43
Abstract—The rapidly growing use of mobile technologies has increased pressure on the demand for mobile-based data collection solutions to bridge the information gaps in the public health sector. In this paper, a prototype for mobile health data collection (MHDK) is proposed. MHDK is built based on open source data collection frameworks. The proposed prototype offers ways of collecting health data through mobile phones and visualizes the collected data in a web application. The evaluation of the prototype seems to show the feasibility of mobile technologies, particularly open source technologies, in improving the health data collection and reporting systems for the developing world. The use of cellular phones for public health service monitoring and evaluation is therefore one of the most promising developments in the quest to achieve improved public health services.
Keywords— Health data, mhealth, developing world. I. INTRODUCTION
ATA collection is one of the important components of public health systems. Decision makers, policy makers and health service providers need accurate and timely data in order to improve the quality of their services. Health data is used as input on health systems in policy making process. Health data is used in analyzing and predicting the health outcomes such as mortality and diseases outbreaks [1]. Health data could also be used for monitoring and evaluating the health services coverage. Drugs stock level data could be used to track and plan drugs distribution logistics in remote healthcare centers. Furthermore the statistical health data can be used to detect and track diseases outbreaks.
Health Management Information Systems (HMIS) in most developing countries are not efficient and this is probably due to unreliability of health data which causes underreporting to the managerial level where decisions and plans are made [2]. In the resource limited settings like in the developing world, evidence based decision-making is important to serve for the available resources. Therefore data driven decision-making is worth for wise and effective distribution of the available resources.
D. Shao is with School of Virtual Education, The University of Dodoma, P.O. Box 490, Dodoma, TANZANIA (email: deoshayo@ hotmail.com).
A. Loconsole is with the School of Technology of the University of Malmo, Sweden (e-mail: annabella.loconsole@mah.se).
B. Hajinasabrazlighi is with the School of Technology of the University of Malmo, Sweden (e-mail: banafsheh.hajinasab@mah.se)
In the developing world, socioeconomic barriers and geographical reasons have hindered the availability of potential health data. These barriers have affected the data collection methods, which are mostly manual, and paper based. Data collected through these manual methods are not standardized and therefore difficult to process for analytical and data mining purposes [3]. The exponential growth of human population in these regions increases challenges to health practitioners in dealing with large volumes of health data.
Health data processing between different levels of health care systems have been affected by this growth as manual aggregation of large volume of data is now a tedious work and has high error rate. In addition to that, the critical shortfall of the health workers in these regions affects the effort of improving the data collection and analyzing process. Poor data collection methods have leads to lack of clear understanding of the flow of health data. If the flow of health data is not clearly understood by the decision makers, fulfilment of the plans and the policies that are created to improve health services may be difficult [2].
While the Internet revolution passed by without appreciably changing the lives of many people in the developing world, mobile technologies offer immediate advantages. Several studies have proposed mobile technology as the candidate technology in improving remote data collection in the developing world and even in isolated regions of developed world [4,5] .The discussion on the use of mobile technology in data collection has been motivated by the advancement of modern cellular technologies, which enables mobile devices to carry more capabilities in memory, processing speed and visual display. Furthermore, the mobile phones are portable and have long lasting battery life that could support remote collection of data in various geographical locations compared to laptop computers [6].
A. Research goals
The main objective of this paper was to study the challenges associated with health data collection and reporting from primary to secondary health facilities. The understanding of these challenges helped to propose a mobile-based health data collection prototype using open source tools. The proposed prototype aimed at identifying ways dealing with challenges in remote data collection for the purpose of improving monitoring and evaluating health facilities in remote areas.
M-Health: A Mobile Data Collection Prototype for Monitoring
and Evaluation of Public Health Service in the Developing
World
D. Shao, A. Loconsole and B. Hajinasabrazlighi
44 This paper is organized in sections and sub-sections; the first section presents background and related work on health information systems including challenges in data collection and information flows. Section two presents the research methodologies that have been adopted in this study. Section three presents the design of the proposed prototype and its evaluation. Lastly, we concluded with a discussion and suggestion of the future work in improving monitoring and evaluation of public health through mobile data collection.
II. BACKGROUNDAND RELATED WORK
A. Health Information Systems (HIS) in the
Developing World
HIS have become a crucial component for strengthening the health systems in developing countries [7]. There has been tremendous growth of these systems in recent years; this has been the result of advancement of technologies, which is taking place all over the world. HIS emergence has therefore lead to shifting from paper based to computer-based ways of processing health information. This shift has increased the opportunities of manipulating patient data efficiently. However, it has also raised challenges of technological complexity in using the advanced tools for processing health data. The usage of health data is extended not only for patient care and administrative purposes but also for planning and decision making in improving health services. Health care workers nowadays deal with large amount of data, which is a very error-prone situation, and it also increases the cost of accessing and using the data. Demand for technology based tools that could ease the data input and manipulating process is vital and is relevant in increasing the performance of health professionals. Ubiquitous network infrastructure which is now available worldwide, open up doors for new health information systems that could allow capturing of different types of data everywhere [7]. However implementation of HIS has been challenging to developing countries due to uncoordinated structures of their health organizations that cause unnecessary fragmentations of health systems, inconsistency and redundancy in reporting [8]. The lack of shared standards in data collection methods cause the gaps in reporting health data as it might lead to important data not to being reported. Furthermore lack of coordination between health care system levels in reporting health data lead to poor utilization of the collected data which might therefore affect the quality of service that is offered by HIS [9].
Proper data collection methods allow regular monitoring of health information systems [1]. Fig 1 shows different levels of health care system and the need of data in each level. Adequate and timely information at the top level is of crucial importance towards improving strategic plans of managing the primary facilities. Lack of adequate information may lead to negative impact to the health system such as underreporting of
important data [9]. Data collection units at the operational level needs to be equipped with appropriate technologies that
can lead to availability of adequate and timely information. Health data systems in remote areas of the developing world have been facing the problems in reliability of data and therefore hampering the delivery of quality of health services (Lucas, 2008). The use of mobile technology seems to be effective as an enabling technology for resource limited settings such as in the developing world [11,12,16].
Fig. 1 Levels of health care system and the data flow [1].
B. Public Health Monitoring and Evaluation
Systems
There are different categories of information that are reported to health managerial level for the purpose of monitoring and evaluating public health service performance. The categories of the information required include; population (health surveys), morbidity and mortality, health service activities, facilities, employee information, drugs distribution and financial information. This information is used to improve health services, especially in increasing accountability and planning progress monitoring in the developing world health systems [13]. There have been efforts of improving the health reporting systems in developing countries, however the demand for improving data collection methods is high due to advancement of technologies and increase of population [2].
The current effort in monitoring and evaluating health service is still not sustainable. In most of the developing world countries, District Health System (DHIS) has been deployed to monitor the performance of remote health care centers. With DHIS in place (see Fig 2), the methods through which data are collected and aggregated increase the risk of low quality of data and has been reported to affect the decisions that are made based on the data [14].
45
Fig. 2 DHIS information cycle in health facilities [14].
C: Challenges of existing health data collection
methods
Health data collection process has not been easy in the developing world due to several factors such as economical
constraints. Table 1 presents the challenges of existing health data collection methods as learned through questionnaire survey and literature review.
TABLE I
CHALLENGES OF EXISTING HEALTH DATA COLLECTION METHODS
Literature review Questionnaire survey
The current methods of collecting and reporting health data.
Paper based and partial computerized methods [14] [15] .
Paper based methods
Time for collection and reporting health data from primary health facilities to secondary facilities.
There are defined frequencies of reporting health data based on type of data and where there data is reported. The frequencies are in terms of weekly, monthly, quarterly and annually [15].
1. Monthly 2. Quarterly 3. Weekly 4. Yearly
It depends on kind of reports Kind of data collected and
reported from primary health facilities to secondary health facilities.
Facility records, birth and death registers, outpatient records [1] .
1. Number of diseases cases reported in health facilities
2. Medical equipment (medical assets) 3. Medical stock level information Users of health data Health statisticians and health managers
[15].
Doctors, government and medical researchers.
General challenges of data collection and reporting systems.
1. Limitation of resources such as human resources and health data processing tools [16][11] [17].
2. Lack of reliable communication infrastructure to support the transfer of data from remote health facilities to management levels (district level). 3. Lack of data accuracy and consistency
of reporting health data.
4. Fragmentation of health information system due to un-coordination between different levels of health care systems [14] [15].
5. The existing electronic data collection methods are mostly SMS based and they have limitations on data capturing capabilities [18].
1. Low data accuracy due of the paper based method in data collecting.
2. Delays in reporting crucial information to the managerial level.
3. General lack of capacity for data collection and processing (few health workers) 4. Poor record keeping methods and mostly are
in paper forms
5. Poor health infrastructure, which is exploited to serve large population, hampers the health data collection efforts.
46
D: Data Collection Frameworks
There are several open source projects that seek to improve the data collection process. Several data collection toolkits have been developed and released under general public license
(GPL). Table 2 shows the comparison of data collection frameworks reviewed in study.
TABLE II
COMPARISONS OF DATA COLLECTION FRAMEWORKS
Tool Data type Handset Protocol Storage License Case study
RapidSMS Text Basic Phones
GSM Local Open Source Surveillance, response monitoring and supply chain [19].
OpenX Data Text, Video, audio, images Java Phones GSMS, GPRS Bluetooth
Local Open Source Early warning systems and mhealth projects in developing countries [20]. Open Data Kit Text, Images, Video, Audio, GPS Android Phones GPRS, Wi-Fi
Hosted Open Source Government, business, health sector and education sector [11] [21].
Java Rosa Limited by headset and network
Java Phones
GPRS Hosted Open source Management of childhood illness via remainders and remote support [22] and in supporting community health care workers (CHWs) [23]. EpiCollect Text, Images,
GPS
Android, iPhone
GPRS, 3G, Wi-Fi
Hosted Open source Data collection suitable in regions where internet connection is not available [24].
E: Weaknesses of the current approaches
Despite of several efforts that have been made to address the health data collection challenges using mobile technology, the demand for improvement is vital. The introduction of newer technologies opens new opportunities of improvement. The followings are the gaps found in the previous way of collecting and reporting health data in the developing world.
Gap 1: There is fragmentation of health information system due to un-coordination between different levels of health care systems [8].
Gap 2: The current way of reporting health data from health facilities to management levels is subject to underreporting due to involvement of human being in collecting and aggregating data [14][15].
The current way of reporting health facilities routine data to the managerial level is not timely and may lead to delay in crucial decisions that could be more effective [15].
III. RESEARCH METHODOLOGY
In this study, a combination of three methods (Literature Review, Design and Creation and Qualitative study) has been used. Combining methods offers great promise on flexibility of the research and draw strengths from multiple methods and therefore allow the research to answer more broader questions that are not confined to only one method [25].
C. Research Methods
(i) Literature review
A documentary analysis was conducted in this study following seven steps as defined by Oates [26]. The steps are searching, obtaining, assessing, reading, evaluating, recording and writing a review. The review helped us to gain an understanding of the challenges of paper based and mobile-based health data collection.
(ii) Design and Creation
According to March and Smith [27], design and creation approach is used by researchers who focus on developing new IT products or artifacts, and its contribution to knowledge comes in the form of constructs, models, methods or instantiations. March and Smith [27], have further introduced a framework that should be used to conceptualize different activities that are involved in designing and IT artifact. In this study, March & Smith‘s framework was used to properly conceptualize and represent all the techniques to the solution. Table 3 presents the mapping of different activities and their outputs.
TABLE III
RESEARCH ACTIVETIES [27]
Build Evaluate Theorize Justify
Constructs
Model X X
Method
47
(iii) Evaluation study
Evaluation is an invaluable component of the research process [28]. The evaluation of the prototype was conducted through questionnaire and interview. The evaluation process helped to determine the applicability and usability of the prototype in facilitating monitoring and evaluation through remote data collection.
III. PROPOSED PROTOTYPE
After comparing the features of each framework in Table 2 based on the findings reported by Jung [29], we selected the open data kit (ODK) for developing the proposed prototype for health data collection.
The proposed prototype offers ways of collecting remote data through a mobile phone. These enable timely data collection in remote health facilities where resources such as electric power is limited and other communication infrastructure such as roads are unreliable. This could help patients, doctors, researchers and other stakeholders to improve health services by delivering valuable, actionable information to the right people at the time needed regardless of their location.
A. Stakeholders of the Proposed Prototype
Health data statisticians - These are the health record
management experts at the primary health care facilities whose duties are to track the health routine data and report to the high levels (see Fig 1). In mobile health data collection systems, these stakeholders shall be able to collect and report the health routine data through electronic forms, which will be accessible from the mobile client software.
Health system managers - The decision and policy makers at
the secondary health facilities whose tasks are to visualize, analyze and make informed decisions to improve the health services.
Other stakeholders - During the questionnaire survey carried
in this study other possible stakeholders were identified. These include doctors, medical researchers and government agents. However due to the time limitation, these users could not be incorporated in the proposed prototype. Therefore, in future studies this could take this group onboard.
B. Components of the Proposed Prototype
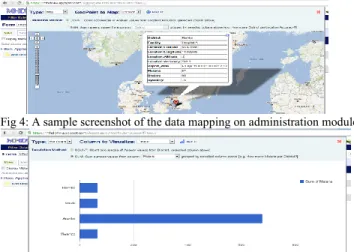
The proposed prototype was developed on top of open data kit framework using Java and XML language. The prototype functionalities were implemented in Android software development kit (SDK). XML was used to design sample data collection forms and Java language was used in the backend module.The collected data can be visualized in two ways, which are maps and simple graphs. Figs 4 and 5 show how the data can be visualized in maps and graphs respectively.
Fig 4: A sample screenshot of the data mapping on administration module
Fig. 5 Sample screenshot of the bar graph of districts against malaria reported cases
The prototype has several components that work together to improve the efficiency of mobile health data collection. The components are XML forms authoring tools, ODK aggregate (MHDK Viewer), Mobile phone client software (ODK collect).
The prototype has a client module, which is composed of mobile application to gather data, administration module consist of web application to manipulate gathered data, and form authoring tools to design data gathering forms (XML forms). Fig 3 shows how the different components relate to each other.
The Xforms are designed using XML editors such as ‘ODK
build’1, which offers flexible visual form design. However it may require further hand coding of the form logic (the order of filling the data in a form). The Xforms are created by the health managers and uploaded to the administration module (MHDK Viewer). The health statisticians then download the Xforms through client module (MHDK Collect) in a mobile phone. The filled Xforms are then sent back to the administration module where health managers can visualize and process data for management purposes such as decision and policy-making. The flexibility of the form design allows the prototype to work with various terminologies (data elements) and allows integration of data from different sources (different primary health facilities). The collected data can be visualized in form of simple graphs and data mapping.
48
Fig. 3 The main components of the proposed prototype (proposed in this work)
C: Evaluation of the Prototype
Evaluation is an invaluable component of the research process. According to Hevner et al. [28], there are different ways in which IT artifacts can be evaluated. The ways are functionality, completeness, usability, consistency, accuracy, performance, reliability and how it fit with the context. The evaluation process of this study aimed to evaluate the functionality and usability of the proposed prototype through a qualitative method.
The priority in participants’ selection was given to the people who have knowledge of the health systems in the developing countries. Therefore we targeted public health
international students, medical researchers and health service managers. We found contacts of the participants through colleagues and organizations websites. The participants were from Kenya, India, Ghana, Tanzania, Ethiopia, Zambia, Malawi, Uganda and Fiji. About 90% of the contacted people responded to our questionnaire. 100% of the interviewed people who were also given chance to use and test the prototype had a good satisfaction level. Table 4 presents the results of user suggestions on functionality and their usabilities.
Table III:
Prototype functionalities and their level of usabilities base on users experience in evaluation study
Module Functionality /Task Usability Users key remarks
Administration Module System administrator/ma nagers Xforms creation 3 - Xforms uploading/publishing 2 -
User creation and privilege setting 2 Users should be categorized and their submission should be marked/identifiable Data visualization and analysis (Data
manipulation)
2 More options for data visualization should be considered in the future.
Client Module
Data collector
Xforms downloading 1 Optimization of the form accessibility should be considered in future
Form filling 2 -
Form submission 1 -
Key:
1= It require very basic IT skills to be able to perform a task 2= It require an average IT skills t to be able to perform a task, 3= It require advanced skills to be able to perform a task
Copyright © 2012 JIVE ISSN 1821-7087 49 In general all participants in both questionnaire study and
interview study, supported the idea behind the proposed prototype and show their hopes that the prototype is applicable in their countries. The health data expert who was contacted in this study quoted saying “I believe this application could be
very useful in developing countries and also could save time, resources and workload”.
V. DISCUSSION
Current practices of collecting health data is through paper based methods where physical forms are filled and collected manually. The transcription of data for analysis is difficult and leads to low quality of data especially when the data volume is large. Furthermore, the supervision of multiple data collections from multiple locations is difficult and may lead to large time lag for data to be available for use. The proposed prototype has implemented electronic data collection forms that are easy to manage for remote health data collection from multiple areas. In addition, the proposed prototype has implemented data viewer module where collected data can be visualized and manipulated for analysis purposes. Compared to paper-based methods, which require extra efforts of filling the forms and thereafter entering the data manually in computer software such as spreadsheets, the proposed prototype has linked the data collection and data manipulation features. Therefore, the proposed prototype may reduce difficulties in data collection and minimizes the time lag for data to be available for usage. Data transcription with proposed prototype is simplified as the data is fed directly to the database through a mobile phone; therefore human data transcription errors is minimized and data accuracy has been increased.
The proposed prototype has capability of capturing data of all type such text, audio, video, images, barcodes, and GPS data. Therefore adds more flexibility in types of data that can be collected than other frameworks such as RapidSMS, FrontlineSMS [30] and Pendragon forms which have limitation in capability of collecting data. Furthermore, the prototype is customizable (flexible form design) and can be deployed in user defined settings compared to other mobile data collection frameworks which are close source and do not offer options to work with user defined settings such as custom data collection forms and other data visualization options.
The flexibility on terminologies used in data collection forms allows easy way of setting uniformity of data formats and therefore increases coordination of different levels of health information systems. Therefore, the proposed prototype can be used to capture health data for various types depending on the demand.
The framework selected to design the proposed prototype (ODK) is based on open source technologies, which allows future development with less effort, which can be affordable and manageable by the economies of the developing regions.
VI. C
ONCLUSIONS AND FUTURE WORKSIn this paper, we investigated the use of mobile technologies in improving monitoring and evaluation of public health system in the developing world. The proposed prototype was
developed to test the applicability and usability of the available mobile and open source technologies in improving the remote monitoring and evaluation of public health services.
The realization that mobile phone based health reporting systems are feasible in the developing world has important implications for health reforms in these parts of the world. It has already been observed that the use of mobile phones for communication is prevalent in the developing world and that the current paper-based reporting systems are not sustainable. There is thus the need for pilot projects to adopt new models such as the prototype proposed in this research in a controlled and experimental process in the field. This will provide the needed datasets for the review of the prototype and for streamlining future research works.
The future studies in this research area could attempt to develop the proposed prototype using data and specifications from the primary sources (actual stakeholders). Such works could also focus on enhancing health data visualization to improve the analysis process. For example, to enable data visualization through mobile phone screen (mobile interface for data visualization). The health data analysis process could also be improved in such a way that some of the decisions to be automated can be based on the collected data. For example, once the drugs stock level goes below certain value, the system can be triggered to provide alerts and suggestions to the health service managers about how to handle the stock run out. Furthermore, the future studies could look at the way different health data systems can be integrated to avoid duplication of data and maintain consistency in reports. In addition, future work could attempt to investigate ways of coordinating different health information systems levels to avoid fragmentation of flow of information through centralization of health data centers. Moreover, there is still room for investigating how open source frameworks could enhance other health management services in the developing world. For example, studies are needed to evaluate the applicability of different open source software packages for health service management in the developing world.
VII. ACKNOWLEDGEMENTS
We would like to thank all reviewers for helpful comments and suggestions in our work. We further thank the ODK experts for their technical support that helped us especially in configuring and testing the proposed prototype. Thank you all.
REFERENCES
[1] C. Abouzahr and T. Boerma, “Policy and Practice Health information systems : the foundations of public health,” Bulletin of the World Health
Organization, vol. 014951, no. 04, pp. 578–583, 2005.
[2] A. S. Nyamtema, “Bridging the gaps in the Health Management Information System in the context of a changing health sector.,” BMC
Medical Informatics and Decision Making, vol. 10, pp. 1–36, Jan.
2010.
[3] P. Mechael, H. Batavia, N. Kaonga, S. Searle, A. Kwan, A. Goldberger, L. Fu, and J. Ossman, “Barriers and Gaps Affecting mHealth in Low
Copyright © 2012 JIVE ISSN 1821-7087 50
and Middle Income Countries : Policy White Paper,” mHealth Alliance, pp. 1–79, 2010.
[4] S. Kulkarni and P. Agrawal, “Smartphone driven healthcare system for rural communities in developing countries,” in Proceedings of the 2nd
International Workshop on Systems and Networking Support for Health Care and Assisted Living Environments - HealthNet ’08, 2008, vol. 8,
pp. 199–6.
[5] Y. Anokwa, C. Hartung, and W. Brunette, “Open Source Data Collection in the Developing World:Open Data Kit enables timely and efficient data collection on cell phones, a much-needed service in the developing world.,” Invisible Computing, no. October, pp. 97–99, 2009. [6] L. Diero, J. K. Rotich, J. Bii, B. W. Mamlin, R. M. Einterz, I. Z. Kalamai, and W. M. Tierney, “A computer-based medical record system and personal digital assistants to assess and follow patients with respiratory tract infections visiting a rural Kenyan health centre.,” BMC
Medical Informatics and Decision Making, vol. 6, pp. 21–28, Jan.
2006.
[7] R. Haux, “Health Information System- past, present, future,”
International Journal of Medical Informatics, vol. 75, no. 3–4, pp.
268–281, 2006.
[8] S. A. Mengiste, “Analysing the Challenges of IS implementation in public health institutions of a developing country : the need for flexible strategies .,” Journal of Health Informatics in Developing Countries,, vol. 4, no. 1, pp. 1–17, 2010.
[9] O. Hanseth, A. Heywood, and T. Fax, “Developing Health Information Systems in Developing Countries: The flexible standards strategy,” MIS
Quarterly, vol. 31, no. 2, pp. 381–402, 2007.
[10] H. Lucas, “Information and communications technology for future health systems in developing countries.,” Social Science & Medicine, vol. 66, no. 10, pp. 2122–32, May 2008.
[11] S. J. Piette John, Blaya Joaquin, Lange Lilta, “Experiences in mHealth for Chronic Disease Management in 4 Countries,” in Disease
Management, 2011, pp. 1–5.
[12] R. N. M. Raoul M Kamadjeu, Euloge M Tapang, “Designing and implementing an electronic health record system in primary care practice in sub-Saharan Africa : a case study from Cameroon,”
Informatics in Primary Care, vol. 13, pp. 179–186, 2005.
[13] M. Morgan, N. Mays, and W. W. Holland, “Review article Can hospital use be a measure of need for health care ?,” Journal of Epidemiology
and Community, vol. 41, pp. 269–274, 1987.
[14] K. H. A. Garrib, N. Stoops, A. Mckenzie, L. Dlamini, T. Govender, J. Rohde, “An evaluation of the District Health Information System in rural South Africa,” South African Medical Journal (SAMJ), vol. 98, no. 7, pp. 549–552, 2008.
[15] M. Mahundi, J. Kaasbøll, and H. Twaakyondo, “Health Information Systems Integration in Tanzania : Tapping the Contextual Advantages,” in IST-Africa Conference Proceedings, 2011, 2011, pp. 1–11.
[16] D. A. Patil, “Mobile for Health ( mHealth ) in Developing Countries : Application of 4 Ps of Social Marketing,” Journal of Health Informatics
in Developing Countries, vol. 5, no. 2, pp. 317–326, 2011.
[17] M. R. Oak, “A review on barriers to implementing health informatics in developing countries,” Health Informatics in Developing Countries, vol. 1, no. 1, pp. 19–22, 2007.
[18] C. Bexelius, H. Merk, S. Sandin, A. Ekman, O. Nyrén, S. Kühlmann-Berenzon, A. Linde, and J.-E. Litton, “SMS versus telephone interviews for epidemiological data collection: feasibility study estimating
influenza vaccination coverage in the Swedish population.,” European
Journal of Epidemiology, vol. 24, no. 2, pp. 73–81, Jan. 2009.
[19] R. S. Sean Blaschke, Kirsten Bokenkamp, Roxana Cosmaciuc, Mari Denby, Beza Hailu, “Using Mobile Phones to Improve Child Nutrition Surveillance in Malawi Using Mobile Phones to Improve Child Nutrition Surveillance in Malawi UNICEF Malawi and UNICEF Innovations Solutions,” 2009.
[20] A. C. Noordam, B. M. Kuepper, J. Stekelenburg, and A. Milen, “Improvement of maternal health services through the use of mobile phones.,” Tropical Medicine & International Health : TM & IH, vol. 16, no. 5, pp. 622–6, May 2011.
[21] Z. A. Rajput, S. Mbugua, D. Amadi, V. Chepng’eno, J. J. Saleem, Y. Anokwa, C. Hartung, G. Borriello, B. W. Mamlin, S. K. Ndege, and M. C. Were, “Evaluation of an Android-based mHealth system for population surveillance in developing countries,” American Medical
Informatics Association (AMIA), vol. 19, no. 2, pp. 1–6, 2011.
[22] N. L. Brian DeRenzi, Gaetano Borriello, Jonathan Jackson, Vikram S. Kumar, Tapan S. Parikh, Pushwaz Virk, “Mobile Phone Tools for Field-Based Health care Workers in Low-Income Countries,” Mount Sinai
Journal of Medicine, vol. 78, no. 3, pp. 406–418, 2011.
[23] G. Mhila, C. Mushi, M. Steele, D. Roos, J. Jackson, B. Derenzi, T. Wakabi, P. Dhadialla, C. Sims, N. Lesh, D. International, and E. Development, “Using Mobile Applications for Community-based Social Support for Chronic Patients,” 2010.
[24] D. M. Aanensen, D. M. Huntley, E. J. Feil, F. Al-Own, and B. G. Spratt, “EpiCollect: linking smartphones to web applications for epidemiology, ecology and community data collection.,” PloS one, vol. 4, no. 9, pp. 1– 7, Jan. 2009.
[25] R. B. Johnson and a. J. Onwuegbuzie, “Mixed Methods Research: A Research Paradigm Whose Time Has Come,” Educational Researcher, vol. 33, no. 7, pp. 14–26, Oct. 2004.
[26] B. J. Oates, “Reviewing the Literature,” in Researching Information
Systems and Computing, London: SAGE Publications, 2006, pp. 71–92.
[27] S. T. March and G. F. Smith, “Design and natural science research on information technology,” Decision Support Systems, vol. 15, pp. 251– 266, 1995.
[28] J. P. Alan R. Hevner, Sudha Ram, Salavatore T. March, “Design Science Information,” MIS Quarterly, vol. 28, no. 1, pp. 75–105, 2004. [29] C. Jung, “Humanitarian Operations Mobile Acquisition of Data,” 2011. [30] K. Banks and E. Hersman, “FrontlineSMS and Ushahidi - a demo,” in
2009 International Conference on Information and Communication Technologies and Development (ICTD), 2009, pp. 484–484.
![Fig. 1 Levels of health care system and the data flow [1].](https://thumb-eu.123doks.com/thumbv2/5dokorg/3974712.78093/2.918.473.831.272.506/fig-levels-health-care-data-flow.webp)