Cooking fuels and
children respiratory
health: Evidence from
Nigeria
MASTER THESIS
THESIS WITHIN: Economics NUMBER OF CREDITS: 30
PROGRAMME OF STUDY: Economic Analysis AUTHOR: Boishakhy Devi
1
Acknowledgement
Certainly, writing a master’s thesis during a pandemic is not an easy task! I have been highly fortunate for having a few great people around me who continuously pushed me and encouraged me to reach my ultimate goal.
First, I would like to express my gratitude to Anna Nordén, my supervisor, for her continuous support, constructive feedback, and valuable insights that have facilitated my thesis journey to successful completion. Thank you very much for giving me an opportunity to work under your supervision during this academic endeavour.
Then, I would like to thank my seminar colleagues and friends who have provided very good feedback during the regular thesis seminars. I am also grateful to all teachers and support staff at Jönköping International Business School (JIBS) who have enriched our academic journey and helped us prepare for a global career in the field of Economics. Further, I am thankful to the Demographic and Health Survey (DHS) Program for providing access to its dataset. Last but not least, I am highly grateful to my husband and my family members for their continuous mental support and inspiration that meant a lot during this master’s program.
Boishakhy Devi Jönköping, May, 2021
2
Master Thesis in Economics
Title: Cooking fuels and children respiratory health: Evidence from Nigeria Author: Boishakhy Devi
Tutor: Anna Nordén Date: 2021-05-24
Key terms: Cooking fuels, Children respiratory health, HAP, ARI, Modern fuels, Nigeria
Abstract
Household air pollution (HAP) has been recognized as one of the lethal causes of millions of premature deaths every year, victimizing mainly children and women. Literature suggests that transition to modern cooking fuels such as electricity, biogas from the conventional ones, for instance, fuelwood, coal, can reduce HAP, thus minimize the likelihood of respiratory health problems among household members. This study explores whether cooking fuels has an impact on children's respiratory health in the context of Nigeria, and in particular, whether modern cooking fuels can be a solution to this problem. By using the children recode of the survey data collected by the Demographic and Health Survey (DHS) for the year 2018, this study finds support to the claim that modern cooking fuels can reduce the probability of Acute Respiratory Infections (ARI) symptoms among children aged below 5 years in Nigeria. This probability is also found contingent on the age, gender, and education of the household heads. However, with regards to individual fuel types, the result seems inconclusive in some instances, mostly due to a lack of observations. The policy implication is that to reduce ARI among children, households should be encouraged to adopt modern cooking fuels, and this should follow with increasing education and empowerment opportunities for women in the household.
3
Table of Contents
1.
Introduction ... 5
2.
Theoretical Framework ... 8
2.1. Effects of conventional cooking fuels ... 8
2.2. Modern fuels – a remedy? ... 10
2.3. The case of Nigeria... 12
3.
Hypotheses ... 14
4.
Methodology... 15
4.1. Data ... 15
4.2. Model Specification... 16
5.
Results and Analysis ... 18
5.1. Descriptive Analysis ... 18
5.2. Probit Regression Analyses ... 18
6.
Discussion ... 24
7.
Conclusion ... 27
4
Tables
Table 1 Descriptive statistics of the variables ... 19
Table 2 Relationship between fuel types and ARI in children (probit regression analyses output) 22
Appendix
Appendix I ... 35 Appendix II ... 36 Appendix III ... 37 Appendix IV ... 39 Appendix V ... 405
1. Introduction
In the anthropocentric world, where we are living today, we depend on nature for various ecosystem services, i.e., the advantages that people obtain from ecosystems (Millennium Ecosystem Assessment, 2005). This study concerns one particular service – fuelwood for cooking and heating – that has received a lot of scholarly and practice attention in recent years. Traditional biomass fuels account for almost one-tenth of the overall energy required by humans around the world (Smith, 2006). This is even more pronounced in the cases of developing and least developed countries where almost 90% of the total rural household depend on conventional fuels for cooking, heating, and different household needs (World Resources Institute et al., 1998). Further, in another recent report, World Health Organization (WHO) stated that almost 3 billion people around the world, especially the ones from the developing and less-developed countries, use different wood-based fuels, charcoals, and dung for cooking (WHO, 2016).
Despite such dependence, the use of conventional cooking has been largely criticized as it leads to increased health risks related to the human respiratory systems. From the perspective of human health, the increasing amount of smoke emitted from fuelwoods leads to lethal health problems in the human body, particularly among women and children as they are more vulnerable due to being directly exposed to this smoke from indoor pollution (Oluwole et al., 2013). WHO also addresses this risk and extends the notion to cover other groups such as, elderly people staying at home in the list of vulnerable groups who are subject to a high risk of HAP. In fact, WHO estimates that HAP from cooking is responsible for 4.3 million premature deaths each year, which posits a serious concern among different stakeholders (WHO, 2016). Further, studies found that the need for cooking fuelwood is one of the main reasons behind long-term deforestation in many South Asian and African regions (Alem & Ruhinduka, 2020; Köhlin et al., 2001). This in turn negatively affects the overall biodiversity and climate condition in such regions while at the same time reducing the size of forests that could substantially contribute to the global economy by their carbon sequestration ability. At the same time, increasing deforestation pushes women to walk a longer distance to collect fuelwood, which not only contributes to different health problems but also reduces their time to do other activities (Das et al., 2019; Wan et al., 2011)
A potential remedy in this regard could be the initiation of modern cooking fuels and technologies, especially in the developing and least developed countries. This prescription is
6
also in line with the aspiration of the United Nations’ Sustainable Development Goals (SDGs), in particular to Goal 7 that aims to ensure affordable, reliable, clean, and modern energy services to households by the year 2030 (United Nations, 2015). While this aspiration holds, this thesis explores whether the proposed solution i.e., introduction to modern cooking fuel can reduce the associated respiratory health risks faced by children. The rationale behind my choice to investigate children’s respiratory health is informed by the fact that children are physiologically at a riskier position than adults. Gough (2019) presents three reasons claiming why children suffer more from air pollution. Firstly, children’s inhalation is 2-3 times faster than adults, which means they inhale 2-3 times more pollutants into their bodies when exposed to polluted air. Secondly, as children are in their early physical and mental development, their organs are also at a delicate development stage which puts them in a very vulnerable position. Exposure to pollution can cause both short-term effects like asthma and long-term lung impairment like lower lung volume. Finally, as the barrier between the bloodstream and the brain is at an initial development stage in newborn children pollutants reach the brain from the lungs through the bloodstream which further affects the child’s intellectual and cognitive development.
Given these premises, the research question of this thesis is,
Can transition to modern cooking fuels be a remedy to children’s respiratory health problems?
This study uses data from DHS (Demographic and Health Surveys) from Nigeria for the year 2018. Nigeria offers a unique setting to explore the research question being the most populous country in Africa with a high dependence on biomass and solid fuels that emit harmful smokes and pollutants that kill numerous lives every year (Obaseki et al., 2017; UNDP & WHO, 2009). Running a series of probit regression, overall this study finds support that compared to conventional fuel types, modern fuels are less likely to cause ARI among children aged below five in Nigeria. With regard to the sourcing of cooking fuels, Jagger and Shively (2014) argued that forest fuelwoods can show better results when it concerns children's respiratory health compared to the fuel alternatives collected from the non-forest areas such as fallows and bushes. To this, this thesis adds that modern fuels can offer a higher quality than the forest-based alternatives by reducing the likelihood of ARI among children. Further, this thesis confirms the effect of a few household-level characteristics on the choice of cooking fuel type (Jagger & Shively, 2014). In particular, it shows that the effect of fuel types on ARI
7
among children might be contingent on different household factors, such as the gender, age, and education of the household head. In particular, it suggests that highly educated female heads can play an important role in reducing the probability of experiencing ARI symptoms among children caused by emissions of household fuels.
The rest of the paper is organized as follows: section 2 presents a theoretical framework that reflects on the key terms and presents an overview of the context, which is then followed by a description of the hypotheses in section 3 and applied methodology in section 4. Section 5 presents the results of the analyses followed by a discussion in section 6. Finally, section 7 presents an overall conclusion along with theoretical and policy implications, limitations, and scope of future research.
8
2. Theoretical Framework
This section presents a review on the current stock of knowledge that discusses the environmental and health concern related to the use of traditional cooking fuels, the transition from traditional cooking fuel to modern cooking fuels, the challenges, and opportunities associated to achieve the proposed targets followed by a reflection on the research context, Nigeria.
2.1. Effects of conventional cooking fuels
On respiratory health
In the 2017 SDG Progress Report published by the United Nations, the current Secretary-General Antonio Guterres referred to HAP as the greatest environmental health threat of the present world (United Nations, 2017). Numerous studies also agree that smoke created from burning fuelwoods can cause serious health problems. For instance, in their seminal work, Naeher et al. (2007) claim that biomass combustion, for example, burning fuelwood emit a substantial amount of detrimental compounds such as poisonous carbon monoxide, nitrogen dioxide, particulate matter (PM), sulfur oxides, formaldehyde, and carcinogens into the air which can cause cancer. A study by Rehfuess (2006) also confirms the life hazard related to indoor smoke exposure.
The exposure to HAP is often far higher than the suggested international guidelines in the developing and least developed countries. In these countries, women are found more prone to death by chronic pulmonary diseases caused by HAP (Smith et al., 2004). The study further claims that women using conventional stoves are at threefold more risk to suffer from chronic obstructive pulmonary diseases (COPD), such as emphysema and chronic bronchitis compared to women who use clean energy like electricity or gas. Children are also at risk of being affected by these fatal diseases as women look after children while cooking. Rehfuess (2006) found that every year in South East Asia and Africa over 600,000 children of age under 5 years die due to pneumonia and other severe respiratory infections caused by HAP. Studies also reveal that children who live in houses using biomass as fuel are at two to three times higher risk to develop ARI compared to the children living in houses using cleaner fuels (Barnes et al., 2010; Fullerton et al., 2009; Khalequzzaman et al., 2007). While the adults are likely to develop ischaemic heart diseases, stroke and chronic obstructive pulmonary diseases, and lung cancer, the children are affected by acute lower respiratory infections (ALRI). ALRI is a more
9
dangerous type of ARI which is responsible for nearly 50 percent of all deaths caused by indoor air pollution. This is the most important cause of child death up to five years of age in developing countries.
It is estimated that roughly 50 percent of all deaths attributable to HAP are caused by ALRI among infants and children (Rinne et al., 2007; Torres-Duque et al., 2008; WHO, 2002). Among infants and children who are exposed to indoor cooking smoke, cases of severe diseases like acute bronchitis and pneumonia are very commonly seen as their immunity towards these respiratory diseases is weakened (Bizzarri et al., 2010). In addition to the respiratory health issues, Cooke et al. (2008) found that indoor smoke can cause diseases like blindness and adverse pregnancy outcomes. Researchers also found evidence of women being affected by high blood pressure during pregnancy when exposed to HAP, causing the birth of underweight children, and increasing chances of childhood pneumonia (WHO, 2018).
Other effects on household
Further, with a high dependence on biomass and solid fuels, the scarcity of fuelwood also increases, which causes women to invest more time in the search and collection of fuelwoods taking away their time from other important activities like childcare, food preparation, agriculture, and often they lose scope to gain educational opportunities (Colfer et al., 2008). Given the lives of women are strongly interlinked with the lives of children, as women suffer from the adverse effects of deforestation, so do children. According to the World Health Organization Global Health Observatory Data Repository, in 2013 the number of children living in homes that use solid fuels in cooking and heating was 352 million. It is observed that children of age under 5 spend more time near cooking areas as they depend on their mothers. Mothers often carry young children on their back while cooking in the kitchen or areas near the kitchen (Oguntoke et al., 2010), making them similarly subjected to fuelwood smoke. Girl children are more exposed to indoor pollution since they help their mothers in cooking and help them in other household chores (Dasgupta et al., 2006). In many low and middle-income countries, women and girls act as the main collectors of fuel for cooking. In addition to the health issues faced by children, their scope to gain education is hampered too as they also help their mother in fuelwood collection. WHO (2016) reports that girls living in households that cook with polluting fuels spend 13 more hours per week on average for gathering fuel than girls living in households using clean fuels. This time could be spent more wisely in learning or at play.
10 Effects on the environment
The collection of fuelwoods is one of the key reasons behind increased deforestation. Scholars estimate that roughly 40 percent of the total rates of deforestation can be associated with
fuelwood collection (Barber et al., 1994; Myers, 1994). Bailis et al. (2015) claim that of the total amount of wood harvested worldwide, more than half is used as fuel, providing approximately 9 percent of overall primary energy. The increased rate of deforestation for fuelwood collection largely prevails in the developing and least developed countries (Mallo & Ochai, 2009; Repetto, 1990). For instance, Ayuba and Dami (2005) noticed that in the rural parts of northern Nigeria, fuelwoods account for 92% of the total fuels used in household cooking, mostly due to the availability and cheap price of fuelwoods. In Sudan, the total forest cover of the country substantially dropped by around 50% in the course of four decades from 1950 to 1990 (MEPD & HCENR, 2003). The situation prevailed in a later study conducted by Alam and Starr (2009). A similar scenario is observed in the case of Ghana. Once used to be a Carbon-dioxide (CO2)emission remover country, Ghana experienced a continuous fall in its
amount of CO2 removed, which can be attributed to a sharp growth in the consumption of
fuelwood (Ghana NatComm, 2000). At the same time, the collection methods of forest fuelwoods often deviate from sustainable management practices, which further worsen the overall scenario (Von Schirnding et al., 2002).
Further, irresponsible consumption behaviors release lethal gases like CO2, methane,
chlorofluorocarbons, etc. to the atmosphere (Silver & DeFries 1990). Studies expect an increase of 2-5 ℃ in the global climate due to the doubling of CO2 release (Ellis, 1991;
Revkin,1988; Royer and Mahouf, 1992). Furthermore, deforestation makes the weather hotter and drier, consequently, give rise to desertification and drought, melting of the polar ice caps, flooding in the coastal areas of the low-lying lands, to name a few. The overall biodiversity is also affected when deforestation occurs. In the past extinctions were driven by natural processes but in the present time extinctions of different species of plants and animals occur due to various human activities including deforestation (Boahene, 1998). All these call for more attention to be paid towards the consumption of forest-based fuel types.
2.2. Modern fuels – a remedy?
There have been numerous studies and experiments conducted in different parts of the world in the quest for viable alternatives to conventional cooking using fuelwoods. Many large-scale
11
initiatives largely motivated by concerns about deforestation and fuel scarcity were made in the past, involving national programs in China in the 1980s and India in the 1990s. The aim was to develop “improved” stoves focusing on improving fuel efficiency relative to traditional stoves and open fires (WHO, 2016). The report by WHO (2016) also suggests that the improvement of combustion efficiency results in the reduction of the amount of pollution produced from cooking, heating, or lighting fire, thus reduces the exposure to HAP. Thus, they suggested installing more cleaner sources of energy in the household.
Jagger and Shively (2014) found that the likelihood of children suffering from ARI due to HAP might be contingent on the fuel type used in the household. Further, studies found that in households that use non-biomass modern fuels such as electricity and gas, inhabitants, especially females who spend long-time cooking, are less likely to experience long-term respiratory diseases such as asthma, lung infections, etc. (Liu et al., 2020; Oluwole et al., 2013; Sapkota et al., 2008). For instance, the switching from traditional ways to modern fuels and cookstoves in Ethiopia and the use of biogas in Vietnamese farm households lowered the emission of harmful greenhouse gases compared to burning fuelwood (Izumi et al., 2015; Mondal et al., 2018). In the rural parts of Nepal where women and children are also sufferers of indoor air pollution, a unique public-private partnership initiative named the Biogas Sector Partnership (BSP) successfully installed more than 260,000 household biogas systems across all of Nepal’s 75 districts which resulted in improving rural lives. (WHO, 2016).
Apart from the impact on respiratory health, the use of modern cooking fuels might also influence the daily activities of children in many other ways. For instance, in underdeveloped and developing countries, it is common to see children engaged in the collection of fuelwood which reduces children’s participation in school. To this, Ding et al. (2014) found that with households getting access to modern cooking fuels, the time spent on the collection of fuelwood and cooking gets reduced, which leads to participation in social activities. Further, studies also found that the use of modern fuel raises school attendance, children’s performance, and decreases sick days related to HAP. Besides, in Tanzania, it was found that modern fuel use is related to the continuance of post-primary education (Levison et al., 2018; Ndiritu & Nyangena, 2011).
However, access to modern fuels such as electricity, LPG, natural gas, and biogas, has been very limited in the developing and least developed countries. A joint report by UNDP and WHO shows that only a tiny percentage of the population in these countries, especially in the sub-Saharan region uses modern cooking fuels, leaving the majority of the population highly reliant on biomass fuels, in particular, fuelwood collected from forests, and again, most of these
12
fuelwood users are also highly dependent on traditional cooking stoves that are likely to produce a lot of smoke leading a high HAP (UNDP & WHO, 2009). This is important, as according to the benchmarks WHO recommends for better burning, the appropriate fuel must be used in the right stove to get the best results. For example, if a “modern” fuel like liquified petroleum gas is burnt in an inappropriate stove it might produce large amounts of pollution. Similarly, if traditional stoves are used to burn processed biomass fuels like pellets and briquettes they may burn incompletely. That being said, switching to modern alternatives from the conventional fuel types often requires a substantial amount of initial and recurring investments for refueling purposes which the poor people living in these developing and least developed countries can hardly afford (Faizan & Thakur, 2019; Nayak et al., 2015; Zulu, 2010).
2.3. The case of Nigeria
Nigeria offers an appropriate context to explore the impact of fuel type on children's respiratory health, as it is one of those countries carrying the heavy burden of child death. A recent report developed by the World Bank finds that only in 2018, 11,200 premature deaths occurred in Lagos, Nigeria, due to respiratory health problems, of which 60 percent accounted for children under the age of five (Croitoru et al., 2020). WHO ranked Nigeria as 3rd on the list of top 10 countries using polluting fuels as the primary energy source for cooking. This report also shows that in Nigeria less than 5% of the total households primarily rely on clean cooking fuels whereas the population primarily relying on polluting fuels for cooking is more than 173 million (WHO, 2016). In particular, this is highly evident in the rural areas where the lack of inexpensive alternative energy sources results in excessive dependence on fuelwood for household energy supply (Oguntoke et al., 2013).
Several studies have investigated the harmful impact of HAP in the Nigerian context. For instance, investigating 269 women in Nigeria, Desalu et al. (2010) found that women who are reliant on conventional fuels are more likely to suffer from respiratory diseases such as chronic bronchitis than the ones who use non-toxic, cleaner alternatives, such as electricity and gas. Then, studying 74 women in the Olorunda community in Nigeria, Ana et al. (2013) also noticed that women who are exposed to smokes emitted from fuelwood are highly likely to suffer from different respiratory diseases. In a similar vein, investigating rural school-going children in Nigeria, Oluwole et al. (2017) found an association between the use of conventional fuels and increased risk of asthma. On the contrary, studying 299 village children aged between 5 - 11 in Northern Nigeria, Thacher et al. (2013) did not find any strong association between
13
exposure to household smoke and increased risk of asthma. Nevertheless, these studies are inconclusive and are mostly based on a relatively lower sample of observations focusing on a particular region. To this debate, the current study adds fresher insights as it reflects on the impact of fuel types on the respiratory health of children below 5 years along with a few other control variables based on a recent data set prepared by a professional body that had conducted large scale surveys with a substantially larger size of Nigerian respondents.
14
3. Hypotheses
The thesis aims at exploring the effect of different fuel types on children's respiratory health in the context of Nigeria. In particular, it examines whether different fuel types used in households may influence the likelihood of children living in households experiencing respiratory health problems due to the smoke emitted from the fuel usage. Guided by Jagger and Shively (2014), in this thesis, I explore the relationship between different cooking fuels and childrens' respiratory health using DHS data for Nigeria collected in the year 2018. Given the holistic economic development that had taken place in recent years in the sub-Saharan region, I expect that there might have been some notable changes in the fuel consumption patterns in this context Nigeria, that might better inform us whether the findings of the prior work hold. Thus, I hypothesize that the probability of experiencing ARIs among children is related to the fuel type used in the household. More explicitly, I test the following hypotheses,
H0 = Type of fuel used in a household has no impact on the likelihood of
experiencing ARIs in children in Nigeria
H1 = Type of fuel used in a household has an impact on the likelihood of
15
4. Methodology
4.1. Data
As the study aims at exploring the relationship between fuel type and children’s respiratory health, I used the children recode of the survey data collected by the Demographic and Health Survey (DHS) for the year 2018. This is the most recent data available on the DHS platform for the given context, Nigeria. The data consists of 33,924 individual-level observations responded by women in Nigerian households. The survey addressed a host of questions covering a wide range of topics. Of these, two variables address respective symptoms of cough and rapid short breath observed among the children aged below 5 years during the last two weeks before the survey was conducted. I considered them combinedly to generate my dummy dependent variable, ARI. The rationale behind choosing the combined symptoms is guided by the fact that these symptoms alone can be caused by different diseases, however, is very likely as a symptom for ARI when observed together (Jagger & Shively, 2014). Then, as my independent variables, I worked with all fuel types, both individually and combinedly denoting modern and conventional cooking fuels, along with age, and gender of the household head, and education level. The rationale behind working with these variables is explained in the following section that presents the estimation models. Appendix 1 provides an explicit list of survey questions asked for each variable used in this analysis.
After selecting the variables, I ran some summary statistics to get a first look at the data. I noticed multiple variables consisting of missing data, especially when it concerns reporting symptoms of cough or rapid short breath. The reason behind these missing data was simply due to the absence of a child below 5 years of age in the household investigated. As I consider the combined effect of these two variables to address ARI expressed in a dummy variable, where 1 denotes the combined effect or 0 otherwise, I omitted the missing variables, which otherwise could influence the overall study, i.e., by being included under the label 0. Further exploring the data, I noticed in the variable fueltype, 444 observations were collected from individuals who were not de jure residents, thus, omitted these observations as well. In a similar vein, I also discarded 10 observations that denoted no food cooked in the household surveyed. Doing so, the final number of observations became 30,285. Then, as the age of the individuals was expressed in a continuous variable, ranging between 15 years to 98 years, I converted it to a categorical variable with a minimum value of 0 to a maximum value of 100 distributed in 4 categories with an equal gap of 25 years, so that instead of reporting the predictability for each age year, I could estimate the impact on different age groups.
16
4.2. Model Specification
To examine the relationship between fuel types and ARI, I estimate a series of probit regression models based on the model used in the study of Jagger and Shively (2014). To estimate the probability of ARI among children, the first two models consider all fuel types combinedly distributed among modern and conventional fuel categories to get an overview of the overall performance of modern fuels over conventional ones. These models are expressed as,
P(ARI=1|modernfuel) = Φ(β0 + β1modernfuel) … (1)
P(ARI=1|modernfuel, agehouseholdhead, sexhouseholdhead, education, sexhouseholdhead*education) = Φ(β0 + β1fueltype +β2agehouseholdhead +
β3sexhouseholdhead + β4education+ β34(sexhouseholdhead*education) …. (2)
Then, to further test the effect of each individual fuel type on the likelihood of ARI among children, two additional models are run which are expressed as,
P(ARI=1|fueltype) = Φ(β0 + β1fueltype) … (3)
P(ARI=1|fueltype, agehouseholdhead, sexhouseholdhead, education, sexhouseholdhead*education) = Φ(β0 + β1fueltype +β2agehouseholdhead +
β3sexhouseholdhead + β4education+ β34 (sexhouseholdhead*education) … (4)
For both considerations of fuel types, i.e., individual and collective, ARI is predicted both without and with control variables to explore whether there is any effect of different household characteristics on the overall estimation models. The calculation is conducted using the statistical software, STATATM.
The dependent variable, ARI is a binary variable, which is equal to 1 when a child is reported to show a combined symptom of cough and rapid short breath during the two weeks before the surveys were conducted, and 0 otherwise. The DHS dataset provides a list of 11 individual fuel types (see, Table 1). Based on these variables, I created a binary independent variable modernfuel, which is equal to 1 when electricity, liquefied petroleum gas, natural gas, or biogas is used in the households surveyed, and 0 otherwise. This independent variable, modernfuel is then used in the first two models to estimate the probability of ARI in cases of
17
households using either modern or conventional cooking fuels. Then, to estimate the probability of ARI for each individual fuel type, a categorical independent variable fueltype is used, which covers all 11 types of cooking fuels used in the household (see, Table 1). It also covered some observations of no food cooked in the household and responses collected from not a de jure resident i.e., the member is not a usual resident of the household surveyed (Demographic and Health Survey, n.d.); however, both of these responses were dropped before running the probit regression as they do not add to the research purpose.
Even though the observations are individual, three household-level characteristics are controlled for when conducting the regression. Among them, two accounts for the gender of the household head and education of the respondents expressed as sexhouseholdhead and education respectively. The rationale behind using these control variables is motivated by scholarly findings that suggest households consisting of educated female heads are highly likely to consider modern cooking fuels and technologies over the conventional alternatives that are often unsafe with regards to respiratory health (Alem et al., 2013; Jagger & Shively, 2014). Thus, I also considered an interaction term between the gender of the household head and their education level. Further, I controlled for the age of the household head, expressed as agehouseholdhead, which was also applied in the study of Jagger and Shively (2014) to see whether the age of the individual leading a household has some impact on the probability of experiencing ARI among children.
18
5. Results and Analysis
5.1. Descriptive Analysis
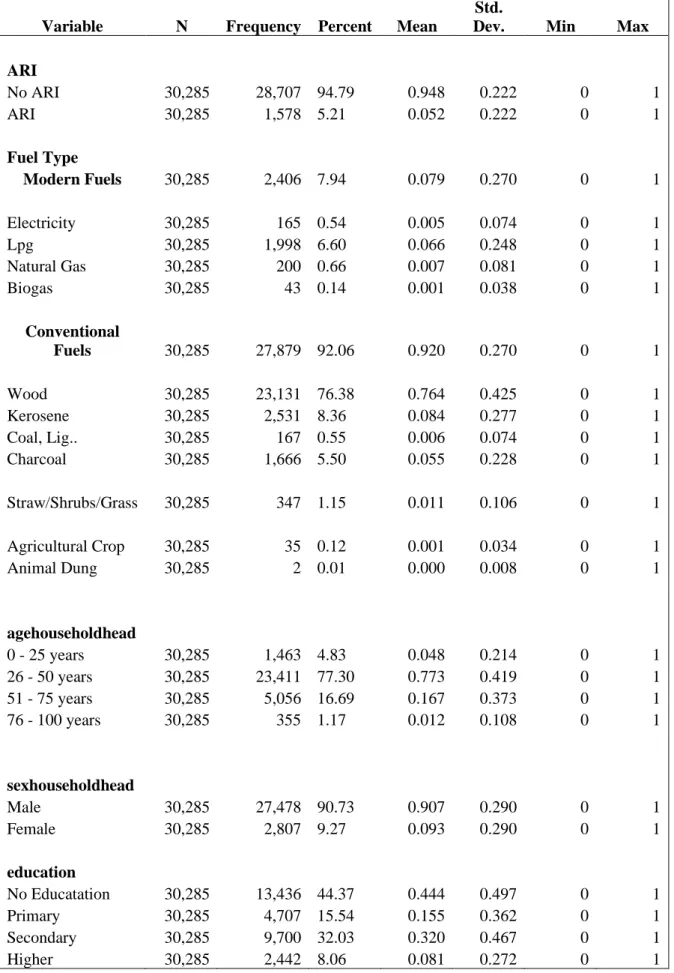
First, let us have a look at the descriptive statistics of the variables used in this study and presented in Table 1. To start with our dependent variable, ARI, we can see that of the total observations analyzed, 1578 individuals (5.21%) reported a combined symptom of ARI whereas the rest either had only one symptom or none within the last two weeks before the survey. In terms of the fuel types used, the surveyed households show a huge dependence on conventional fuels (92.06%) compared to modern fuels (7.94%). Among the conventional ones, wood is the most widely used fuel by households accounting for (76.38%) whereas liquefied petroleum gas, LPG, accounts for the most common modern cooking fuel (6.60%). It should be mentioned that all respondents reported only one fuel type being used in the household, thus, the dataset excluded information on whether any households were using multiple fuel types. Most of these households had a male household head (90.73%) who would be most likely to belong in the age group between 26 – 50 years (77.30%). With regards to the education of the individuals surveyed, i.e., the women, around half of them received no education (44.37%), and there were only a few who could avail themselves an education beyond the secondary school level (8.06%).
5.2. Probit Regression Analyses
The first two models estimate the probability of ARI when fuel types are combinedly categorized between modern and conventional ones without and with controlling for the above-mentioned household characteristics, respectively (see, Table 2). Both these models support the hypothesis that there is an impact of fuel type on the likelihood of experiencing ARI among children in Nigeria. We find that modern cooking fuels provide significantly better results when it concerns ARI among children. Specifically, the first model shows a 1-unit increase (what we can safely assume as 100 kg, ref. Jagger and Shively (2014) in the consumption of modern cooking fuels decreases the likelihood of finding children with ARI symptoms by 2.1%, which, however, gets reduced to 1.6% as per the second model, when is controlled for household characteristics i.e. gender and age of the household head, education of the respondent. We see that as the age of the household head increases the likelihood of ARI decreases until a certain point, specifically the second model shows that likelihood of ARI among children is significantly decreased by 2% in the households that are led by individuals aged between 51 to 75 years, and then it slightly declines. An interpretation of this can be that
19 Table 1 Descriptive statistics of the variables
Variable N Frequency Percent Mean
Std.
Dev. Min Max
ARI No ARI 30,285 28,707 94.79 0.948 0.222 0 1 ARI 30,285 1,578 5.21 0.052 0.222 0 1 Fuel Type Modern Fuels 30,285 2,406 7.94 0.079 0.270 0 1 Electricity 30,285 165 0.54 0.005 0.074 0 1 Lpg 30,285 1,998 6.60 0.066 0.248 0 1 Natural Gas 30,285 200 0.66 0.007 0.081 0 1 Biogas 30,285 43 0.14 0.001 0.038 0 1 Conventional Fuels 30,285 27,879 92.06 0.920 0.270 0 1 Wood 30,285 23,131 76.38 0.764 0.425 0 1 Kerosene 30,285 2,531 8.36 0.084 0.277 0 1 Coal, Lig.. 30,285 167 0.55 0.006 0.074 0 1 Charcoal 30,285 1,666 5.50 0.055 0.228 0 1 Straw/Shrubs/Grass 30,285 347 1.15 0.011 0.106 0 1 Agricultural Crop 30,285 35 0.12 0.001 0.034 0 1 Animal Dung 30,285 2 0.01 0.000 0.008 0 1 agehouseholdhead 0 - 25 years 30,285 1,463 4.83 0.048 0.214 0 1 26 - 50 years 30,285 23,411 77.30 0.773 0.419 0 1 51 - 75 years 30,285 5,056 16.69 0.167 0.373 0 1 76 - 100 years 30,285 355 1.17 0.012 0.108 0 1 sexhouseholdhead Male 30,285 27,478 90.73 0.907 0.290 0 1 Female 30,285 2,807 9.27 0.093 0.290 0 1 education No Educatation 30,285 13,436 44.37 0.444 0.497 0 1 Primary 30,285 4,707 15.54 0.155 0.362 0 1 Secondary 30,285 9,700 32.03 0.320 0.467 0 1 Higher 30,285 2,442 8.06 0.081 0.272 0 1
20
after a certain age, here in our sample after 75 years, a household head might be not strong enough to control or influence household decisions with regards to the fuel consumption choice, as their sons and daughters might already emerge as an important, decision-making figure in the household. Further, in line with the literature, we notice that when the women are highly educated the likelihood of ARI among children gets reduced by 1.05%, and this can be further reduced by 1.83% when the households are led by women with highly educated women. These inverse relationships hold when considered the interaction effects between gender and the education of the household heads. Even though the results are not significant, the marginal effects show that a highly educated female head might contribute to better fuel choice thus reduce the likelihood of ARI among children than an uneducated female head.
The third and fourth models estimate the probability of ARI among children for individual fuel types. Again, both models suggest that there is an impact of fuel type on the incidence of ARI, thus rejects the null hypothesis that there is no relationship between fuel type and the likelihood of ARI in children. In both models, wood is used as the baseline reference group, and evidently, all individual fuel types, be it a modern or conventional one, reduce the likelihood of experiencing ARI among children compared to what it would be otherwise due to using wood as the household fuel. Among the modern fuel types, electricity comes out as the best possible alternative compared to wood and can reduce the likelihood of ARI among the children by 3.33% and 3.31% when estimated without and with control variables, respectively. On the other hand, biogas shows comparatively weaker marginal effects in both models, which might be due to the limited number of observations reported for this fuel type. However, with regards to the conventional ones, it was very surprising to see coal lignite suggesting a better performance than electricity when compared against wood as the household fuel type. Based on the probit results, it can be said that a 100 kg increase in coal, lignite consumption as the household fuel might be associated with a 4.5% decrease in the likelihood of ARI, both with and without control variables, compared to fuelwood. Again, we can assume that this has been the case due to a few numbers of observations accounted for this particular fuel type. Apart from these, agricultural crop residues and different types of shrubs, straw, and grass are found to show relatively lower effects on ARI than many conventional and modern fuel types. Besides the fewer numbers of observations reported for both of these fuel types, one can also assume that households that use agricultural crop residues as fuels might be from well off conditions who experience higher agricultural yields, ensuring an overall better nutrition plan for their children (Jagger & Shively, 2014). It could also be that these two fuel types were temporarily used in the households when the survey was conducted and thus
21
led to a fewer number of observations. However, this assumption could not be verified as DHS recode manual did not provide any hints on whether these households were using a mix of different types of fuels (see, Demographic and Health Survey, n.d.). Nevertheless, with regards to the control variables and interaction term, model 4 resonate the findings of model 2, i.e., there is a likelihood of better performance concerning ARI among children when the household head belongs to 51 – 75 years of age group, and this can be further improved if the household head is a female. Educated females are found to contribute to reducing ARI likelihood among children. Also, similar to model 2, the analysis shows that marginally, female heads with higher education can better contribute to the reduction of ARI likelihood among children compared to an uneducated female head. The estimation of all four models individually is also presented from Appendix II to Appendix V.
22
Table 2 Relationship between fuel types and ARI in children (probit regression analyses output) a,b
Model 1 - ARI and modern fuels (without control variables)
Model 2 - ARI and modern fuels (with control variables)
Model 3 - ARI and individual fuel types (without control
variables)
Model 4 - ARI and individual fuel types (with
control variables)
Estimated Coefficient
Marginal Effect Estimated Coefficient Marginal Effect Estimated Coefficient Marginal Effect Estimated Coefficient Marginal Effect Fuel types
Modern Fuels (c.f. Conventional fuels) -0.237*** (0.051) -0.021 -0.174*** (0.055) -0.0163 - - - - Electricity (c.f. wood) - - - - -0.398* (0.211) -0.0333 -0.372* (0.211) -0.0316 Lpg (c.f. wood) - - - - -0.269*** (0.056) -0.0250 -0.238*** (0.061) -0.0226
Natural gas (c.f. wood) - - - - -0.237
(0.169) -0.0225 -0.202 (0.170) -0.0197 Biogas (c.f. wood) - - - - -0.104 (0.330) -0.0110 -0.092 (0.332) -0.0098 Kerosene (c.f. wood) - - - - -0.234*** (0.049) -0.0224 -0.224*** (0.051) -0.0215
Coal, lignite (c.f. wood) - - - - -0.682**
(0.270) -0.0456 -0.674** (0.271) -0.0450 Charcoal (c.f. wood) - - - - -0.180** (0.057) -0.0180 -0.177** (0.058) -0.0176 Straw/shrubs/grass (c.f. wood) - - - - -0.323** (0.137) -0.0288 -0.311** (0.138) -0.0278
Agricultural crop (c.f. wood) - - - - -0.327
(0.431)
-0.0290 -0.354 (0.419)
-0.0306
Age of the household head
26 - 50 years (c.f. Age≤25) - - -0.136** (0.053) -0.0161 - - -0.130** (0.053) -0.0152 51 - 75 years (c.f. Age≤25) - - -0.174*** (0.059) -0.0200 - - -0.178** (0.059) -0.1202 76 - 100 years (c.f. Age≤25) - - -0.168 (0.124) -0.0194 - - -0.178 (0.125) -0.0202
23 Female-headed household (0=No; 1=
Yes) - - -0.089 (0.093) -0.0083 - - -0.062 (0.093) -0.0067 Education Primary (c.f. no education) - - 0.075** (0.035) 0.0095 - - 0.088** (0.036) 0.0106 Secondary (c.f. no education) - - -0.035 (0.030) -0.0038 - - 0.008 (0.031) 0.0005 Higher (c.f. no education) - - -0.097* (0.057) -0.0105 - - -0.027 (0.059) -0.0039 Interaction effects
(gender and education of the household head)
Female head with primary education (c.f. uneducated female head)
- - 0.090
(0.129)
0.0177 - - 0.081
(0.129)
0.0183 Female head with secondary education
(c.f. uneducated female head)
- - -0.012
(0.113)
-0.0043 - - -0.037
(0.113)
-0.0027
Female head with higher education (c.f. uneducated female head)
- - -0.143 (0.190) -0.0183 - - -0.155 (0.190) -0.0147 Constant -1.609*** (0.012) - -1.465*** (0.053) - -1.575*** (0.013) -1.456*** (0.053) - N 30,285 30,285 30,283 30,283 Pseudo R-squared 0.0019 0.0042 0.0057 0.0076 Log Pseudolikelihood -6186.7008 -6172.2076 -6162.7478 -6151.3874
a. Robust standard errors are reported in parentheses
24
6. Discussion
Overall, the results presented above show that there is an impact of fuel type on children's respiratory health in the Nigerian context. The first two models confirm that combinedly modern cooking fuels are significantly safer when it concerns children’s respiratory health compared to their conventional counterparts when considered together. However, looking at the individual level of fuel types, we notice some inconclusive results. For instance, when compared with fuelwood, among the modern alternatives, electricity seems to offer the best output with regards to ARI in children, whereas biogas shows the lowest marginal effect among all modern and conventional cooking fuels. One explanation might be the limited number of observations accounted for this fuel type. However, seeing a limited number of observations might be less surprising if we consider that the installation and maintenance of biogas plants are usually very expensive and require expertise that is often not always available in the developing and least-developed countries (Faizan & Thakur, 2019; Surendra et al., 2014). This challenge might hold for all modern fuel types and ultimately can restrict the population from switching to a cleaner source. Even if someone transits to the modern alternative, a complete switch might rarely happen as refueling cleaner fuels, for instance, LPG, electricity, might incur more costs than the traditional wood-based and biomass alternatives (Nayak et al., 2015).
On the other hand, among the conventional fuels, lignite coals seem to outperform other conventional alternatives when compared with fuelwood. Again, this might be the case due to a limited number of observations. Although all conventional fuels show a negative marginal effect compared to fuelwood, one must interpret this result with caution as this does not automatically warrant continuing with these fuel types, such as kerosene, charcoals, which are marked as lethal and highly risky fuels for human health, in particular for the children (WHO, 2018). On the discussion of why the mass population should switch from using biomass fuels in traditional cooking stoves, Openshaw (1979) argues that most traditional biomass stoves are very inefficient. When tested under controlled trial they were seen to use six or seven times more energy than non-biomass-burning stoves. Barnes et al. (1994) claim that the unaffordability of the poor population to get access to modern stoves and fuels acts as a motivation behind developing more energy-efficient and affordable stoves which can lessen the local pressure on wood resources, cut down the walking time required to collect fuel, reduce the budget for the expenditure on fuelwood or charcoal and last but not the least decrease the number of pollutants released into the environment.
25
To promote the widespread use of modern fuels, government interventions through direct engagement, offering subsidies as well as initiating different types of public-private collaboration is instrumental (Nayak et al., 2015; UNDP & WHO, 2009; Zulu, 2010). However, individual organizations are also playing key roles in different contexts. As an example, we can have a look at the achievements of an organization named Solar Sister, which centers local women to spread clean solar energy for achieving sustainable solutions to climate change and improves their lives, and eradicates poverty. With the provision of solar energy and clean cookstoves, it has reached 1.8 million people across Africa and created more than 5000 clean energy entrepreneurs (Solar Sister, n. d.). Another interesting example could be the study of Randomised Exposure Study of Pollution Indoors and Respiratory Effects (RESPIRE) that explored the provision of a modern stove, Plancha, in Guatemala. The study found that women who received planchas had experienced reduced CO2 levels and other improved health
symptoms (Diaz et al., 2007; Smith-Sivertsen et al., 2004). From a policy implication perspective, the Nigerian government can explore and encourage similar activities to tackle the harmful impacts of HAP. In line with this, Duflo et al. (2008) emphasize the need of developing, promoting, and subsidizing improved cooking stoves. They further advocate for promoting improved cooking stoves that can efficiently use traditional cooking fuels, which would be a better solution for poor households that cannot afford the cost of modern fuel like electricity, thus refrain from switching to cleaner alternatives. In a similar vein, WHO (2013) claimed that halving exposure to indoor air pollution can be achieved with the use of a chimney stove instead of an open fire.
The international community initially encouraged the use of improved stoves because of their possibility to decrease the consumption of fuel and thus reduce deforestation (Manibog, 1984). It was soon after when the health concerns associated with the use of traditional stoves and fuel and the public health benefits resulting in a reduction in carbon emission and exposure to indoor smoke came into discussion. This “double dividend” benefits public health while reducing unfavorable environmental impacts centered a great deal of effort on the designing and dissemination of improved stoves (Barnes et al., 1994; Kammen 1995; Smith et al., 1993). Globally, we see many positive impacts such as a decrease in fuelwood consumption as well as reduced exposure to HAP, thanks to the adaption of modern cooking methods and fuels (see, Gowda et al., 1995; McCracken & Smith, 1998).
Moreover, this study also shows the likelihood of finding ARI symptoms among children might be contingent on who is making the key decisions in the household and his/her educational level. In both models 2 and 4, we notice households that are led by individuals who
26
are over 50 but less than 75 years, are more likely to see a better outcome with regards to ARI among children. And the results look even more promising in cases when the leader of the household is an educated female. These findings are consistent with prior studies and imply that to guide the households in taking better decisions concerning their fuel choice, more female must be provided with higher education opportunities along with an improvement of their socioeconomic conditions (Desalu et al., 2010; Faizan & Thakur, 2019; Liu et al., 2020;
27
7. Conclusion
The purpose of this thesis was to explore whether fuel types have any impact on children’s respiratory health and whether a transition to modern cooking fuels can be a remedy. Prior studies found that Nigerian women who are reliant on conventional cooking fuels are highly exposed to HAP, thus suffer from respiratory health problems (Ana et al., 2013; Desalu et al., 2010; Oluwole et al., 2017). Based on the children's recode of Demographic and Health Survey (DHS) survey data conducted in Nigeria in 2018, this thesis extends this discussion by confirming the effects of conventional cooking fuels on children’s respiratory health. Specifically, it shows that modern cooking fuels combinedly are marginally more effective when it concerns ARI among children compared to the traditional fuels used in households. However, the effects are not conclusive when considered for individual fuel types and their marginal effects on the likelihood of ARI. Also, we notice some impact of household characteristics such as the age and gender of the key decision-maker at home, and the level of female education.
However, as in all research works, this study also faced a few limitations. The first concern, lack of longitudinal data collected from the same households. Even though DHS central database offers cross-sectional survey data for different years, there is no indication provided that these surveys were collected from the same households. As a result, it was not possible to see whether the discussed effects evolved over a period. Second, when estimating the impact of fuel type on ARI, household income could be an important factor to be taken into consideration. However, the children's recode dataset does not contain any such variable. Nevertheless, one can consider the level of education as a proxy to socioeconomic status and that was controlled in two models of this study. Third, the survey collected information on one single fuel type used in the household. It would be interesting to know whether there were households that used more than one type of fuel at a time or during the year. For instance, agricultural crop residues might be more available after harvesting season, whereas a household with access to electricity might only use it when it rains outside and makes the situation impossible to burn fuelwoods. However, the survey does not help in this regard. Fourth, considering the adverse impact of fuelwood consumption on the environment, it would be very interesting to further explore whether the transition to modern cooking fuels can also reduce the rate of deforestation. However, again, the dataset did not contain any such information. Moreover, I attempted to connect this DHS dataset with additional deforestation data, but in vain, as the datasets could not be matched with each other, simply because either they consider
28
individual vs aggregated level or, do not consider the same households so to speak the impact could not be explored.
However, the good news is, this is perhaps the most updated dataset with the highest number of observations available on the given topic for the chosen context. Also, all the limitations mentioned above can be addressed in future studies, if the researchers can engage with the context and collect data over a period from the same households including the impact on the environment. Additionally, future research might also consider collecting information on regional levels so that they could later investigate whether the impact of fuel types varies among different regions, and if yes, why so and what should be done to improve such conditions. With regard to policy implications, this study suggests investing more resources in designing holistic approaches to address, motivate and retain people to transit to more modern fuel types that offer better outcomes to both physical and environmental wellbeing. From a policy perspective, considering the expensive costs of switching to modern fuel alternatives, policymakers might drive for some public-private collaboration to scale up the development process. At the same time, this thesis also provides a hint that empowering and educating women can positively contribute to fuel choice at the household level and reduce the likelihood of ARI in children.
29
8. Reference
Alam, S. A., & Starr, M. (2009). Deforestation and greenhouse gas emissions associated with fuelwood consumption of the brick making industry in Sudan. Science of The Total
Environment, 407(2), 847-852.
Alem, Y., Hassen, S., & Köhlin, G. (2013). The dynamics of electric cookstove adoption: panel data evidence from Ethiopia. Working Papers in Economics, Department of Economics,
University of Gothenburg.
https://gupea.ub.gu.se/bitstream/2077/32452/1/gupea_2077_32452_1.pdf
Alem, Y., & Ruhinduka, R. D. (2020). Saving Africa's tropical forests through energy
transition: A randomized controlled trial in Tanzania (No. 885). Ruhr Economic Papers.
https://www.econstor.eu/bitstream/10419/227108/1/1742253237.pdf
Ana, G., Adeniji, B., Ige, O., Oluwole, O., & Olopade, C. (2013). Exposure to emissions from firewood cooking stove and the pulmonary health of women in Olorunda community, Ibadan, Nigeria. Air Quality, Atmosphere & Health, 6(2), 465-471.
Ayuba, H. K., & Dami, A. (2005). Environmental science: An introductory text. Apani Pub
Kaduna.
Bailis, R., Drigo, R., Ghilardi, A., & Masera, O. (2015). The carbon footprint of traditional woodfuels. Nature Climate Change, 5(3), 266-272.
Barber, C. V., Johnson, N., & Hafild, E. (1994). Breaking the Logjam. Washington, DC: World Resources Institute.
Barnes, D. F., Openshaw, K., Smith, K. R., & Van der Plas, R. (1994). What makes people cook with improved biomass stoves. World Bank Technical Paper, 242, 2004.
Barnes, D. F., Krutilla, K., & Hyde, W. F. (2010). The urban household energy transition:
social and environmental impacts in the developing world. Routledge.
Bizzarri, M., Bellamy, C., Bizzarri, R. M., Katajisto, M., & Patrick, R. E. (2010). Safe access to firewood and alternative energy in Kenya: an appraisal report. New York: Women’s
Commission for Refugee Women and Children.
Boahene, K. (1998). The challenge of deforestation in tropical Africa: reflections on its principal causes, consequences and solutions. Land Degradation & Development, 9(3), 247-258.
Colfer, C. J. P., Dudley, R. G., & Gardner, R. (2008). Forest women, health and childbearing. Human Health and Forests: A Global Overview of Issues, Practice and Policy, 113-133.
Cooke, P., Köhlin, G., & Hyde, W. F. (2008). Fuelwood, forests and community management– evidence from household studies. Environment and Development Economics, 103-135.
30
Croitoru, L., Chang, J. C., & Kelly, A. (2020). The cost of air pollution in Lagos.
https://openknowledge.worldbank.org/bitstream/handle/10986/33038/The-Cost-of-Air-Pollution-in-Lagos.pdf?sequence=5&isAllowed=y
Das, K., Pradhan, G., & Nonhebel, S. (2019). Human energy and time spent by women using cooking energy systems: A case study of Nepal. Energy, 182, 493-501.
Dasgupta, S., Huq, M., Khaliquzzaman, M., Pandey, K., & Wheeler, D. (2006). Who suffers from indoor air pollution? Evidence from Bangladesh. Health Policy and Planning, 21(6), 444-458.
Demographic and Health Survey (n.d.). DHS-VII Recode Manual.
https://dhsprogram.com/pubs/pdf/DHSG4/Recode7_DHS_10Sep2018_DHSG4.pdf
Desalu, O. O., Adekoya, A. O., & Ampitan, B. A. (2010). Increased risk of respiratory symptoms and chronic bronchitis in women using biomass fuels in Nigeria. Jornal Brasileiro
de Pneumologia, 36(4), 441-446.
Diaz, E., Smith-Sivertsen, T., Pope, D., Lie, R. T., Diaz, A., McCracken, J., ... & Bruce, N. (2007). Eye discomfort, headache and back pain among Mayan Guatemalan women taking part in a randomised stove intervention trial. Journal of Epidemiology & Community Health, 61(1), 74-79.
Ding, W., Wang, L., Chen, B., Xu, L., & Li, H. (2014). Impacts of renewable energy on gender in rural communities of north-west China. Renewable Energy, 69, 180-189.
Duflo, E., Greenstone, M., & Hanna, R. (2008). Indoor air pollution, health and economic well-being. SAPI EN. S. Surveys and Perspectives Integrating Environment and Society, (1.1). Eckholm, E. (1975). The other energy crisis: firewood. Worldwatch Paper, (1).
Ellis, J. (1991). Antarctica and global climatic change: review of prominent issues in Antarctica and the global change'in C. Antarctica and Global Climatic Change, Belhaven, London.
Faizan, M. A., & Thakur, R. (2019). Association between solid cooking fuels and respiratory disease across socio-demographic groups in India. Journal of Health & Pollution, 9(23).
Fullerton, D. G., Semple, S., Kalambo, F., Suseno, A., Malamba, R., Henderson, G., ... & Gordon, S. B. (2009). Biomass fuel use and indoor air pollution in homes in Malawi. Occupational and Environmental Medicine, 66(11), 777-783.
Ghana National Communication to the UNFCCC (Ghana NatComm). (2000). Ghana National
Communication to the United Nations Framework Convention on Climate Change Conference of the Parties. http:// unfccc.int/resource/docs/natc/ghanc1.pdf
Gough, J. (2019). Toxic air is harming our children with every breath that they take. https://www.unicef.org/rosa/stories/toxic-air-harming-our-children-every-breath-they-take Gowda, M. C., Raghavan, G. S. V., Ranganna, B., & Barrington, S. (1995). Rural waste management in a south Indian village—a case study. Bioresource Technology, 53(2), 157-164.
31
Izumi, T., Higano, Y., Matsubara, E., Dung, D. T., Minh, L. T., & Chiem, N. H. (2015). Effect of appropriate technology introduction to farm households in vietnam for GHG emission reduction. Journal of Sustainable Development, 8(8), 147.
Jagger, P., & Shively, G. (2014). Land use change, fuel use and respiratory health in Uganda. Energy Policy, 67, 713-726.
Kammen, D. M. (1995). From energy efficiency to social utility: improved cookstoves and the Small Is Beautiful model of development. Energy as an Instrument for Social Change
(Goldemberg J, Johansson TB, eds). New York: United Nations Development Programme,
50-62.
Khalequzzaman, M., Kamijima, M., Sakai, K., Chowdhury, N. A., Hamajima, N., & Nakajima, T. (2007). Indoor air pollution and its impact on children under five years old in Bangladesh. Indoor Air, 17(4), 297-304.
Köhlin, G., Parks, P. J., Barbier, E. B., & Burgess, J. C. (2001). Spatial variability and disincentives to harvest: deforestation and fuelwood collection in South Asia. Land
Economics, 77(2), 206-218.
Levison, D., DeGraff, D. S., & Dungumaro, E. W. (2018). Implications of environmental chores for schooling: Children’s time fetching water and firewood in Tanzania. The European
Journal of Development Research, 30(2), 217-234.
Liu, Z., Li, J., Rommel, J., & Feng, S. (2020). Health impacts of cooking fuel choice in rural China. Energy Economics, 89, 104811.
Mallo, I. I. Y., & Ochai, B. C. (2009). An Assessment of the Effects of Urbanization on Deforestation in Bwari Council, Abuja–FCT, Nigeria. Abuja Journal of Geography and
Development, 3(1), 1-19.
Manibog, F. R. (1984). Improved cooking stoves in developing countries: problems and opportunities. Annual Review of Energy, 9(1), 199-227.
McCracken, J. P., & Smith, K. R. (1998). Emissions and efficiency of improved woodburning cookstoves in Highland Guatemala. Environment International, 24(7), 739-747.
Millennium Ecosystem Assessment. (2005). Ecosystems and Human Well-Being (Vol. 5, P. 563). Washington, DC: Island Press.
MEPD (Ministry of Environment & Physical Development) and HCENR (Higher Council for Environment and Natural Resources). (2003). Sudan's first national communications under the
United Nations Framework Convention on Climate Change. Volume 1: Main communications.
https://unfccc.int/resource/docs/natc/sudnc1.pdf
Mondal, M. A. H., Bryan, E., Ringler, C., Mekonnen, D., & Rosegrant, M. (2018). Ethiopian energy status and demand scenarios: prospects to improve energy efficiency and mitigate GHG emissions. Energy, 149, 161-172.
32
Myers, N. (1994). Tropical Deforestation: Rates and Pattern. The Causes of Tropical
Deforestation, 27-40.
Naeher, L. P., Brauer, M., Lipsett, M., Zelikoff, J. T., Simpson, C. D., Koenig, J. Q., & Smith, K. R. (2007). Woodsmoke health effects: a review. Inhalation Toxicology, 19(1), 67-106.
Nayak, B. P., Werthmann, C., & Aggarwal, V. (2015). Trust and cooperation among urban poor for transition to cleaner and modern cooking fuel. Environmental Innovation and Societal
Transitions, 14, 116-127.
Ndiritu, S. W., & Nyangena, W. (2011). Environmental goods collection and children’s schooling: Evidence from Kenya. Regional Environmental Change, 11(3), 531-542.
Obaseki, D. O., Awopeju, O. F., Awokola, B. I., Adeniyi, B. O., Adefuye, B. O., Ozoh, O. B., ... & Erhabor, G. E. (2017). Domestic solid fuel combustion in an adult population in Nigeria: A cross sectional analysis of association with respiratory symptoms, quality of life and lung function. Respiratory Medicine, 130, 61-68.
Oguntoke, O., Opeolu, B. O., & Babatunde, N. (2010). Indoor air pollution and health risks among rural dwellers in Odeda area, South-Western Nigeria. Ethiopian Journal of
Environmental Studies and Management, 3(2).
Oguntoke, O., Adebulehin, A. T., & Annegarn, H. J. (2013). Biomass energy utilisation, air quality and the health of rural women and children in Ido LGA, south-western Nigeria. Indoor
and Built Environment, 22(3), 528-534.
Okia, C. A. (Ed.). (2012). Global Perspectives on Sustainable Forest Management. BoD– Books on Demand.
Oluwole, O., Ana, G. R., Arinola, G. O., Wiskel, T., Falusi, A. G., Huo, D., ... & Olopade, C. O. (2013). Effect of stove intervention on household air pollution and the respiratory health of women and children in rural Nigeria. Air Quality, Atmosphere & Health, 6(3), 553-561.
Oluwole, O., Arinola, G. O., Huo, D., & Olopade, C. O. (2017). Household biomass fuel use, asthma symptoms severity, and asthma underdiagnosis in rural schoolchildren in Nigeria: a cross-sectional observational study. BMC Pulmonary Medicine, 17(1), 1-8.
Openshaw, K. (1979). A comparison of metal and clay charcoal cooking stoves. In Conference
on Energy and Environment in East Africa, Nairobi (Kenya), May 1979 (No. 18892).
Rehfuess, E. (2006). Fuel for life: household energy and health. World Health Organization. https://www.who.int/airpollution/publications/fuelforlife.pdf?ua=1
Repetto, R. (1990). Deforestation in the tropics. Scientific American, 262(4), 36-45.
Revkin, A. C. (1988). Endless summer: living with the greenhouse effect. Discover, 9(10), 50-61.
33
Rinne, S. T., Rodas, E. J., Rinne, M. L., Simpson, J. M., & Glickman, L. T. (2007). Use of biomass fuel is associated with infant mortality and child health in trend analysis. The
American Journal of Tropical Medicine and Hygiene, 76(3), 585-591.
Royer, J. F., & Mahouf, J. F. (1992). Consequences of an increase in the greenhouse effect'. The
Courier, 133, 18-21.
Sapkota, A., Gajalakshmi, V., Jetly, D. H., Roychowdhury, S., Dikshit, R. P., Brennan, P., ... & Boffetta, P. (2008). Indoor air pollution from solid fuels and risk of hypopharyngeal/laryngeal and lung cancers: a multicentric case–control study from India. International Journal of Epidemiology, 37(2), 321-328.
Silver, C. S., & DeFries, R. S. (1990). One Earth: Our Changing Global Environment; One
Future. National Academy Press.
Smith, K. R. (2006). Health impacts of household fuelwood use in developing countries. UNASYLVA-FAO-, 57(2), 41.
Smith, K. R., Mehta, S., & Maeusezahl-Feuz, M. (2004). Indoor smoke from household solid fuels. In M. Ezzati, A. D. Lopez, A. Rodgers, & C. J.L. Murray (Eds.), Comparative
quantification of health risks: Global and regional burden of disease due to selected major risk factors (Volume 1, pp. 1435-1493). World Health Organization.
Smith, K. R., Shuhua, G., Kun, H., & Daxiong, Q. (1993). One hundred million improved cookstoves in China: how was it done?. World Development, 21(6), 941-961.
Smith-Sivertsen, T., Díaz, E., Bruce, N., Díaz, A., Khalakdina, A., Schei, M. A., ... & Smith, K. R. (2004). Reducing indoor air pollution with a randomised intervention design–. Norsk
Epidemiologi, 14(2), 137-143.
Solar Sister. (n.d.). What we do: our impact. https://solarsister.org/what-we-do/our-impact/
Surendra, K. C., Takara, D., Hashimoto, A. G., & Khanal, S. K. (2014). Biogas as a sustainable energy source for developing countries: Opportunities and challenges. Renewable and
Sustainable Energy Reviews, 31, 846-859.
Thacher, J. D., Emmelin, A., Madaki, A. J., & Thacher, T. D. (2013). Biomass fuel use and the risk of asthma in Nigerian children. Respiratory Medicine, 107(12), 1845-1851.
Torres-Duque, C., Maldonado, D., Pérez-Padilla, R., Ezzati, M., & Viegi, G. (2008). Biomass fuels and respiratory diseases: a review of the evidence. Proceedings of the American Thoracic
Society, 5(5), 577-590.
UNDP., & WHO. (2009). The energy access situation in developing countries: A Review
Focusing on the Least Developed Countries and Sub-Saharan Africa.
https://www.undp.org/content/dam/undp/library/Environment%20and%20Energy/Sustainable %20Energy/energy-access-situation-in-developing-countries.pdf
United Nations. (2015). Transforming our world: the 2030 Agenda for Sustainable