviews. The aim of using a less formal interview style, semi-structured interviews, is to receive answers and insights that cannot be found in previous research (Muratovski, 2016). Additionally, being able to answer speculations and questions, striving for open-ended questions might invite more of a discussion and being more relaxed. Semi-structured interviews encourage a two-way conversation, but having questions prepared is necessary if the interviewee is hesitant when talking (Muratovski, 2016). Interviewing is a great method for confirming background research. The questions can also be adjusted according to each participant and their level of academic language. The insights from the participant observation were used to formulate relevant questions, with words and topics that make sense in a healthcare context.
4.5 Data analysis
With all of the insights, notes, quotes and questions, analyzing the data was an essential part of my design process.
Thematic Content Analysis
Coding is an essential part of the processing of data organization in most qualitative studies (Vaismoradi et al., 2016) Coding reduces and breaks down the data to manageable sections and is considered as one level of abstraction. It may aid the researcher to identify explicit meanings that are linked by a common theme or idea. Additionally, it may help the researcher to select appropriate information to accommodate the research question. It is important not to begin coding with a specific focus as it will interfere with the ability to recognize themes. The first step in the analysis of the raw data is to immerse oneself in the material and get familiarized with it. During the familiarization, it is important to take notes in order to later identify recurring words,
expressions and themes. Once the material has been reviewed, the researcher can attempt to identify key issues, concepts and themes. In this project I started to read and re-read the data in order to become familiar it. Later, I began marking words, sentences and observations that were of interest to use for the affinity diagram. I found that coding was essential to de-clutter my data, but the affinity diagram was better to use when visualizing the themes, thus making it more tangible.
Affinity Diagram
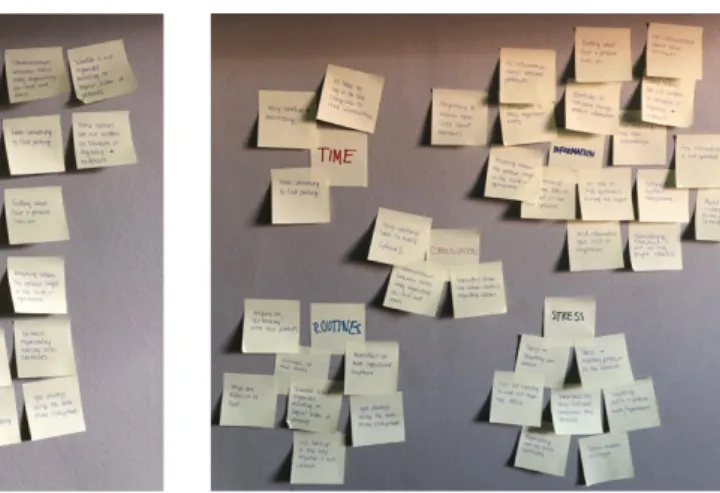
For processing and analyzing the data generated in the different phases of the exploration, affinity diagramming is a tool to organize the data and ideas. It is used to cluster information and sum up the major insights, user needs and pain points. Affinity mapping gives a complete picture of the early research process and provides a tangible overview of the insights (Kumar, 2013). In this project, all of the insights accumulated through the fieldwork research was clustered according to the thematics on post-its covering the wall in order to create a visual representation of the data.
Venn diagram
To make sense of the data and the insights, the Venn diagram method is used to indicate possible relations between the findings (Kumar, 2013). It consists of overlapping circles, where the designer can easily identify the connections between the thematics. The exterior represents the data, or insights, that are not related to the thematics within the circles and provides argumentation to why these insights were excluded. It is a visual method that is easily communicated to peers as well. In this study I used a Venn diagram to show the area of interest, where all five circles meet (See Figure 15).
Figure 6. Example of affinity diagrams
4.6 Ideation methods
After analyzing the data, gathering the insights and structuring the five thematics using the Venn diagram, it is time to start the design process. In this section I provide the ideation methods used.
Sketching
An important method throughout a design process is sketching (Buxton, 2007). As the design process begins with ideation and ends with usability testing, a large amount of time is put into sketching. The significance of sketching might be evident in a shorter design process with a low budget as sketches should be quick and timely as well as inexpensive and disposable. Additionally, sketches should suggest and explore rather than confirm, meaning that this is the time to challenge yourself and your design. In this thesis I began ideating on paper to explore the design space fully. I drew different scenarios, ideas and prototypes, later moving on to digital sketches.
Prototyping
A prototype is a concept in its early stage, a primitive version of something that will potentially be iterated over and over until it is a final product. Prototypes ranges from low-fidelity paper mockups wireframes and high-fidelity interactive prototypes. The choice of prototype depends on the questions you ask and the qualities you would like to test.
“Prototypes are representations of a design made before final artefacts exist. They are created to inform both design process and design decisions. They range from sketches and different kind of models at various levels — "looks like," "behaves like," "works like" — to explore and
communicate propositions about the design and its context.” (Buchenau & Suri, 2000, p. 1).
The model in Figure 7 represents three dimensions that are important to consider when designing an interactive artefact. In this project, the purpose of creating a low-fi prototype of the tool was to test the user flows, what makes sense in the way a user navigates through the tool? Afterwards, I moved on to a mid-fi prototype to explore and evaluate design ideas with the intended users in order to iterate and revaluate, its “role” and “look and feel”. Houde and Hill (1997) define “role” as “the functions that an artefact serves in a user’s life - the way of which it is useful to them” (House and Hill, 1997, p.3). What features are necessary to support the purpose of the prototype? Additionally, I explored the concrete experience of the tool and what it would be like to interact with it. It is pointed out by Houde and Hill that it is necessary to know
your users to decide what kind of fidelity the prototype needs to be to best support your idea. My users are a mix of experienced and less experienced technology users and therefore I
chose to present interactive prototypes, as visually and physically accurate as possible. This is so that, my users may imagine the tool being used and its’ role in their area of expertise and to criticize it accordingly and not be disturbed by its low fidelity. In this project I was more interested in what role the prototype could have for a night shift worker, and to do so I had to consider the “look and feel”
as well because the appearance is part of the experience.
Usability testing
The concept of conducting usability tests is to design products that enables the user to achieve their goals without frustration. Rubin and Chisnell (2008) point out that designing usable products is difficult, and design and implementation do not always match. Usability testing goes hand in hand with the basic principles of user-centered design, which include having an iterative design process and an early focus on users and their tasks. The overall goal of usability testing is to ensure that the product is useful and valued by the target users, easy to learn and easy to use. Rubin and Chisnell (2008) also points out the limitations of testing and that it is, despite efforts, always an artificial situation and one cannot prove that a product works. However, for the appropriate reasons, usability testing in this project was an essential step to improve the tool and its features. I created a usability test plan that accommodated the specific objectives that I wanted to explore and the research questions that I needed to answer.
User flows
There are many different ways to interact with a product, depending on the user’s motivation and goal. Creating a user flow can suggest the journey a user can take when interacting with a product and can be used to evaluate different design decisions. When it comes to interfaces, a user flow can be used to create an intuitive interface that is easily navigated by the user. If you find that the user flow is complicated, it is a good idea to re-evaluate the number of interactions. A successful design is created when the user can easily navigate through an interface without frustration and hesitation, which user flows can prevent (Still & Crane, 2007). In this project, creating user flows were helpful in evaluating the flow before creating an interactive prototype that would be tested on users.
Usability test 1 Usability test 2
Figure 8. The classic dimensions of what prototypes can prototype (Houde & Hill, 1997) with my usability tests included.
4.7 Ethical consideration
This project follows the ethical considerations described by the Swedish Research Council in “Good research practice” (Vetenskapsrådet, 2017). First of all, the manager in charge of the home care organization was informed about the project and signed a form approving the study and what field research methods were to be used. Secondly, all the participants were informed in detail about the project and the purpose of their participation. All of them read the letter of consent and approved it orally. The interviews were audio recorded and later transcribed. Contributions to the project were anonymized to prevent harmful information from being exposed. I purposely take into consideration what information I use and put in this thesis to protect the participants. I will not mention either name, age or gender, but define them as users with different technical backgrounds and/or experience of working in home care. In all the images that are used, I have purposely excluded faces and any features that can be connected to a person. All of which is in consideration to GDPR and to protect the participants.
5 Design process
The previous chapter described in detail what methods were used in this thesis. In this chapter I will present the field study material that are the basis for my design opportunity, ideation process and final result.
Literature studiesBackground research
Participant observation Interviews
Data analysis Affinity diagram
Brainstorming
Discussion with users Five themativs
Four design opportunities
Choosing design opportunity Concept sketches Storyboarding Wireframe Prototyping #1 Usability test #1 Usability test #2 Iterate Wrap up Prepare interviews Prototyping #2 Iterate Reflection
Discover
Define
Develop
Deliver
User flows
5.1 Field studies
The analyzed material was gathered during both participatory observations and semi-structured interviews. The data sets consist of images, audio recordings and field notes. These together with the literature studies serve as a foundation to insights gained and to the design opportunities. All of the collected fieldwork data was in Swedish and later translated to English.
In total one participatory observation was conducted during an entire shift, a total of 10 hours, with two full-time home care workers with several years of experience working in home care. During the participatory observation, I followed the workers for one whole night while taking notes and asking questions to get insights concerning the information flow and communication that occur during and between shifts and what type of media they are using. At a different occasion, individual semi-structured interviews were conducted with one temporary worker and one full-time worker at the office, in a separate room from other employees. The interviews lasted for ca 20 minutes each and were audio recorded.
The outcome of the field studies are reported in the following sections.
5.2 The essentials of a
night shift worker
Working in a mobile workplace means having all of the essential tools with you while working outside of the office. In Figure 8, we can see both a paper schedule, a pencil and an identification card and a mobile phone in the employee’s’ pocket (See Figure 10). These are a few of the items that they bring with them. This particular
home care worker wears reading glasses in a strap and a healthcare badge for sub-nurses as well. Additionally, they bring an alarm, which is to be used if the staff is threatened and has a built-in GPS that can be tracked by the police. The alarm and mobile phone are the two items that they are obligated to always have on them at all times. The night shift workers always work in pairs, one of them taking alarm calls and the other one is driving.
Information exchange at work
In this section I will describe the formal and informal communication and information flow that happens between and during shifts focusing on what objects are used. The four main objects are described individually as: paper schedules, mobile phones, computers and whiteboards.
5.2.1.1 Paper schedules
As mentioned earlier, Malmö municipality has still not introduced mobile digital schedules and patient information; therefore much information is still paper based. Every home care worker receives a paper schedule upon the beginning of their shift. Usually, it is a couple of pages worth of information that will guide you through the shift. The home care worker can find crucial patient information on the schedule including: name, address, time and the tasks that are to be done. It is also used to check off all of the visits, so that no one is forgotten. This paper schedule will travel with the employees throughout the night, and in the morning, they will put it in a binder to be archived. The schedule contains confidential patient information and it is very important to not misplace it. Paper is used throughout the shift to take notes of information that is relevant to inform the morning staff and to support the documentation that occurs at the office at the end of the shift.
5.2.1.2 Mobile phone
Every home care worker is required to carry one or two phones specific to each area division. The phones are provided by home care and contain the necessary phone numbers that you might need during your shift. Calling the nurse, 112, the alarm center, the stand-by manager, a locksmith and the other teams might be needed during a shift and these numbers should be in every phone. The phone itself is most likely a smartphone, but some teams are still using a push-button telephone (See Figure 11). However, the necessary actions do not require a smartphone. During a shift, home care workers will carry the phone in their pocket or close to them, being
prepared to answer the alarm center that delegates the alarms they receive. So, the first priority of using the phone is to receive alarms and communicate with other night shift teams and it is the primary tool used outside of the office to stay connected. During the participant observation, the phone was used several times per hour, most often for calls from the alarm center or using to call the nurse. When calling a nurse, the home care worker will be describing the current event in order for the nurse to evaluate what is the appropriate next
Figure 11. The phone the night shift workers used during the participant observation.
step. An example that occurred during the participatory observation was a patient whose catheter fell out, which requires a nurse to visit. However, the first people responding to the alarm and being physically present are the home care staff. Over the phone, the nurse asked what equipment was there and what kind of catheter the patient had in order to know whether he/she needed to bring more equipment. Before a nurse arrives, the home care worker will, to an extent, be the eyes and ears to of the nurse so that she or he can understand what needs to be done.
5.2.1.3 Computer
Using a computer is an essential part of documenting the events that happen during a shift. All home care employees should have a personal log-in to the computers and the programs that they use. The program used for documenting and finding patient information is currently only accessed through a computer. The employees have a responsibility to document any deviations concerning both the patient and the routines. Small details might become basis for patterns that will be analyzed by staff if there are recurring events with certain patients. For example, if a patient
deviates from his or her daily routine, that is information that should be documented. Ideally there should be time dedicated in the schedule for documentation, however, if the night is stressful the employees might not be able to document until later. One employee expressed that many times there is no time for documentation, meaning that deviations of the patients’ wellbeing, and patterns, will go unnoticed. The information that is written on the computer is publicly available documents, meaning that relatives and the patient herself are allowed access to the information. Therefore, it is crucial to be unbiased and formal when writing.
5.2.1.4 Whiteboard
Despite the fact that computers should contain first-hand information, the use of whiteboards to communicate is used throughout the shifts. It is easy to write, manipulate and erase information on the board (Fitzpatrick & Ellingsen, 2013). Usually, one will find information concerning employees that have called in sick and patients that are hospitalized or not home. The reason for using a whiteboard is that the whiteboard is the center piece of every room and therefore information that is written on it is rarely missed. All employees that enter the room will see the information, including the schedule planner, the manager and the nurse. During the participant observation, the home care
Figure 12. One of the computer rooms they use for documentation.
workers checked the board in every area to see if there was any last-minute information put up.
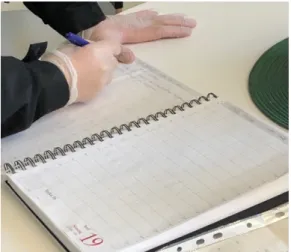
5.2.1.5 Notebooks
Notebooks are worth mentioning as most night shift teams have a physical notebook where they summarize their shift for the other team to catch up on the latest changes. The notebook contains informal messages, alerts or changes that are particularly important for the other night shift team. A home care worker described the notebooks as a way for night shifts to communicate with each other without physically meeting (See Figure 13). It usually concerns alarms or specific requests from patients that are not
documented on the computer. However, the home care worker points out that writing in the notebook is voluntary and therefore not everyone does it.
Table 1. Summarize of the objects that are used by home care workers, when, why and how.
Used for Used when Pros Cons
Paper schedule Patient information; name, address, key number, phone number, service and time. Taking notes, checking off patient
Throughout the shift, especially before and during. Easily manipulated, supports staff to find information, used for informal parallel documentation
Contains confidential information, limited information, easy to lose or misplace. Physically takes up space in pockets. Mobile phone Communicating with;
nurses, doctors, 112, alarm center, colleagues. Find essential phone numbers
Throughout the shift, several times per hour.
Always with them, quick way of communicating, direct, small device.
Relies on verbal information
Computer Formal documentation and accessing all available patient information
When and if there is time
Contains detailed patient information and patient history
Spatially bound to the office, time consuming and many steps. Not all substitutes have access. Whiteboard Last minute information,
relevant information about staff and patients
Before shifts to read After shifts to write and update Easy to manipulate. Spatially bound – the right information at the right place and time. The center of a room, hard to miss
Spatially bound – many rooms, many
whiteboards. Requires mobility.
Notebook Communication between shifts, informal information, relevant updates. Before shift to read. After shifts to write.
Be prepared for the shift and latest updates.
Irregular updates, not used by everyone.
Figure 13. The notebook the night shift workers use to communicate.
Key takeaways
The key takeaways from observing the artefacts that are used throughout the shift is that they all have their specific purpose and place in time (See Table 1). The paper schedule and the mobile phone are the only artefacts that are used “on the go”, meaning that all additional information can only be found at the office. It seems as if formal information is the most time consuming to access and also takes the longest to document whilst verbal information is a quick solution to save time. Additionally, the home care staff relies heavily on being able to contact the alarm center when being out of office to access very basic patient information. When a patient alarm sounds, the alarm center is the bridge between the home care workers and the patient. As described in chapter 2 (2.3.2), the alarm center receives all alarms and delegates them to the right home care team.
5.3 Five thematics
The previous section described the tools home care workers use to communicate, receive information and keep documentation. To process additional data that was gathered during the fieldwork, affinity diagrams (Kumar, 2013) were used to create categories and recurring topics (See Figure 14). With the affinity diagram I had the possibility of detecting patterns from the accumulated data which resulted in five thematics that are described below.
Time
As mentioned in the background research, issues with time are well known to be a problem in home care. Time with patients and time between patients are two of the main dilemmas that are currently being discussed. The schedule does not allow for deviations. During the interviews and observation, the more practical issues with time is the difficulty of finding legal parking. Spending valuable minutes circulating the residences is something that the car-bound night
Other than that, a busy schedule with many alarms might call for prioritizing visits and a discussion of how to do that properly. During both interviews and participant observation it was pointed out that finding the right key to patients is also time consuming, the current analog key system is outdated, and keys are easily misplaced. Time intertwines with all of the thematics in one way or another.
Routines
Prioritizing visits during stressful shifts is something that more experienced home care workers can do, as they know the area and their patients better. Being dependent on a home care worker knowing the routines and what to prioritize might not always be possible. A home care worker mentioned that relying on “gut-feeling” or “going with the flow” when receiving an alarm from a new or unknown patient is common. Home care does, of course, have routines for almost everything and how to operate in different situations. However, as with any other profession, there are routines that are not always written down on paper, or on a schedule: more specifically routines that happen in the homes of patients. These very specific details cannot be found written down anywhere which is also a reason for being hesitant towards new temporary workers. The job is not simply to follow a checklist but to provide individualized care for each patient. Where do I find Bruno's medical list? Should all lamps be turned off before leaving or does Agda want her bedroom lamp on? These small details are specific to each patient and are not mentioned on the schedule that the home care employees bring with them.
Information
The fact that routines are individual to each patient raises awareness of what information should be available and where one should be able to find it. Currently, additional information concerning patients can only be accessed via computer, through same software that the employees use to write documentation. The only information a home care worker carry with them is the information that can be found on their schedule, which is limited to a certain number of patients. An important insight is that most alarms occur whilst being out of office, in the car or while busy with another patient. During the participant observation, it happened several times that the alarm center called while the home care worker was unable to take notes and had to rely on remembering the information. Furthermore, if the alarm center calls regarding a patient that is not on the schedule, the home care workers do not have any information about the patient except the information that is provided by the alarm center. Crucial information concerning patients, for example whether they have a contagious disease is only available on the computer.
Communication
There is an evident lack of structured communication between the staff ending their shift and handing over information to the upcoming shift. The communication between shift changes concerns the most relevant information
that happened during the shift, if something occurred out of the ordinary that might affect the morning shift. This information is first and foremost communicated verbally, and if the morning staff are not present, it is noted on a whiteboard or in a notebook. The communication with the alarm center is positive even though it is dependent on verbal communication. The process of receiving and answering alarm calls are described in chapter 2 (2.3.2). However, I found out during the participant observation that when the home care workers arrive at a patient’s home, they must press a button on a tiny speaker that will connect them to the alarm center in order to confirm their arrival. This communication is essential to assure the alarm center that the alarm call has been received and completed.
Stress
All of the thematics that have been described above lead to stress. Additionally, stress adds to deviations from routines, forgetting information and miscommunication. An employee expressed that remembering important alarm calls after a stressful shift is difficult and sometimes it pops up on the way home from work.
5.4 Identifying design opportunities
After I had gathered all the insights that were accumulated through the research phase and put them on post-its, identifying, clustered them into themes that became what I call the “five thematics”. From there I tried to find similar insights and narrow them down to design opportunities (DO). For example, the insights concerning key information were transformed into one design opportunity. The process resulted in four workable design opportunities with a short definition and description. (See the Double Diamond process in Figure 9)
DO1: How might we design a key information system that is easy for the home care worker to access and update?
A few of the insights concerned the difficulty of locating and finding keys. First of all, they are located at different locations, geographically, depending on the area and it might be difficult to know in which area to find a particular key. Once at the office, there are sometimes multiple lockers spread out and information concerning what locker to look for does not exist. Additionally, the key register is messy, handwritten, rarely updated and therefore finding a key can take time – time that the employees do not have.
Figure 15. Venn diagram of the five thematics
DO2: How might we design a way for employees and temporary staff to learn the routines of new areas?
During both interviews and participatory observation, it was expressed that learning a new area is very difficult and therefore employees and temporary workers avoid rotating to new areas. An interviewee, a temporary worker, expressed that you rely on your co-worker to know the routine and schedule in an area. However, when there is no experienced co-worker present, which may happen occasionally and during summer vacation there is nowhere to turn for help. As mentioned in the introduction, there is an inadequate number of employees in home care and the amount of elderly inquiring services increases meaning that there might finding a way for new employees to settle is valuable.
DO3: How might we decrease the amount of information being lost during and between shifts?
Information lost between and during shifts is a current problem. Most of the communication is done and only later, if needed, documented digitally. It was expressed that information between and during shifts, deviations from the routines, is easily forgotten. During the participant observation, I noted that there is no “good” way of taking notes when being in the car, on the way to a patient or with a patient. So, the employees most likely rely on remembering information unless they can write down brief notes on a piece of paper. After several hours of working, one employee expressed that they had to start taking notes to remember all of the alarm calls and in what order they came in. DO4: How might we design an information system that is accessed by home care workers “on the go”?
As mentioned, Malmö municipality does not use digital schedules or have any digital information when being out in the field. Field research revealed that having digital information access when being outside of the office is something home care workers would appreciate in order to become more time efficient.
5.5 Early concept sketches
In the first steps of the ideation phase, I worked on all four design opportunities, brainstormed several concepts without any constraints in mind to see where I would end up. The design opportunities were still quite broad, but with the insights from the fieldwork studies I developed four concepts that were of interest to explore further. One of the ideas that I chose not to develop further was to create a “key vending machine”. The idea was to decrease the number of lost keys and rely on a digital key system, rather than physically taking the keys yourself. The idea was inspired by a previous workplace where you would pick the required clothes you needed for your shift through interacting with a digital interface. The machine registered what clothes you received and would register when you returned them.
After having evaluated the concepts developed, I decided to move on with ideas that focus on information on the go and with existing artefacts that they use. While the phone the most essential artefact on the go, it is only used for calling and receiving alarms I saw potential to make it more useful. I sketched four ideas, one that would support each design opportunity, and was later to have a discussion with a home care worker regarding the concepts.
The concepts were discussed and briefly evaluated by one home care worker on one occasion and then by two home care workers during a meeting at the office. The second meeting was focused on the attitude towards digitization.
Concept discussion with home care workers
I presented all four concepts to find out what concept to possibly continue with. It was pointed out that DO2, the “introduction to a new area” concept for new employees would be difficult to maintain updated as the schedule is constantly changing, and it would mean more work for the experienced employees who are already overworked. The conversation leaned towards DO3, the digital alarm register and DO4, mobile schedule. The employee asked whether it would be possible to create a hybrid between the two. Concerning the first design opportunity, updating and editing the key register is managed by office staff and is not relevant for night staff. However, the possibility of searching and finding key information from outside the office would be highly appreciated. The employee expressed a positive attitude towards the third design opportunity, being able to have an overview, history and information concerning the alarms. It would mean that one does not have to write down the information about the alarm whilst being on the phone with the alarm central, which in some situations is impossible as it requires both hands. “It happens quite often that I have to call back to the alarm center and ask for the name, address or key number as sometimes it’s just completely blank”. Additionally, the employee added, it would be great to see at what time the alarms came in and what the patient wanted in order to prioritize if needed. Prioritized alarms might be silent alarms or that the patient fell, feels ill or has a hard time breathing.
Two more home care workers were invited to discuss the concepts, where the themed conversation was digitization in healthcare. One of the home care workers was very positive to such change and the other one was reluctant towards it. A contributing factor to the resistance is the fear of having occasional system failures, for example with digital locks. Having issues with digital devices might add stress and time rather than the opposite. In addition to system failures, complicated interactions and unnecessary steps to perform a task seemed worrying as well. The other home care worker, who is pro-technology, has experience of an app that is used in Lomma. They use both digital locks and digital schedules. The worker expressed that all the information they needed was in the phone and therefore they did not need to bring anything else when they went out to see patients.
The insights gained from the discussion with the home care workers, lead me in the direction of focusing on DO3. To create a digital tool to keep track of the alarms, having access to basic patient information “on the go” and having an overview of the alarms throughout the shift. The benefits of such tool would be to avoid unnecessary actions, calls to the alarm center and delays in finding patient information. It would also support the home care workers to rely less on memorizing information. Additionally, one would have access to archived alarms from previous shifts as well as specific dates. The archives could possibly be used for multiple purposes: being updated on previous shifts alarms, finding patient information concerning patients that sounded their alarm the previous shifts and being more prepared.
First sketch
The first physical wireframe contained the essential screens that I would need to conduct a user test. The first feature that I focused on was “new alarms” or “incoming alarms”, meaning that the home care worker should be able to see what alarm calls they have waiting right now and access information about the alarm. The information that I included is similar to what one can find on the schedule; patient’s name, civic registration number, address and key number. Additional information that I decided would be useful was: what floor a patient lives on, if he or she lives with anybody, possible diseases that are infectious, whether they have a pet and contact information to a relative or trustee. The second feature I focused on was to access the “archives” or “history” of previous alarms during earlier shifts, for home care workers to access an overview of what happened when they were off work. The first sketches are depicted in figure 17 of how it could possible look like.
5.6 Prototyping #1
The first prototype consisted of wireframes, made in Adobe XD, for me to test out the idea in general on an iPhone 8 interface. As shown in figure 18, I connected the wireframes, made the buttons clickable and tested it out on my phone. After doing so, I continued to add color, icons and text to create my mid-fi prototype (See Figure 20) that would have the appearance of a finished product. Despite being time consuming, the reason for creating an interactive prototype in high resolution was for the users, the home care workers, to experience what it would be like interacting with the tool, to be independent during the user test to complete the tasks without me interfering
(Houde & Hill, 1997) . Since the prototype was created for an iPhone 8, I used principles from the IOS Human Interface Guidelines (Apple Inc., 2020). As proposed by the guidelines, I used a consistent theme throughout the interface and its components. The icons used and repeated had the same appearance and purpose in order to create a seamless experience. An overall fundamental design principle for mobile phones is to include only the necessary information and to make it intuitive. The first interactive lo-fi prototype was created for me to understand the connections between the screens and what made sense.
New alarms Alarm history
Patient info
Go back/exit
Choose date
New alarms Patient info
Go back/exit
Alarm history All alarms
Figure 18. The first digital wireframe of the “New alarms”, “Patient information” and “Alarm call history”.
Figure 19. The first sketch of the user flow.
Usability test #1
Before conducting the usability test, I filled out a one-page usability test plan dashboard (See Figure 21) to have a structured goal with test objectives and tasks. The aim of the first usability test was to determine what features are usable, if additional information needs to be added or removed and the overall notions of the tool from a user-centric point of view.
The first user test was done with two users, one who had been previously interviewed and one who I had followed during the participant observation. The user tests were separate and conducted at the office in a room where we could discuss openly. The procedure followed as depicted in the test plan (See Figure 21) starting with a brief introduction, following the user test itself where the users were asked to perform different tasks. After the test, we had
Figure 21. My usability test plan (Travis, D., 2017)