Examensarbete i omvårdnad Malmö universitet
61-90hp Hälsa samhälle
Sjuksköterskeprogrammet 205 06 Malmö
EXPLORING COMMUNICATION AND
INFORMATION IN RURAL AREAS FOR
NURSES IN MAPUTO, MOZAMBIQUE
TINA LEANDERSSON
JOSEFINE TEDENLIND
The authors would like to say a special thank you to Dr Vaz, Dr Tchamo and Mrs Bomba for all the assistance in implementing this bachelor thesis. Additional, a thank you to our
supervisor at Malmo University, PhD Elisabeth Mangrio.
EXPLORING COMMUNICATION AND
INFORMATION IN RURAL AREAS FOR
NURSES IN MAPUTO, MOZAMBIQUE
TINA LEANDERSSON
JOSEFINE TEDENLIND
Leandersson, T and Tedenlind, J. Exploring communication and information in rural areas for nurses in Maputo, Mozambique. Degree project in Nursing 15 credit points. Malmö
University: Faculty Health and Society, Department of Care Science, 2018.
Aim: The aim of this MFS study is to illuminate how nurses describe the communication and information strategies used in order to promote young women's reproductive health in rural settings, Maputo province. Background: To be able to provide good healthcare to women in rural areas it is crucial for the nurses to reach out with communication and information. Mozambique has one of the highest maternal mortality rates in Africa. The high number of deaths is partly due to a lack of self-determination among women, a long distance to reach health care centers and lack of economic support for transportation and medical costs. This is intensified by poverty, young age, inequality, and less economic rights of making own
decisions. Method: Semi-structured interviews were conducted on a sample of seven nurses at four different hospitals in Maputo province. The collected data was transcribed, coded and analyzed by a qualitative content analysis. Results: From the data, two main categories emerged, which focus on specific tools to give information to reach out in rural areas and the challenges that the nurses face regarding information and communication. It was shown in the result that the nurses had to provide individualized information in mother tongue and provide more aid in communication, which in turn would ease the nurse’s
work. Conclusion: Different strategies and tools were identified among the nurses to promote young women's reproductive health. The nurses pointed out the importance of providing information in mother tongue to reach out in rural areas.
EN UNDERSÖKNING
OM KOMMUNIKATION OCH
INFORMATION BLAND
SJUKSKÖTERSKOR PÅ
LANDSBYGDEN I MAPUTO,
MOZAMBIQUE
TINA LEANDERSSON
JOSEFINE TEDENLIND
Leandersson, T och Tedenlind, J. En undersökning om kommunikation och
information bland sjuksköterskor på landsbygden i Maputo, Mozambique. Examensarbete i omvårdnad 15 högskolepoäng. Malmö Universitet: Fakulteten för Hälsa och samhälle, Institutionen för vårdvetenskap, 2018.
Syfte: Syftet med studien var att belysa hur sjuksköterskor beskriver de kommunikations- och informationsstrategier som används för att främja unga kvinnors reproduktiva hälsa på
landsbygden i Maputo provins. Bakgrund: För att kunna erbjuda god hälso- och sjukvård till kvinnor på landsbygden är det av stor vikt att kunna nå ut genom kommunikation och information. Mozambique är ett av de länder i Afrika med störst mödradödlighet. Den höga siffran av dödsfall grundar sig delvis i bristen på självbestämmande hos kvinnor, avstånd till sjukhus och bristen på ekonomiskt stöd för transport samt medicinska kostnader. Det förstärks av fattigdom, ung ålder, ojämlikhet samt avsaknad av ekonomiska rättigheter till att fatta egna beslut. Metod: Semistrukturerade intervjuer genomfördes med sju olika sjuksköterskor på fyra olika sjukhus i Maputo provinsen. Den insamlade data blev transkriberad, kodad och sedan analyserad. Kvalitativ innehållsanalys tillämpades. Resultat: Två huvudkategorier framkom från den insamlade data. Den första huvudkategorin berörde vilka verktyg sjuksköterskorna använde sig av för att nå ut på landsbygden med information och kommunikation och den andra huvudkategorin som uppkom handlade om utmaningarna som sjuksköterskorna i studien ställdes inför angående kommunikation och information. De två kategorierna hade tre underkategorier vardera. I resultatet påvisades att sjuksköterskorna var tvungna att
tillhandahålla information på modersmål och använda sig av anpassade
kommunikationsverktyg, vilket i sin tur skulle underlätta sjuksköterskans arbete. Konklusion: Olika strategier och verktyg identifierades av sjuksköterskorna i syfte att främja unga kvinnors reproduktiva hälsa. Sjuksköterskorna påpekade vikten av att ge information på patientens modersmål, för att nå ut till alla på landsbygden. Nyckelord:, Information, Kommunikation, Kvinnohälsa, Omvårdnad, Prevention.
TABLE OF CONTENT
INTRODUCTION 6
BACKGROUND 6
Maternal health 6
Focus Fistula Organization 7
Cultural competence 7
Communication is the key 8
AREA OF CONCERN 9 AIM 9 METHOD 9 Pilot 9 Sample 10 Data collection 10 Data analysis 10 ETHICAL CONSIDERATIONS 11 RESULTS 12 To face challenges 12 Language issues 12 Cultural issues 13
Nurses wish of improvement 14
Tools for giving information to reach out in rural areas 15
Preventive work 16 Education 16 Community work 17 DISCUSSION 18 Method discussion 18 Data collection 18 Sample 19 Data analysis 19 Discussion of result 20 CONCLUSION 22
FURTHER RESEARCH AND VALUE FOR THE STUDY 22
REFERENCES 24
APPENDIX 1 27
INTRODUCTION
Through internet connection and social media, we can be contacted, share our facts and ideas with a simple click on a smartphone or using a computer. This is something most of us take for granted in Sweden. In developing countries, in this case Mozambique, internet technology is mainly more common for those who live in the cities but in rural areas it is still far from available for everyone. This Minor field study focus on describing the nurse's strategies in how communication and information is carried out in rural settings in order to promote young women's reproductive health in rural settings. Studying nursing, we have been taught, since day one, the importance of preventive care, communication with the patients and equal care. Majority of the people in Mozambique live far away from hospitals which involves several different risks. With that in mind, we felt that there was an important need to
investigate and illuminate what methods health professionals used to reach out in rural areas and how to improve the communication and information that was given to women to
promote their reproductive health.
BACKGROUND
Mozambique is a country located in Southeast Africa and is bordered by the Indian Ocean to the east, with a population of about 30,5 million people (World population review 2018). The capital city is Maputo. Mozambique became independent from Portugal in 1975 after several hundred years of colonization. Two years after the independency the country suffered from a civil war that ended 1992 and left it in shambles (UNICEF 2014). The country’s economy is today stabilized due to the agriculture that contributes 80 percent of Mozambique’s labor force (USAID 2017). This economic expansion has unfortunately not improved or reduced the poverty, which has almost remained unchanged (World Bank 2017).
Health today in Mozambique is determined by where people are born, their economic status, gender, and age (Firoz et al. 2016). The health care system is financed through funds from the state budget and from external funds but because of extensive poverty, not many people can afford to pay medical assistance (WHO 2015). The availability of hospital beds has a density of 0,7 beds/1000 population (World Factbook 2011).
The Nation is strongly male dominated which leads to women's lack of self-determination (Cook et al. 2004). As an additional consequence of male dominance, young women are often forced to marry before the age of 18. Statistic from Mozambique shows that the rate of child marriage reaches a 48 percentage (UNICEF 2016). In light of women’s health, UNICEF have pointed out that:
“Girls who marry before they turn 18 are less likely to remain in school and more likely to experience domestic violence. Young teenage girls are more likely to die due to complications in pregnancy and childbirth than women in their 20s; their infants are more likely to be stillborn or die in the first month of life” (UNICEF 2016).
Maternal health
Mozambique has one of the highest maternal mortality rates in Africa with a ratio of 480 per 100,000 live births (Firoz et al. 2016). This high number of deaths is partly due to the lack of
economic support for transportation and medical costs, a lack of self-determination
among women and a long distance to reach healthcare centers. This is intensified by poverty, young age, inequality, and less economic rights of making own decision (ibid).
Many Mozambican women often delay their consultation with a midwife which in turn may lead to serious health complications (Munguambe et al. 2016). These delayed decisions to seek prenatal care are influenced by factors such as fear of medical procedures, complexities of decision making in the household, social, economic and structural factors. Women often wait to seek prenatal care until pregnancy shows or until the baby starts to move. Some women delay seeking prenatal care and choose more traditional treatments common to their culture, such as visiting a healer, instead of a midwife (ibid).
Delayed decision making, lack of transportation, poverty and lack of skilled attendance at birth can lead to obstetric fistula (Cook et al. 2004). An abnormal hole/fistula is created in the tissue wall between the vagina and bladder and/or rectum, which leads to incontinence of urine and/or feces. It is often due to women who give birth before their pelvis is fully grown, premature childbearing and/or malnutrition. The occurrence of fistulas is because to the baby's head is pressing on blood vessels and thereafter cuts off the blood flow to the soft tissue around it. It leads to necrosis of the tissue by the lack of oxygen and consequently, the appearance of fistulas. Obstetric fistula is a largely hidden problem that affects young women who give birth at home under poor and bad conditions (ibid).
Focus Fistula Organization
The Focus Fistula Organization (2016) is a non-profit organization founded in 2016, focused on offering care and treatment by repairing women with obstetric fistula. The organization's aim is to end the fistula occurrence in Mozambique. By raising public awareness, provide safe surgeries and educate nurses to early discover fistula patients in pre- and postnatal care, the prevalence will reduce. Another preventive focus is their outreach work provided by the nurses at the organization. The organization has invited the authors to help them to identify and describe which outreach methods are used and how communication and information can be improved to decrease the occurrence of obstetric fistula.
Cultural competence
Jirwe et al. (2014) describes cultural competence as an ability that involves understanding people’s different culture backgrounds such as gender, socio-economic background, life experiences and other beliefs. The ambition of cultural competence is to care for everyone and provide equal and individualized healthcare. To understand the differences between people, it is necessary to have knowledge about culture diversities. Cultural competence is a dynamic and complex developing process that is an ongoing and continuous expanding of one's cultural knowledge. It will develop over time and will begin with identifying one's own cultural values and traditions. This will continue through interactions with other people from different cultures and extend through a lifelong learning. Therefore, to be able to recognize and respect other people’s cultural backgrounds, nurses need to identify their own and understand how these have shaped them as a person. Nurses who are culturally competent have the ability to identify their own stereotypes and by knowing these cultural differences minimize the risks of hurting others with different cultural background. With a cultural competence, nurses mediate understanding and respect to the patients and is most likely to get the same in return. Such a relationship between the nurse and the patient creates good
conditions for quicker recovery (ibid). This shows that it
the most important is to see the patient as an individual person and not only a part of a culture (Wiklund Gustin & Lindwall 2012).
Communication is the key
Communication is defined as an exchange of thoughts and ideas between people, to achieve an understanding (Kourkouta & Papathanasiou 2014). It consists of physical space, cultural and social values and psychological conditions (ibid). It is an essential component in the nursing profession, where communication is the key to provide good healthcare and safe practice (Hartung & Miller 2018). To be able to improve the skill of communication, there is a need to describe what the concept of communication is and making sure there is an ongoing evaluation of the process among the staff (ibid). To achieve a good result in healthcare, communication is significant in all nurse’s assignments, such as prevention, therapy,
education and health promotion (Kourkouta & Papathanasiou 2014). The language should be individualized and understandable for all involved to improve the healing process. It is confirmed that patients that seeks help at healthcare clinics and hospitals comes in to the dialogue with emotional and physical stress due to the situation that he/she is facing. The dialogue between the nurse and the patient involves a lot of various feelings and should therefore be handed with frankness and honesty to not create any doubts or misunderstandings (ibid).
Communication is a complex and important nursing treatment where the patient need to be involved for a faster and better healing process (Swedish Society of Nursing 2011). By letting the patient be involved in the communication and healthcare provides a so
called holistic perspective. A holistic nursing approach refers to a kind of nursing practice which focuses on treating the patient as a whole as opposed merely treating the symptoms of their present condition. Holistic perspective is characterized by openness to the patients’ needs and as far as possible, to involve the patient in the communication and decision-making regarding his/her own health care (ibid).
The Swedish Society of Nursing (2017) has identified that one of the most common reasons to health-related adverse events, is failure in the transmission of communication. Everyone involved in the communication have different ways of seeing and perceiving the context of the conversation because of earlier experiences in life and previous references. These earlier experiences have an impact on how the message is given/received and could easily be misunderstood due to the other person’s references (ibid).
The overall literacy rate is 47 percentages (USAID 2017) and 70 percentages
of Mozambiquan population are living in rural areas (World Bank 2017). Most of rural people in Mozambique do not speak the official language (Portuguese) nor English, which makes it crucial to reach out in these areas by providing radio in their mother tongue (Macueve et al. 2009). According to Macueve et al. (2009), the radio is still the most affordable and effective communicative method to reach out in rural areas of Mozambique. Radio broadcast is not depending on access to electricity and is free of charge to the listener which makes it a cheap and practically way of spreading and receiving communication and information (ibid).
AREA OF CONCERN
Based on the information from Focus Fistula together with the knowledge of that Mozambique has one of the highest maternal mortality rates in Africa, there is a need to investigate what methods and strategies regarding communication and information the nurses use to promote young women's reproductive health. Many women in Mozambique do not have the possibility to make their own decisions, due to the strong inequality that exists in the country (Munguambe et al. 2016). As a consequence of not having the power of
self-determination, Mozambican women in rural areas often delay their consultation and by that time, complications may already have occurred (ibid). The poor access and long distance to health care in rural areas makes it difficult for women to receive information. This shows the importance of further research of how the nurses in rural areas work to prevent unwanted obstetric issues.
AIM
The aim of this MFS study is to illuminate how nurses describe the communication and information strategies used in order to promote young women's reproductive health in rural settings, Maputo province.
METHOD
An empirical study was conducted with a qualitative approach as described by Polit & Beck (2014). Interviews were held, to gain a deeper understanding of how nurses conduct outreach work and what kind of information that is given in order to prevent obstetric complications before and after childbirth. By using a qualitative approach, data is based on human’s experiences and observations, which in turn, is suitable to receive a holistic perspective of what is being studied (Polit & Beck 2014). Data was collected through a semi-structured interview guide with open-ended questions. This allowed the informants to talk freely and letting new ideas to be brought up during the interview and the interviewer could steer back to the sets of questions when needed. By using this technique, the authors gained a deeper understanding of how the world is perceived by the informants. This increased the value of the informants’ answers and the comprehension of what was being studied (Kvale 2014). The interview guide is shown in appendix 1.
Pilot
To test the feasibility of the interview guide a pilot interview were conducted as suggested by Polit & Beck (2014). To reassure that the interview questions, along with the functioning of the recording equipment worked, a pilot interview was held with a medicine student from Belgium doing the internship in Mozambique. The information provided by the medicine student were helpful and gave the researchers an insight of how communication and information was conducted in Maputo hospital. The pilot interview was not used for any further analysis, because the informant did not achieve the inclusion criteria.
Sample
Before the departure to Maputo, the authors came to know about that there were no nurses currently working for the Focus Fistula Organization. This required reevaluation of which nurses that could be appropriate to answer the aim. After consulting with the supervisor in Maputo, the solution was to use nurses in rural areas, who were working daily with spreading information and giving communication. The four hospitals where the interviews were held, were selected in an agreement with the director at Direcção Provincial de Saúde, department of Health, where a credential was received to be able start the study. The
inclusion criteria’s were that the nurses had conducted outreach work and spoke English or Portuguese. The sample included a total of seven nurses between the ages of 26-58, working at the maternity ward. They all spoke Portuguese and had experiences with outreach work in the rural areas of Mozambique.
Data collection
Data was collected during the days 5-10th of April 2018. The interviews were held in four different rural hospitals, within the area of Maputo province. At each opening meeting at the hospitals, the head-nurses were given information about the study and the inclusion criteria’s. In turn, a selection of suitable nurses, who showed interest in participating, was distributed among the staff. The interviews were held at the hospital, at a place where the nurses felt comfortable and without getting disturbed by others. The duration of the interviews varied from 27 minutes to 60 minutes and the total recorded time was 240 Minutes. During the interviews, both authors were attendant, though one was in charge of leading the interview while the other author took notes and provided supplementary questions. Taking turns on leading the interview and taking field notes were made.
In order to conduct the interviews an interpreter was hired. This person was chosen in consultation with the supervisor in Maputo. For the purpose of the study, it was of most important that the interpreter was a woman due to the hierarchy situation and considering to the area of questions that the interviews regarded. This is further described by LeBaron et al. (2015) that the interviews must be authentic to gain trustworthy and meaningful data. The interpreter shall be culturally acceptable considering social status and gender equality (ibid).
Data analysis
For analyzing the collected data, a thematic content analysis as described by Burnard et al. (2008) was performed. The thematic content analysis involves identifying themes and categories that emerge from the collected data by going through the transcripts to verify and confirm themes that repeatedly is brought up. This method is appropriate
for analyzing qualitative, semi-structured interviews with open-ended questions (ibid). Once the interviews had been transcribed verbatim, they were heard and read through once again to check each other’s transcriptions. Next step was to identify meaningful sentences and data that was relevant and linked back to the aim of the study. These quotes and phrases were highlighted and numbered to easily to go back to the specific transcript if needed. A new, clean document to paste all the meaningful and highlighted phrases was created, which is described as initial coding (ibid).
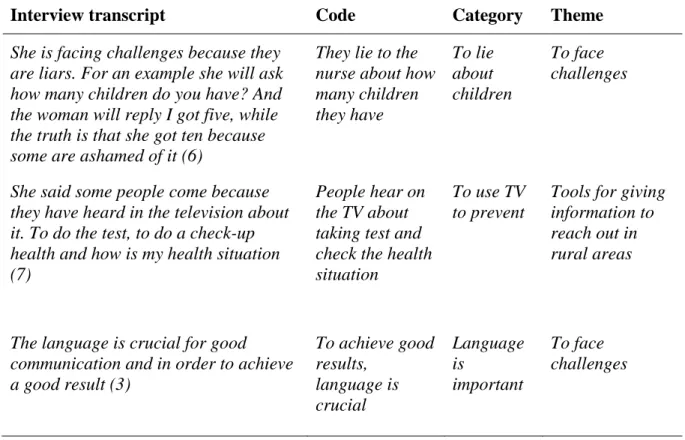
The codes were re-highlighted into different colors and matching categories and then formed in total six so called sub-categories. Throughout the process of coding, the sub-categories were divided into two overall main categories that emerged from the data. In order to show how he analysis procedure has been conducted, an example with the final set of themes, categories and codes are shown in table 1.
Table 1. Selected examples to illustrate the analysis process
Interview transcript Code Category Theme
She is facing challenges because they are liars. For an example she will ask how many children do you have? And the woman will reply I got five, while the truth is that she got ten because some are ashamed of it (6)
They lie to the nurse about how many children they have To lie about children To face challenges
She said some people come because they have heard in the television about it. To do the test, to do a check-up health and how is my health situation (7)
People hear on the TV about taking test and check the health situation
To use TV to prevent
Tools for giving information to reach out in rural areas
The language is crucial for good communication and in order to achieve a good result (3) To achieve good results, language is crucial Language is important To face challenges
ETHICAL CONSIDERATIONS
Before the study could begin an ethical application had to be submitted and accepted by the Ethical Council at The Faculty of Health and Society, at Malmo University. In December the 15th, 2017 ethical approval was given. Application number HS 2017, number 72. The study was also approved by the contact person in field, who worked as the director at the Focus Fistula organization.
In The Swedish Research Councils (2002) guideline, the research ethical principles are described. Central consideration of how to obtain confidentiality throughout the study was taken and the participants in the study was informed about the investigation by
the authors. Information was given verbally and written to the participants before the
investigation started. The participants gave their written approval to take part of the study and they were informed of their right to drop-out at any point of time. A clarification on that participation was voluntary was made and all the collected data was confidential. The
informed consent letter is shown in Appendix 2. All the information about the participants got a number instead of their name. Only the students knew what number the participants had. The gathered data was stored on separate encrypted USB and the internet access was switched off during the interviews and process of transcribing. The USB stick was secured and locked in a safe to protect against misuse or thievery. The computers that was used for the cause was secured with password protection.
RESULTS
Two overall main categories were identified from the outcome of the collected data. In order to get a greater comprehension, the data has been categorized to achieve a better
understanding of the result. During the conduction of the interviews, it became clear that some topics was mentioned repetitively, which later developed into the subcategories. Throughout the procedure of analyzing, two main categories emerged, which were To face challenges and Tools for giving information to reach out in rural areas. Each main category got three subcategories that sums up the themes, which is shown in table 2.
The following quotes in the result are sometimes presented in third-person voice due to interpreter's participation and translation.
Table 2. Data Categories and Sub-Categories
Category Subcategory
To face challenges - Language issues
- Cultural issues
- Nurses wish of improvement Tools for giving information
to reach out - Preventive work
in rural areas - Education
- Community work
To face challenges
During the conversations with the seven nurses, they confirmed some of these challenges while meeting their patients. The theme To face challenges is meant to summarize the interviewed nurses experiences of their daily work challenges at the hospitals.
Language issues
Several nurses emphasized that language barriers were an everyday challenge that took a lot of time and effort at their work. The language barrier created a challenge in ensuring that the patients truly had understood the importance of what had been said. In rural areas of
Mozambique, a lot of people did not speak or knew Portuguese but spoke only native languages. As a consequence of the language challenges, the nurses described several other techniques to reassure that their message was understood. Actions such as facial expressions, gestures, body language and follow-up questions were used to ensure the nurse and help the patients understand.
“At the end of the session, she will go back to them and say “do you understand? Tell me what you have understood”. And this is how she evaluate that the patient has understood what she said” (Nurse 5)
The available material that the nurses used at the hospitals was all in Portuguese which in turn created a gap between the nurses and the patients. To overcome this, the nurses translated the Portuguese material verbally into local mother tongue that sometimes was described as time
consuming and tiring. When the nurses felt that they struggled or did not know the patient’s local language, usually they could ask a colleague for help when confronting this kind of issues, to step in and help with translating.
“They have all of the information in Portuguese, but what they do is to accommodate and translate it into the mother tongue language. If they don't know they get assistance from colleagues to translate to mother tongue” (Nurse 3)
In Mozambique the national language is Portuguese, but the majority of the population also spoke one local language, especially in rural areas. All of the nurses in the study spoke Portuguese and spoke at least one local language. Some nurses mentioned, that one reason of language difficulties at the hospitals was because the country was boarded by six other
countries. This made it tough for the nurses to reach all the women in Maputo province due to the language influences from the other adjoining countries. As a result, the
dialogue suffered and the nurses struggled with language misunderstandings.
“For an example, my child is born here, and then after 10 years-15 years, she studies on the other side. She got half her life the other side, then she comes back. She comes back not speaking shangaan at all, not speaking Portuguese at all and then the communication is tough” (Nurse 3)
Cultural issues
All nurses clearly expressed daily obstacles that originated from culture and traditional aspects. In rural areas of Maputo province, it was very common with polygamy and early marriage before the age of 18 years. The majority of the nurses said that the girls that married before 18, dropped out of school and quickly became pregnant, which ended their chances of finishing primary and/or upper secondary school. Consequently, by not
finishing the school led to great reading and writing difficulties.
“Once you get pregnant it means automatically you are going to stay with that man. And they’re too young, from thirteen, so they break the school, closing opportunities in the life. At the time the husbands are too old for them” (Nurse 6)
When marriage at early age occurred, one nurse explained that the young women found it difficult understanding how certain physical conditions could arise, such as fistulas. The nurse was laughed at and faced a lot of skepticism when she tried to explain a certain physical condition that was connected with the patient. This was described as a consequence of early marriage and not completed school education. Therefore, the women could sometimes not understand how the complication could exist or how it was connected with their body and situation.
“It is difficult to understand something you have never seen before. And sometimes even when they are explaining about the prevention, about them to take care, they laugh because
they can not understand for example how the feces can come out of the vagina as a complication” (Nurse 1)
One nurse expressed that it is so deeply rooted in the Mozambican culture that a woman should be married and have a family. A single woman is not seen with good eyes from the society's point of view. Being single and unmarried could mean that something is wrong with you and you can become sort of an outcast. Since this it is not a desirable situation for these
women, polygamy is seen as a security option of not being left out. This is one reason that polygamy still exists, together with the financial issues that you have to battle when being single.
“It is because financial issues and socially, a single woman is not seen with good eyes in the society” (Nurse 6)
One specific nurse talked about the difficulties she faced during the consultation with the women after they had been giving birth. When the nurse introduced them to the different kinds of contraceptives that were available, the women were most often very thankful. This gave them the ability to control when they wished to be pregnant again. Unfortunately, many women stopped taking birth-control pills or did refuse to have etonogestrel contraceptive implant because of the stories they heard from fellow women in their villages. They daily challenge of trying to promote women's reproductive health was complicated due to the old sayings and ignorance.
“The women outside telling them that if you take those pills you might become infertile and then they won't accept, they avoid. Regarding that implant that we put here (points at arm), they are told that if it escapes somehow it comes to your heart you are dead” (Nurse 1)
Culture aspects such as using traditional medicine and going to witch doctors was still
something that took place in big parts of the rural areas. This was expressed by the nurses as a big contradiction of what the nurses and the healthcare conception was all about and what they stood for. When patients chose to use traditional options, huge health complications can arise and lead to non-reversible conditions and at worst case scenario, death. One nurse explained that her patients most often went to see a witch doctor at first but always came back to seek help at the hospital because the conditions that the person searched for had not
improved or changed.
“They go to witch doctors but they always come back because there are things that they can not do, that has to be completed here” (Nurse 5)
The nurses all more or less mentioned the mission of trying to get their patients to understand the importance of taking prescription medicine on the right time and day. Many people did no t own or knew how to use a watch but were instead guided by the position of the sun. To overcome this challenge, the nurses used a strategy that consisted of showing pictures of the sun's position at the time they were supposed to take the medicine. The prescription medicine came in a small enclosable plastic bag with four images of the sun and the moons different positions during the 24 hours of the day.
“If you say seven o’clock and you have to take it each six hours the person doesn’t understand, so you have to talk about “in the morning, midday and in the afternoon or evening”. This is where the thing is, you can’t tell that person that after each six hours or each 8 hours, each 12 hours, the person will not understand” (Nurse 2)
Nurses wish of improvement
The importance of receiving the updated and new research concerning medical material and women’s health, was something the nurses stated as a wish of improvement. To not have the access or possibility to find such new updated material was described as a challenge and demotivation. What the nurses had to rely on was their nursing education, working experience
and colleague’s knowledge, which often was enough, but not in a self-development purpose.
“She consider challenge or difficulties when they don’t have the updates. Because the updates are important, the refreshing in the area. New methods and so on in the maternal and
child health. And very particular in the family planning, for the women. Not to get pregnant now and again all the time in the hospital” (Nurse 5)
When leaving work to go home, there was one nurse that experienced that the information sheets that she was handing out earlier during the day, was found on the ground by the entrance to the hospital. The reason why the information sheet was thrown on the
ground had a connection to the patient’s low education level and their lack of reading and writing skills. The nurse pointed out that to be able to improve this situation, one option could be to replace the written information sheets with illustrating images. By using more images at the hospital, the nurses would not need to worry about the patient not understanding and throw the written information sheets away. This was something the nurses wished and believed could give a positive and affective outcome to improve.
"When she walks and before she reaches the gate she can find the information sheets somewhere thrown on the ground. At the time the woman doesn’t read and the husband as well. Both of them do not read, they did not go to school to learn how to read and write. That’s why the images are better” (Nurse 6)
Many of the interviewed nurses mentioned a wish for more material to be able to hand out to the patients after a consultation. They had only a limited number of material to use at the hospitals, which made it hard to reassure that the patient actually would remember what was said at the consultation. If the extra material existed, the patients would be able to share knowledge from the consultation with their family and friends, which could help the nurse’s wish of improvement. The wish for more material to hand out to the patients were one continuous factor that was brought up to be able to improve the circumstances.
“They’re lack of this material, it is very welcomed to have them, it helps to have a booklet. They can not give the patients because there is very few” (Nurse 4)
The nurse's pointed out that the distance between the hospitals in Maputo province was far and a lot of times were also hard to get there without a vehicle. This forced many pregnant women to walk to the hospital, which in itself was a risky thing to do regarding the safety of the mother and the baby. During rain season, the roads became flooded and destroyed which made it even harder. Travelling during the night brought additional challenges due to the lack of street lights and the thought terrain. Therefore, the nurses wished that there was a certain vehicle assisting with transporting the pregnant women to the hospital to avoid the risks that could arise while being pregnant and when walking such distance.
“We know that people live far away like 5-10 kilometers, or more, and it's in the night it's challenging. They got a house in the back of the hospital area, they call it the waiting room. The people that lives far away from the hospital, when time comes they come in to stay here and will stay till the delivery day” (Nurse 2)
Tools for giving information to reach out in rural areas
The theme illuminates what tools the nurses used to prevent health issues and how the nurse’s worked with spreading and giving information in rural areas in Maputo province. The theme
was divided into three sub-categories, preventive work, education and community work. In this main category, the focus is on the outreach work that the nurse conduct to prevent illness among women’s health.
Preventive work
To reach out to the local people living far away from hospitals and health clinics, some nurses told that they used the radio as a way to reach out and inform. The radio was a device that almost everyone had at home or at work. Therefor it was a considerably practical tool that provided an option to reach out with information which brought a greater awareness. They broadcasted these programs about three times per day where they talked about how to prevent illness and why and when you should seek help at the hospital. There was also specific topics that they discussed at the radio. For an example, if you were not capable to attend today’s session about the importance of breastfeeding your baby, it was possible to catch up on the radio.
“Let’s say she goes there to make the session and some are at work, others are at the farm, so they miss it. But when it comes in the radio they will listen to it. Because during the day, they might be talking about it, two, three, four times until you are reached by the
information” (Nurse 7)
Some preventive work was described by the nurses as targeted informative TV-programs. One TV-program focused on prevent young girls from becoming pregnant at young age before the body is physically ready. The TV-program showed some of the consequences that could occur at early pregnancy and the nurses found that this was closely linked to young marriage in rural areas.
“On TV, there were cases of, I will put it to girls like fourteen years’ old, fifteen years old that got a baby but because of their still young, not prepared, they end up having fistulas. So, what she was hearing they were teaching to avoid being pregnant when they are still young. And she said that the education was, is more for the rural areas because this is where the thing happens, like that” (Nurse 6)
Education
To reach the teenagers in the community, some nurses went to visit schools and
educated them about sexual health. In this way, the nurses took responsibility to teach and educate about the biological development in the body and how to have safe sex without getting any sexual transmitted infections. In order to give the best nursing care, the nurses defined this kind of work as important to develop health care and increase knowledge among the youths in the country. They felt it was important to talk about sexual health in early age, not only because of prevent early pregnancies but also to inform about the advantages to finish school and get an education.
“They go and visit the schools and they do sessions and the children will attend. The girls and boys attend to the sessions. To prevent the unwanted pregnancies and diseases of sexual transmission. When to have intercourse and what happens to the body. And then, to let them know that it’s good to grow without these problems and study. Be somebody and start to enjoy life the other way” (Nurse 7)
By having sessions with young couples, both received the same information about how their partner and their own body functions. The nurses counselled couples together, which
promoted and highlighted the importance of respecting and listening to each other. By talking and informing the couples of the importance of having sex on equal conditions the gender gap between women and men
“Most of the time they invite the boy and the girl. Let’s say that the girlfriend and the boyfriend and they should be together to be counselled. Hopefully, this makes women and men more equal” (Nurse 1)
Community work
To be able to provide good healthcare for everyone, even though you live far away from a hospital, the majority of the nurses in the study collaborated with traditional midwives and volunteers. The midwives and volunteers were people that lived in the rural area and small villages, who knew the people and the district. In this way, volunteer workers became the extended arm of the nurses. Nevertheless, this gave the nurses at the hospital a greater insight in who were in need for help and they could assist the volunteers when needed. The nurse’s offered regular training and education for the volunteers to maintain safe and good quality of the healthcare. By collaborating with the communities, the nurses spread and reached out with information, which in the long term could improve and prevent illness. By working like this, there were an ongoing communication between the patients and the people in rural areas.
“The volunteers receive a training here in the hospital for them to be able to spread the information. You educate women to go out in the province. And they’re getting good results, it’s a sort of preventive work” (Nurse 3)
Something the nurses had worked persistently with was to convince pregnant women to come to the hospital and have their baby there. To reduce the rate of children and maternity
mortality, this was something that the nurses emphasized as a crucial area to improve. The nurses described it as a tough process to get the local midwives to understand the importance of having the pregnant women to give birth at a hospital. The nurses perceived it as the local midwives had difficulties with comprehending with the fact that it is better to have the baby at the hospital. It was apprehended by the midwives that the nurses tried to take their job away from them. The nurses and local midwives talked it through and due to the
severe consequences that can arise by having a baby at home, both parts agreed that it was safer to deliver at the hospital. In turn, the nurses taught the local midwives how to follow and monitor the pregnancies in the rural and when it was time to go to the hospital.
“The midwives in the rural areas, they work together with the hospital. They used to deliver woman in the rural areas, in the community’s. Now the midwives tell them to go to the hospital” (Nurse 6)
To reach out to many people at the same time, some nurses said that they went once a month to workplaces close to the hospital to hold different sessions for the workers. Mainly it was men working at these places, which was a conscious choice by the nurses. The nurses used this strategy to involve the men in their wife's maternity health and informing them about why and when to seek help. The sessions were highly appreciated because the men were able to ask the nurse questions without their wife’s presence and discuss in a group together with other men. This was seen as an opportunity for the men to exchange experiences with each other. By giving these tools and information to the men, gave them the possibility to
understand the normal and detect abnormal conditions. By learning how to discover warning signs within one’s partner can prevent some seriously complications.
“Mainly it’s men working there. The nurses do session and when the men reach home they inform their wives and the wives comes to the hospital. The men, they even said that the nurses should come back more often” (Nurse 7)
DISCUSSION
The discussion below is divided into method discussion and discussion of result.
Method discussion
In order to respond to the study's purpose, a quality research design was chosen. It is
described by Bernard & Ryan (2010) that every field of science depends on well-developed methods to be able to answer the cause of the thesis (ibid). By using a qualitative research approach, the study is an ongoing decision-based process where realities and viewpoints are not all known at the beginning of the study (Polit & Beck, 2014). The researchers need to have a fundamental understanding of a flexibility regarding time-planning, human
interactions and cultural differences during their study (ibid).
Initially the interviews were supposed to be held with nurses working daily with outreach work for Focus Fistula Organization. However, there was no nurses yet connected to the organization that only worked with outreach work. This meant that the authors had to come up with a backup plan. After consulting with the supervisor in Maputo, the solution was to visit four rural hospitals in Maputo province. These nurses had daily experience with maternal health and spreading information and giving communication.
Data collection
The study was conducted on a relatively small group of seven informants which implies a certain limitation in generalizability (Polit & Beck, 2014). On the other hand, the credibility is strengthened due to the distance between the four different hospitals that was spread out over whole Maputo province. The concept of trustworthiness is connected to the findings in the collected data. The result should be a reflection of the personal or lived experiences of the phenomenon that is being studied (Curtin & Fossey, 2007). To achieve trustworthiness, one should use concepts and terminologies suitable to strengthen the aim (ibid).
To answer the aim of the study, semi structured interviews were held to gain a deeper
understanding of how the world is perceived by the informants. The interviews were set up so each informant was asked similar set of questions, all open-ended (Bernard & Ryan, 2010). By using open-ended questions allow the informants to use their own words, which in turn capture their view of ideas and thoughts (ibid). According to Polit & Beck (2014), during the interviews, the interviewer’s role is to encourage the informants to express themselves and talk freely. This was done by encouraging and confirming the informant to continue talking by just adding affirmative comments like “uh-huh” or “I, see” (Bernard & Ryan, 2010). When preparing for the interviews, the questions were read and discussed thoroughly between the authors and the supervisor at the university before departure. The focus was to ask
questions that reflected back and answered the study's aim. However, it turned out that during the interviews with the nurses, some questions seemed to be perceived as difficult
but the authors simplified the questions to the context until the informants understood what was asked. While using interviews to answer the aim, there was a need to be aware of the problem of missing data (Bernard & Ryan, 2010). This could be due to people's unwillingness to answer or a failure to ask a question in the right way (ibid). Therefore, we were critical against ourselves and evaluated after each and every interview to make sure we became satisfied with the results. This includes identifying issues, such as missing data.
The national language in Mozambique is Portuguese, which was spoken by all the nurses. The questions were translated from English to Portuguese with the help of an interpreter. The authors sometimes noticed that some answers were incoherent compared to the asked questions. When such an occasion occurred, a reformulation of the question was done to avoid misunderstandings. One of the main tasks, when it comes to using an interpreter according to Ingvarsdotter et al. (2010), is to decide what kind of pre-knowledge and insight this person should have in the studied area. The choice of interpreter can give different outcomes depending on what position of status she or he holds. If the informants know who the interpreter is, this might put them in a position of holding information back due to the maintaining relationship they have (ibid). When choosing an interpreter, the authors were recommended by their supervisor in Maputo to contact one. Before contacting the interpreter, it was decided by the authors that it should be female and that she was familiar with medical terminology.
It is important to keep in mind when using an interpreter that people have different ways of perceiving things due to different culture backgrounds, which may affect the results and answers from the informants. This might lead to two completely separate views of a problem, while during the actual verbal discussion, they seem to have a common comprehension (ibid). While working with an interpreter, it is of great importance that she/he is familiar in the study purpose, the interview questions and it is of the utmost importance that the confidentiality is kept, in relationship to participants and researchers (LeBaron et al, 2015).
Sample
To find suitable participants, the head nurse at each visited hospital was informed about the purpose of the study and then assisted with finding nurses based on the inclusion criteria’s. The suitable nurses were asked to participate in the study with an explanation that it was highly voluntary and confidential throughout the study. The seven nurses that got requested to participate in the study accepted.
Data analysis
To code and analyze the gathered data, a thematic content analysis described by Burnard et al. (2008) was carried out to analyze seven transcribed interviews. The analyze process
consisted of four steps. In this process it involved detecting patterns, repetitive words and phrases to then categorize them into a number of similar subcategories. Based on the
subcategories two main themes emerged that summarized the collected data (ibid). Neither of the authors had any earlier experience with analyzing and coding qualitative data. Therefore, this part of the process was perceived as very time consuming and frustrating considering trying to understand the procedure and the part of pairing the right words and phrases into fitting subcategories.
According to Curtin & Fossey (2007) to reassure the trustworthiness of the study, the researchers should involve the participants in the data analyzing process. This refers to letting the participants review the collected data and their specific transcript to enable them to
contribute to the study. This gives an opportunity for the participant to add any comments or to clarify if any misunderstandings have occurred during the interviews, that can be corrected (ibid). Due to size limitations of the minor field study, the authors were not able to meet the informants a second time because of a strictly budget and due to the travel distances. Burnard et al. (2008) suggests another way of having data analyses validated. By letting an
experienced and independently suitable researcher review the transcripts and coded data to strengthen the trustworthiness. Adding a third party, the minor field study was validated through the authors supervisor at Malmo University.
Discussion of result
Supported by previous literature and research, it was known that the Mozambican nurses struggled with many different daily challenges. All the interviewed nurses in this study agreed on that communication needed to be adapted for the individual person and situation to make sure that the message was understood. When the situation occurred of not speaking the same language, it was described by the nurses as one of the main problems of giving
communication and information. This contributed to a language gap between the nurses and the patients, which was perceived as time consuming and frustrating. By not knowing if the patient truly had understood what the nurses informed about the first time, they had to ensure themselves by doing so called follow-up questions for the patients.
To provide quality person-centered healthcare, it was emphasized by the nurses that given information needed to be in local language to be able to reach out to all rural communities. According to Macueve et al. (2009) the radio is described as the easiest and most accessible tool to provide and spread information. Through the radio, it was possible to educate families and communities far away which in turn gave them the capability of spreading knowledge and information (ibid). The local radio programs were highly appreciated by the nurses and the patient as it turned out to be an effective method to make people seek early help at the hospitals. It was defined as an important and fundamental tool to be able to provide equal information to everyone, no matter where you live or what social status you have. However, the radio is a practical tool in many ways, but it is also a form of a one-way communication. It was a collective communication method, which is not individualized.
Several nurses experienced situations where the patient would verbally confirm that they understood the given information, while the truth was the opposite. During the consultations, the patients was participating in the conversation by giving minimal responses such as “yes” and “mm” and no other supplementary questions were asked. This gave the nurses an
indication of that some parts of the conversation was perhaps not completely understood. It is described by Dalby Landmark et al. (2016) that some healthcare staff sometimes
overestimate their own ability to communicate and give information to patients. One reason of overestimating such situation is because patients do not always express their lack of
understanding or they might overvalue what they actually have understood (ibid).
Language barriers is by Azam Ali et al. (2017) described as a problem that arise when the nurse and the patient do not speak the same language. It is proven that it can jeopardize the safety of the patient by increasing the risk of adverse events such as medication errors and misunderstandings (ibid). The nurse’s solutions to overcome the language barriers that they encountered in this study was to call for a colleague to assist with translating into the patient’s local mother tongue. If there still were problems with understanding each other, other
common solutions were to use facial expressions, body language, gestures and booklets with images to make the patient understand. By involving the patients in the decision-making
regarding their own treatment, Dalby Landmark et al. (2016) suggest that it opens up for the opportunity for them to reject or accept the proposed treatment. When the patient is included and gives his/her consent, a mutual ethical approval is achieved. But to be able to know what is being rejected or accepted, a precondition is that the patient has truly understood what has been said (ibid).
Culture is defined by Tjallinks (2004) as a multifaceted concept that is used to divide people into different groups. Culture includes beliefs, ideologies, approaches and verbal and
nonverbal language. Culture is a phenomenon that is transferred over time and between generations (ibid). According to Jirwe et al. (2009), culture affects the people's interactions between each other and their beliefs as well as ideologies that exists within the group. Though, this does not mean that their beliefs need to be proven as true, because it has unconsciously been accepted as the true paradigm by the group. Over time, culture will evolve but it usually happens notelessly. This makes it a lot easier to point out other groups culture features than recognize your own (ibid).
The results demonstrate several different cultural issues that was highlighted as a problem regarding the nurse’s profession. A deep and old rooted culture that still lives among the Mozambican people sometimes had a negative impact on the nurse’s job. It was shown that instead of seeing a legitimized nurse as a first option, a lot of the patients went to a traditional healer. World Health Organization (2013) presented that the ratio of medical doctors in Africa is 1:40 000, compared to the large ratio of traditional healers which are 1:500. For millions of people in rural areas, this means that the accessibility to find and receive help from a
traditional healer is much easier and more available (ibid). This gives an explanation of why traditional healers still are used in such an extent.
Culture was undoubtedly an important factor that needed to be considered and met with respect. At the same time as culture could be an issue, the nurses knew the significance of not trying to reduce the women's beliefs and cultural background. Polygamy was something that still existed a lot in the rural areas. It was maintained due to the negative thoughts that came with being a single woman as well as the difficulties it implied to manage to provide enough food and money when being single. This meant that the patriarchate in the country was being preserved and women in rural areas will continue to be reliant of men. The nurses understood the reason why women chose to marry a man with several wives but still fought the
consequences of early pregnancies and obstetric complications that came with it.
A widely spread of child marriages takes place in Mozambique which gave consequences that the nurses had to encounter on daily basis. The early marriages limited the young women's school attainment and had a negative influence on their health and body. The study identified reading and writing problems among the women due to the early marriages and not completed their school education which complicated the nurses work when it came to giving written information. The nurses felt that there was a challenge to make the women understand the anatomy and the physical changes that comes with a pregnancy. Nguyen & Wodon (2014) says that the earlier a girl is married, the lower the probability that she is literate. It is mentioned, that in many countries, laws have been established to protect and prevent girls from marry before 18 but unfortunately these laws are not fully followed (ibid).
As a strategy to reach women, some nurses turned to the husbands working at the local village factories. There the nurses held informative sessions to educate the husbands about obstetric issues that could occur associated
with their wives' pregnancies and the possible consequences of delayed decision making. The nurses held the sessions with the men because they were aware of the men’s position in the households regarding economy and decision making. However, Firoz et al (2016) presents a number of determinants that affects the maternal health negatively in Mozambique. Lack of power to make decisions, inequality and lack of male support. In this study there was no insinuating of that the nurses in Maputo province felt that working in the rural areas was negative or a demotivation. There was material and instruments that they felt there was a lack of, but they did not express any dissatisfaction with the fact that they worked in rural areas. In a report presented by World Bank (2004) it was found that the healthcare staff in the rural areas had a much higher turnover at clinics and hospitals. The majority of the staff expressed a desire of wanting to transfer to other clinics and hospitals due to the lack of service
availability and opportunity for development and training possibilities (ibid). This may suggest that the available treatments in other provinces than Maputo province may be harder for the women to receive help in. Few educated healthcare professionals wanted to work in rural areas where they experienced lack of material which made the healthcare in rural areas in the country vulnerable.
CONCLUSION
For nurses in Maputo province, Mozambique, communication implies as an essential skill to be able to provide good healthcare for the women that live in rural areas. Different strategies and tools were identified among the nurses to prevent unwanted obstetrical complications. To reduce the maternal mortality in the province, the nurses in the study had built up a network of volunteers and local midwives in the rural areas, that cooperated with the hospitals. The nurses put a lot of time and effort to educate and visit communities to raise the awareness and enlighten the importance of not delaying the decision of going to the hospitals when needed. The challenges that the nurses encountered regarding reaching out with communication and information was sometimes described as frustrating. Not having enough material to hand out to the patient nor having access to the newest updated material was a demotivation. To achieve the best results, the information should be given in local languages since far from everyone speaks Portuguese. To reach as many as possible in rural areas, the radio was the most effective method. There was a desire to broadcast more health-related programs and these programs should be in mother tongue. Even though this was a small study, it indicates that the nurses need to adapt and individualize their communication techniques after their patients to prevent obstetric issues in rural areas.
FURTHER RESEARCH AND VALUE FOR THE
STUDY
In this study, we have sought to identify different methods and strategies that the nurses used to promote young women's health. By clarifying what strategies the nurses in Maputo
province use and what strategies that are most effective to address preventive work, it was also suggested that some areas could be improved to help future nursing generations.
From the perspective of the Focus Fistula organization, it would be of interest to invest time and money in the findings that are presented in this study, in order to prevent the occurrence
of obstetric fistulas. Studies like this one where the focus was on describing and illuminating communication and information methods to promote young women's reproductive health in rural areas, should be encouraged to investigate by others. The study was carried out in
Maputo province only, which may imply that the result would differ if it were implemented in other provinces in the country. By expanding studies to other provinces in Mozambique and/or African countries, it will be possible to compare the communication and information strategies and techniques and possible inspire one another, in order to gather the best
REFERENCES
Azam Ali P, Watson R, (2017) Language barriers and their impact on provision of care to patients with limited English proficiency: Nurses’ perspectives.
Journal of Clinical Nursing, 2018;27:e1152–e1160.
Bernard H R, Ryan G W, (2010) Analyzing Qualitative Data Systematic Approaches. Los Angeles, Sage.
Burnard P, Gill P, Stewart K, Treasure E, Chadwick B, (2008). Analysing and presenting qualitative data. British Dental Journal, 204, 429-432.
Cook R J, Dickens B M, Syed S, (2004) Obstetric fistula: the challenge to human rights. International Journal of Gynecology & Obstetrics, 87, 72–77.
Curtin M, Fossey E (2007) Appraising the trustworthiness of qualitative studies: Guidelines for occupational therapists. Australian Occupational Therapy Journal (2007) 54, 88–94. Dalby Landmark A M, Svennevig J, Gerwing J, Gulbrandsen P, (2016) Patient involvement and language barriers: Problems of agreement or understanding?
Patient Education and Counseling 100 (2016) 1092–1102
Firoz T, Vidler M, Tatenda Makanga P, Boene H, Chiaú R, Sevene E, Magee L
A, Dadelszen P, Munguambe K, Community CLIP Working Group, (2016) Community perspective on the determinants of maternal health in rural southern Mozambique: a qualitative study. Reproductive Health, 13, 124-131.
Focus Fistula Organization, (2016) >http://focusfistula.org/en/?page_id=945< (2017-02-01) Hartung S, Miller M, (2018) Rural Nurse Managers’ Perspectives into Better Communication Practices. Journal of community health nursing 2018, vol 35, no.1, 1-11
Ingvarsdotter K, Johnsdotter S, Östman M, (2010) Lost in interpretation:The use of interpreters in research on mental ill health.
International Journal of Social Psychiatry 58(1) 34–40.
Jirwe M, Momeni P, Emami A, (2014) Kulturell mångfald. I: Friberg F, Öhlén J, (Eds) Omvårdnadens grunder (2nd edition). Kristianstad, Studentlitteratur AB. Kourkouta L, Papathanasiou I, (2014) Communication in nursing practice. Mater Sociomed. 2014 Feb; 26(1): 65-67
Kvale S, (2014) Den kvalitativa forskningsintervjun. Lund, Studentlitteratur AB.
LeBaron V, Iribarren S, Perri S, Beck S, (2015) A practical field guide to conducting nursing research in low- and middle-income countries. Nursing outlook 63 (4) 462-473.
Macueve G, Madlate J, Ginger L, Gaster P and Esselina Macome, (2009) Women's use of information and communication technologies in Mozambique: a tool
for empowerment?. I: Buskens I, Webb A, (Eds) African woman & ICTs Investigating Technology, Gender and Empowerment. (1st edition) London, Zed Books Ltd.
Munguambe K, Boene H, Vidler M, Bique C, Sawchuck D, Firoz T, Tatenda Makanga P, Qureshi R, Macete E, Menéndez C, Dadelszen P, Sevene E, (2016) Barriers and facilitators to health care seeking behaviors in pregnancy in rural communities of southern Mozambique. Reproductive Health, 13, 84-97.
Nguyen M C, Wodon Q (2014) IMPACT OF CHILD MARRIAGE ON LITERACY AND EDUCATION ATTAINMENT IN AFRICA >
http://allinschool.org/wp-content/uploads/2015/02/OOSC-2014-QW-Child-Marriage-final.pdf< PDF (2018-05-29) Polit D & Beck C T, (2014) ESSENTIALS of NURSING RESEARCH: Appraising Evidence for Nursing Practice. Philadelphia, USA: Lippincott Williams & Wilkins.
The Swedish Resarch Council,
(2002) Forskningsetiska principer inom humanistisk- samhällsvetenskaplig forskning. >http:// www.gu.se/digitalAssets/1268/1268494_forskningsetiska_principer_2002.pdf< (2017- 02-20)
Swedish Society of Nursing, (2011) Foundation of nursing care values >
https://www.swenurse.se/globalassets/01-svensk- sjukskoterskeforening/publikationer-svensk-sjukskoterskeforening/etik-publikationer/foundation.of.nursing.care.values.pdf< PDF (2018-04-30)
Swedish Society of Nursing (2017) Strategy for improving the quality of nursing
>file:///C:/Users/User/Documents/MFS/Mozambique/strategy_for_improving_the_quality_of _nursing.pdf< PDF (2018-04-28)
Tjallinks J E (2004) Cultural Competence. I: Tjale A, De Villiers L, (Red.) Cultural Issues in Health and Health Care: A Resource Book for Southern Africa. Juta Academic, Cape Town. Unicef, (2016) A fair chance for every child.
>https://www.unicef.org/publications/files/UNICEF_SOWC_2016.pdf< (2017-02-03)
Unicef (2016) Child marriage. >https://www.unicef.org/protection/57929_58008.html< (2017-02-05)
Unicef (2014) Fakta: Mozambique
>https://unicef-porthos-production.s3.amazonaws.com/mocambique-fakta.pdf< PDF (2017-03-15)
USAID (2017) EDUCATION >https://www.usaid.gov/mozambique/education< HTML (2018-05-22)
Wiklund Gustin L & Lindwall L, (2012) Omvårdnadsteorier i klinisk praxis. Stockholm, Natur & Kultur.
World Bank, (2017) Development challenges
World Bank (2017) Country Overview
>http://www.worldbank.org/en/country/mozambique/overview< (2018-06-02)
World Bank (2004) Primary health care in Mozambique
>http://siteresources.worldbank.org/AFRICAEXT/Resources/ww11888final201.pdf.pdf< PD F (2018-06-03)
World Factbook (2011) Mozambique > https://www.cia.gov/library/publications/the-world-factbook/geos/mz.html< HTML (2018-05-26)
World Health Organization (2015) Mozambique's health system
>http://www.who.int/countries/moz/areas/health_system/en/index1.html< HTML (2017-02-03)
World Health Organization (2013) WHO Traditional Medicine Strategy
2014-2023 >http://apps.who.int/iris/bitstream/handle/10665/92455/9789241506090_eng.pdf;jsessio nid=7A91AF437D75A4756CE29291C050BF6B?sequence=1< PDF (2018-05-21)
World population review (2018) Mozambique Population.
>http://worldpopulationreview.com/countries/mozambique-population/< HTML (2018-06-03)
APPENDIX 1
General questions:
1. How long have you worked as a nurse?
2. Have you heard of Focus Fistula organization?
3. Tell us about how you came in touch with Focus Fistula organization. 4. Tell us about a typical day at your work where you use communication and
information.
Interview questions:
1. What methods do you use to communicate and give information to women? 2. Is there anything you can be better at regarding communication and giving
information?
3. What challenges do you experience when meeting women, regarding communication and information?
4. What motivates you to help these women?
5. What is the hardest part of your work, considering communication and information?
6. How could/would you like to improve the communication and information with these women?