Faculty of technology and soci-ety
Computer science
Bachelor’s thesis
15 credits, undergraduate level
Psychosis simulated in virtual reality
-attitudes pre and post exposure.
Psykos simulerad i virtuell verklighet -Attityder f¨ore och efter exponering.
Pierre Leidbring
Degree: Bachelor of science 180 credits Field of study: Computer science Program: Systems developer Date of final seminar: 2018-05-29
Supervisor: Thomas Pederson Examiner: Ivan Kruzela
Sammanfattning
Studier har p˚avisat att de negativa attityder som en stor del av befolkning uppvisar mot mental oh¨alsa ¨ar en bidragande faktor till de stigma som omger m˚anga av dessa sjukdo-mar. Denna uppsats st¨aller tv˚a fr˚agor: hur kan en simulering av psykos konstrueras f¨or VR och p˚a vilket s¨att kan en s˚adan simulering p˚averka attityderna gentemot tillst˚andet psykos. I ett f¨ors¨ok att besvara dessa fr˚agor byggdes en prototyp med Unity3D och Google Resonance audio. Denna prototyp anv¨andes sedan i kombination med tv˚a enk¨ater f¨or att besvara fr˚agan g¨allande attitydf¨or¨andringar. Resultaten kom att visa att det ¨ar m¨ojligt att konstruera en s˚adan simulering samt att VR som medium uppvisar potential att p˚averka attityden hos anv¨andaren gentemot ¨amnet f¨or simulering. Som forts¨attning p˚a denna uppsats skulle framtida forskning kunna best˚a framtagningen av ett ramverk f¨or konstruerandet av simulering i VR. Framtida forskning skulle ¨aven kunna fokusera p˚a att upprepa enk¨aterna med ett st¨orre antal deltagare. Detta skulle leda till ett st¨orre dataset vilket i sin tur skulle fr¨amja belysandet av subtila skillnader i de potentiella atti-tydf¨or¨andringarna.
Abstract
Studies have shown that the negative attitudes held by a substantial portion of the general public towards mental illness is a contributing factor to the stigma surrounding illnesses such as schizophrenia and psychosis. This thesis asks two questions: how to construct a psychosis simulation using VR and in what ways such a simulation can affect the attitudes towards the illness. As an attempt to answer these questions a prototype was built using Unity3D and Google Resonance audio. This prototype was then used in conjunction with two surveys in order to answer the question regarding attitudes. The results showed that building such a simulation is possible and that VR holds potential to affect participants attitudes towards the subject of simulation. To build upon this thesis, future work could consist of establishing a framework for building simulations in VR. Future work could also consist of repeating the surveys with a larger number of participants which would yield a larger data set which in turn would promote the highlighting of subtle nuances in a potential attitude change.
Contents
1 Introduction 1
1.1 Background and related work . . . 1
1.2 Simulation of psychosis symptoms . . . 2
1.3 Research aim . . . 2 1.4 Research questions . . . 2 1.5 Thesis scope . . . 2 1.6 Jayway . . . 3 2 Method 4 2.1 RQ1 . . . 4 2.2 RQ2 . . . 5 2.3 Method discussion . . . 5 3 Theoretical background 7 3.1 Virtual reality . . . 7 3.2 Unity3D . . . 7 3.3 Psychosis . . . 8 4 Literature review 9 5 Design 11 5.1 Conceptual framework . . . 11 5.1.1 Use case . . . 11 5.1.2 Requirements . . . 11 5.1.3 Problem breakdown . . . 12 5.2 System architecture . . . 13 5.3 System design . . . 14 5.3.1 Technical design . . . 14 5.3.2 State management . . . 15 5.3.3 Audio . . . 15 5.3.4 Scenario design . . . 16 6 Implementation 18 6.1 VRTK . . . 18 6.1.1 Unity3D . . . 18 6.1.2 Steam VR . . . 19 6.2 Resonance Audio . . . 19
7 Results and discussion 21 7.1 Participants . . . 21 7.2 Survey design . . . 21 7.3 Procedure . . . 21 7.4 Results . . . 23 7.4.1 Simulation . . . 23 7.4.2 Attitudes . . . 24
7.5 Discussion . . . 24
8 Conclusions and future work 26
8.1 Future work . . . 26
A Appendix 28
A.1 Surveys . . . 28 A.2 Survey results . . . 30
1
Introduction
1.1 Background and related work
A psychotic person often shows two main symptoms, delusions and hallucinations[6]. Delu-sions often manifest as strong beliefs that are not held by others and that may be considered irrational and are some times paranoid in nature. These delusions can also take the form of perceived conspiracies directed towards one self.
Hallucinations during psychosis can be experienced through all the five senses. Common examples of hallucinations are seeing shapes and colors, hearing voices, feeling touched even though one is alone, smelling things others can’t smell, the sensation of taste even though ones mouth is empty[6].
Prior research show that the general public as a group present negative attitudes and emotions towards those suffering from mental illnesses, especially towards those suffer-ing from schizophrenia and psychotic conditions[1]. Amongst the aforementioned illnesses schizophrenia is met with the least positive attitudes. These negative emotions and atti-tudes seems to stem from a combination of fear and the presumption that people suffer-ing from schizophrenia would be prone to show violent and/or unpredictable behaviour through which they could be potentially dangerous[1]. Together these negative emotions and attitudes form a stigma surrounding schizophrenia and psychosis with the potential to induce real world consequences for those suffering from the illnesses. Some of the possible consequences includes increased social distance and discrimination. The stigma surrounding these illnesses has in turn led to a prevalent shame in those suffering from the aforementioned illnesses. Due to this shame, those suffering from schizophrenia and psychotic illnesses are less likely to seek help for their conditions. The effects of people experiencing these illnesses not seeking help could potentially have a negative impact, not only on a personal level but also on a societal level[1].
Aside from neuroscience and psychiatry, several other disciplines within academia has taken an interest in the research around mental illnesses. With the advances in computing and the spread of internet it has become magnitudes easier to inform and educate the general public. Building upon this fact, several systems has been implemented trying to simulate the symptoms of schizophrenia and psychosis in order to educate, inform and to research the attitudes towards people faced with these illnesses[2][4][18]. Earlier software implementations aiming to simulate visual and auditory hallucinations often associated to schizophrenia exist in a wide range of styles. There are examples of distributed versions being deployed on the internet through a massive multiplayer online game by the name of Second life[18]. The interface to this simulation consisted of a traditional computer interface where the user utilizes a mouse, keyboard and a screen. Other implementations make use of old, more primitive, iterations of VR(Virtual reality) headsets[2].
1.2 Simulation of psychosis symptoms
Several attempts to implement systems simulating the symptoms associated with schizophre-nia and psychosis has been done prior to this paper[2][4][18]. All which aim to raise the awareness of these illnesses amongst the general public. Among these earlier attempts to raise awareness and promote education on the subject of schizophrenia and psychosis lo-fi systems has been implemented[2][18]. Even though the experiments utilizing the systems yielded positive results they where quite brute and unrealistic in nature due to the techni-cal limitations of virtual reality at the time of study. Since the release of consumer grade VR headsets such as HTC Vive1 and Occulus Rift2 developers and researchers has seen
an increased availability of these devices3.
1.3 Research aim
The aim of this thesis is to contribute to the research regarding VR in the context of psychosis simulation. In particular using VR simulation of the symptoms associated with psychosis. This will be achieved by analyzing both the implementation of the simulation and the results yielded by the survey. Secondly this thesis aims to investigate in what way people’s attitude towards psychosis would be affected by the simulation.
1.4 Research questions
RQ1: How can a psychosis simulation be constructed using virtual reality?
RQ2: In what way can a VR-simulation simulating the symptoms of psychosis affect non-psychotics attitude towards those experiencing psychosis?
1.5 Thesis scope
When developing a VR-application there are a multitude of platforms, frameworks and code libraries to choose from. The simulation developed for this thesis is built with Unity3D4 with the addition of VRTK5, SteamVR6 and Google’s Resonance audio7. The target platform is Windows 10 and the VR-hardware consists of an HTC Vive headset and controllers. 1https://www.vive.com/us/ 2 https://www.oculus.com/rift 3 https://www.wsj.com/articles/virtual-reality-finally-catches-onwith-businesses-1496664000 4 https://unity3d.com/ 5 https://vrtoolkit.readme.io/ 6https://steamcommunity.com/steamvr 7 https://developers.google.com/resonance-audio/
The aim of the simulation is mainly to function as a proof of concept and to be used as a basis for the survey regarding attitudes towards psychosis. It is not meant to be used as an investigative tool for the application of VR in mental health nor is it meant to be used as a therapeutic tool by any means. However, it can function as a source of inspiration for future research.
The design of the prototype’s content such as which symptoms included and the design of these will be based strictly of the literature reviewed. Due to the varying nature of psychosis and the fact that each patient have individual versions of the symptoms a general interpretation was deemed more suitable for the prototype. Basing the prototype’s content on one or several peoples experiences poses ethical issues and may also skew the experience in a way that would make it less general and less relatable. Numerous attempts to contact psychiatric professionals was made in order to have them validate the prototype. However none of the contacted professionals responded.
1.6 Jayway
The stakeholder of this thesis is Jayway8, an international IT consultancy company with offices in Sweden, Denmark and USA. Jayway’s ambition with this thesis is to further explore the possible application areas of virtual reality. For this thesis Jayway has helped to formulate the research questions. They also contributed by providing hardware for development. Also their personal participated in the testing of the simulation.
8
2
Method
In order to answer both research questions, two methods have been applied. Since RQ1 builds upon the construction of a prototype, a method in line with software engineering practices was used.
To yield results and answers for RQ2 two surveys was utilized in combination with the simulation.
2.1 RQ1
For the development of the prototype for this thesis, system development as a research methodology was applied as presented by Nunamaker et al.[12]. This methodology consists of a systematical approach to construct and implement a system which is described in the five stages depicted below. Due to it’s agile nature this methodology provides a clear process structure and a possibility to revisit and change earlier stages as needed.
Figure 1: Workflow as suggested by Nunamaker[12]
As shown in Figure 1 this methodology consists of five stages performed in an agile man-ner. In the first stage a conceptual framework is constructed. The construction of this framework consists of researching the domain. For this thesis the domain is made out by VR and specifically VR simulations of psychosis and hallucinations. The research is performed in order to understand the domain and then to break down the problem of designing and implementing the following prototype. As a result of the domain research and problem breakdown a use case is formulated. Requirements are the identified from the use case.
Once the requirements are identified, a system architecture is designed. The architecture defines relationships between the systems components as well as the functionalities. The architecture is the basis upon which the system is designed and implemented. After the architectural design, the system itself gets designed.
The prototype gets implemented after the design phase. Once the system is implemented it is time to test the system in order to test the hypothesis. The testing of the system often includes another method such as observation, case study or survey in order to yield results[12].
In order to evaluate the prototype and answer research questions, users tests will be held. The user tests will consist of the participant filling out a form relating to their attitude towards psychosis and thereby providing data for RQ2. They will go through the VR-simulation and afterwards they will fill out the form once again. During this user test, every action that gets triggered in the prototype will be logged to a file together with all state changes that occur as a response to these actions. The prototype will then be evaluated on the basis of these logs in relation to the scenario design.
2.2 RQ2
RQ2 ”In what way can a VR-simulation simulating the symptoms of psychosis affect non-psychotics attitude towards those experiencing psychosis?” is a question regarding attitude. In order to measure the participants attitude pre and post exposure to the simulation, they will fill out a survey. This survey consists of questions regarding their attitude towards those affected by psychosis. The participants will fill out the survey before they partake in the simulation in order to establish their pre existing attitude towards sufferers of psychosis. They will then fill out the exact same survey directly after partaking in the simulation. By comparing the results of the two surveys, potential differences in attitude can be made visible. The surveys is utilizing the Likert scale[11].
In the context of this thesis, attitude will be defined as the opinions an individual hold towards another. Specifically opinions associated with negative emotions. The emotions focused on are fear and contempt. Actions based on these opinions and attitude will be left outside the scope of the thesis.
2.3 Method discussion
Nunamaker’s[12] ”Systems development as a research methodology” is chosen as method because of its alignment with agile systems development. It provides a framework that is both suitable for the development of a prototype, due to it’s agile nature, and for research.
An alternative method that would have great potential for this thesis would be action research. In the case of action research the prototype would have been developed in close
collaboration with a psychiatric professional. This would have increased the validity of the scenario depicted in the prototype. Action research was however not chosen because of two main reasons: the attempts to contact psychiatrists yielded no results and action research poses the risk of focus being transferred away from the prototype itself. The risk of moving focus away from the prototype was the major concern since this thesis aims to take a technical approach on the problems presented.
The method chosen for RQ2 is a survey based on the likert scale. This approach is inspired by the ”yes or no”-survey preformed by Yellowlees[18] in a similar study. In the interest of higher granularity and the possibility of detecting finer shifts in attitude a four grade likert scale was deemed more suitable.
In order to measure the percieved change in attitude over time a series of interviews could have been utilized. In such a scenario the participants would have gone through the simulation, been subjected to an interview directly afterwards and would then go through a number follow up interviews the coming weeks. Although this method have the potential to yield greater results it was deemed unsuitable due to the time constraint of this study.
3
Theoretical background
The following chapter serves as a concise, theoretical and technical explanation in order to ease the understanding of the rest of the paper. Virtual reality and psychosis are the focus points of the paper and will therefore be explained in this chapter.
3.1 Virtual reality
The term virtual reality(VR) lacks a clear definition but is most often used in reference to a computer generated 3D-world of an interactive nature. These 3D-worlds are most commonly interacted with via head mounted displays(HMD) such as HTC Vive or Oculus Rift.
VR creates the illusion of being in a virtual world in an immersive manner. The experience of VR consists mainly of two things, visuals and interaction. The visuals are usually presented using an HMD which utilizes stereoscopic rendering. Stereoscopic rendering is a method for rendering the same image on two side-by-side screens synchronously. The interaction part of VR is most commonly handled by collecting spatial data for the HMD. This data can consist of the HMD’s position in the 3D-world and rotation. Some HMDs eg HTC Vive make use of two controllers as well. The same type of data is collected for these as for the HMD itself. There is additional data resulting from listening for button presses and strokes on the touch pads. Aside from interaction with objects in the virtual world via the controllers the user must be able to move from one position to another. The concept of user motion in VR is called locomotion. There are different methods to achieve locomotion amongst which teleportation is one. Teleportation is often considered the more comfortable option since it does not risk causing motion sickness. Teleportation can be perceived as unnatural and sometimes even be detrimental to the immersion of the virtual world so it might not be the most suitable method for all VR applications. By the use of room scale the user can walk freely inside a small space surrounding the user inside the virtual world. This is done using the data the tracking device in the HMD[10].
3.2 Unity3D
Unity is a game engine available on linux, macOS and Windows. Unity allows the developer to make games using the Unity editor which provides a graphical interface to the engine API. Provided within unity are libraries for graphics, input handling, network, physics and audio. The developer can instantiate game objects using the graphical interface and then attach scripts on those objects. These scripts are written in the programming language C# utilizing both .NET9 and Mono10. Combined with the open source library VRTK and the
SteamVR middleware, unity provides an environment for both development and testing of VR applications aimed towards HTC Vive.
9https://www.microsoft.com/net/ 10
3.3 Psychosis
Psychosis is both a symptom and a condition[9]. Psychosis can have a multitude of causes, amongst which schizophrenia, bipolar disorder and drugs are some. Psychosis is characterized by a range of symptoms. Some of these are distorted perception of reality, delusions, hallucinations, a weakened or lost connection with reality and difficulties judging reality. Every patients experience is different. Some experience the full range of symptoms and others might not. The most common symptom is auditory hallucinations[6]. These hallucinations often manifests as voices speaking to the patient even though the patient is be them selves. It is quite common for these voices to utter statements of distaste or for them to voice their dislike for the sufferer. Combined with the often conspiratorial delusions that also is a symptom of psychosis, these voices can greatly weaken the sufferers connection with reality[6].
The hallucinations often experienced by those suffering from psychosis aren’t always au-ditory and can be visual instead. These are how ever less common[9].
4
Literature review
This systematic literature review will serve as a summary of the current state of the re-search regarding virtual reality(VR) technology within the mental health area, specifically in the domain of schizophrenia and psychosis. Aside from that it will also extend to earlier attempts to decrease the stigma surrounding these illnesses.
People suffering from schizophrenia and various psychotic symptoms are often met with a negative attitude. Examples of this being that people tend to seek out a greater social distance and are more inclined to recommend forced treatment of those suffering from schizophrenia compared to sufferers of depression, for example. This attitude amongst the general public results in a stigma for those in need of help with the aforementioned conditions. This stigma often manifests itself as shame and fear of getting help[1]. Several studies have been conducted in order to discover new ways of reducing the stigma-tization of mental illnesses, schizophrenia and psychosis in particular. Based on the thesis that experiencing the symptoms of schizophrenia first hand would have a greater im-pact on an individual’s attitude towards the illness, a study was conducted using VR simulation[15]. In the simulation the participant took the role of a person suffering from schizophrenia and was faced with the task to visit a pharmacy in order to get a refill on their prescription. While inside the pharmacy the other customers as well as the phar-macist would start plotting against the participant, this being made clear by the use of malicious statements directed against the participant. In parallel with the VR simulation, an empathy condition was performed. Here the participants were asked to imagine var-ious scenarios described by the experiment conductor and write down their feelings and thoughts regarding the scenario. Some participants took part in both the simulation as well as the empathy condition. The results of those taking part only in the simulation differed significantly from the control condition. Those taking only the empathy condi-tion showed a smaller difference from the control condicondi-tion and those taking part in both showed the greatest difference. The results being that the VR simulation induced greater perceptions of empathy when combined with the empathy condition.
The simulation approach to education on mental illnesses has been taken on other con-ditions as well, not just psychosis and schizophrenia. Upon identifying a problem of lack in understanding amongst family and friends to those suffering from illnesses tied to per-ceptual disturbances, a study using VR as a simulation tool was conducted. The study was built upon the notion of VR being a powerful medium for simulating things that would not be possible to experience otherwise due to VR’s large potential for immer-sive experiences[13]. The choice of VR as the simulation platform was also motivated by the results of prior studies showing that VR can be used to promote self-compassion in depression sufferers.
Even though VR technology yields a large potential for inducing empathetic emotions towards sufferers from psychosis, the research has not limited itself to the use of VR. Earlier attempts has been made in order to raise awareness about psychosis. A simulation utilizing the already large virtual platform ”Second life” was developed in 2006, in order
to simulate the experience of psychosis[18]. By making use of ”Second life”, which is a massive online multiplayer game, the reach of the study could be vastly extended as it could be conducted in a distributed manner.
After partaking in the simulation the participants filled out a form in which they de-scribed the impact the simulation had on their attitude towards people suffering from psychosis. Even though this simulation were lacking the immersive properties of contem-porary VR they showed a subjective increase in understanding for the symptoms common in schizophrenic as well as psychotic patients. The results showed 76% of the respondents had gotten an increased understanding of auditory hallucinations and that 69% thought that the simulation had improved their understanding of visual hallucinations[18]. VR research in the domain of mental health does not focus explicitly on the application in stigma reduction strategies. The research in this field can be split up into two primary areas of focus, understanding and treatment. Due to the immersive nature and interactive properties, VR lends itself well to education. In 2004 one of the first attempts to build a VR simulation for psychosis was made[3]. Due to the fact that VR had not been as developed and readily available at the time of the research, the focus of the study was primarily on the technology itself and whether it would be possible to simulate psychosis with VR. The study did conclude that once VR software for use in 3D environments was developed it could be of potential use in both the context of treatment as well as education about mental health[3]. In 2016 the potential of VR as an investigative tool for psychological processes was once again part of the conclusion of a study[17]. This outlook on VR was shared by Freeman et al in an article from 2008 in which seven uses of VR for psychosis was presented[8]. Amongst the seven use cases the simulation of psychotic symptoms was one. Freeman et al also proclaims that VR can be a powerful tool in the depiction of psychosis[8].
The stigma surrounding psychosis and schizophrenia is an often recurring point of interest in the research papers regarding VR and psychosis[8, 5, 7, 16]. This interest in the stigma towards psychosis and the pointed out potential of VR as an immersive educational tool proposes a research opportunity. There is research to be done regarding VR as a medium for education and raising awareness about psychosis. The prior research prompts the question if VR can be beneficial for improving the understanding of psychosis and if so, in what ways.
5
Design
This chapter aims to explain the design of the prototype. Various possible designs and technologies will be presented.
5.1 Conceptual framework
During the first phase of development it is most important to get a clear picture of the problem. In order to understand the requirements of the system a use case needs to be specified. With this use case as a background, requirements will be specified.
Focus during the first step of development lies on getting a clear picture of the problem. In order to achieve a greater understanding of the problem, it is broken down into smaller sub problems which are well defined. Before defining the requirements and breaking down the problem a use case is to be identified.
5.1.1 Use case
During the first meeting with Jayway theme was decided to be empathy and stipulated that the system must be developed for VR using HTC Vive. The theme of empathy was described as, by using VR the user should have the opportunity to place themselves in a situation or context in which they would not realistically find themselves otherwise. Based on the theme of empathy the idea of simulating psychosis was introduced. After some discussion, it was agreed that the prototype should consist of a scenario relatable to most people but experienced from the perspective of a person suffering from psychosis. The scenario within the prototype where to be made up of everyday tasks such as getting out of bed, taking medication, preparing breakfast and answering the phone.
5.1.2 Requirements
Upon closer examination, the proposed use case exhibits three main requirements in order to yield the data necessary to answer RQ1.
1. The user must be able to interact with the key objects e.g medicine containers and phones within the system.
2. The system must utilize sound in such a way that it is perceived as auditory halluci-nations. Meaning sound must be three dimensional and respect obstructing objects such as walls.
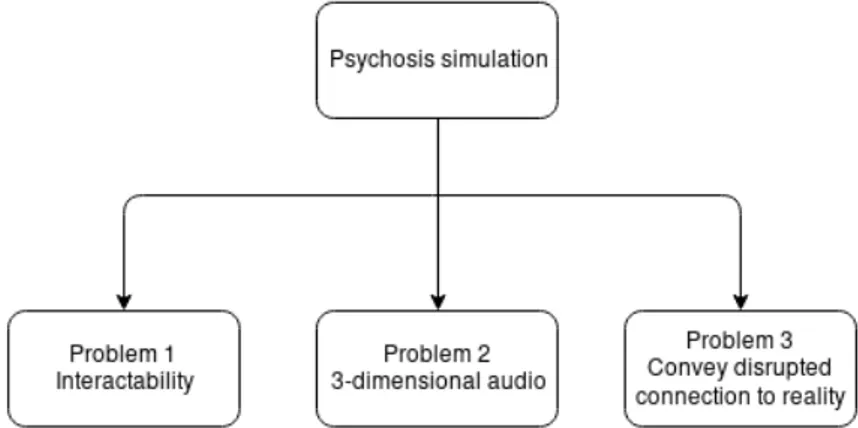
From these requirements a subset of problems emerge. In order to promote understanding and ease the visualization of these problems a problem tree is constructed.
Figure 2: Problem breakdown visualization
5.1.3 Problem breakdown
As shown in Figure 2 the main problem is broken down into a subset of problems consisting of three distinct problems. These sub problems do how ever need further explanation and clarification in order to be defined within the context of this thesis.
Problem 1
Just as the word suggest, interactability is the ability to interact with something. The definition of interactability in the context of this thesis is the users ability to interact with objects within the VR simulation. The interaction with objects is constrained to key objects only. Key objects include alarm clock, medication container, radio, phone, key and door. This constraint is needed in order to keep the user progressing forward in the simulation and to limit the potential distractions.
Problem 2
In order to simulate auditory hallucinations as well as the sounds of radios and alarm clocks, the audio must be perceived to function as close as possible to peoples normal perception of audio. That implies that the audio in the prototype must respect spatial changes. This means that the audio shall be perceived as further away should the user move away from it. It also means that when the user turns their head away from the audio source, it shall act accordingly. Meaning that the volume shall decrease in the ear that is the furthest away from the source while remaining unchanged in the ear closest to the source.
Problem 3
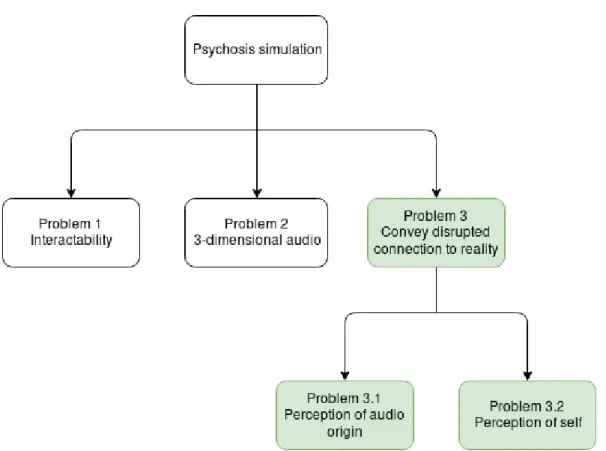
One of the characteristic symptoms of psychosis is delusion and a lost or weakened con-nection to reality. The question of what is real lies outside the scope for this thesis and is therefore simplified into two distinctive problems. See Figure 3.
Figure 3: Furthered problem breakdown
Problem 3.1
Perception of audio origin relates to the users perception of an arbitrary sound source. The user should be uncertain of whether a sound is coming from some tangible object within the simulation or if it is a product of the characters psyche.
Problem 3.2
Perception of self relates to how the user perceives of themselves within the context of the simulation. In order to strengthen the delusional trait of psychosis the user should be uncertain of their state in the reality depicted in the simulation.
5.2 System architecture
The system architecture is the composition of the system. It describes the relationship between the modules included in the system, their functionality and the motivation behind each module.
When developing in Unity3D, a script is attached to game objects in order to instill a certain behaviour in that object. From the developers perspective the main execution loop of the program is to be considered a black box. This meaning that the developer does not need insight in the chronology of the execution in the main loop. The scripts attached to the various game objects is therefore executed as callbacks inside the main
loop. The main loop is also considered to be the sole producer of the system’s global state.
In a system with many intractable objects, all of which has their own state, state manage-ment can become cumbersome. This due to the risk of objects not adhering to the global state or transitioning into illegal states. This risk will be referred to as state fragmenta-tion.
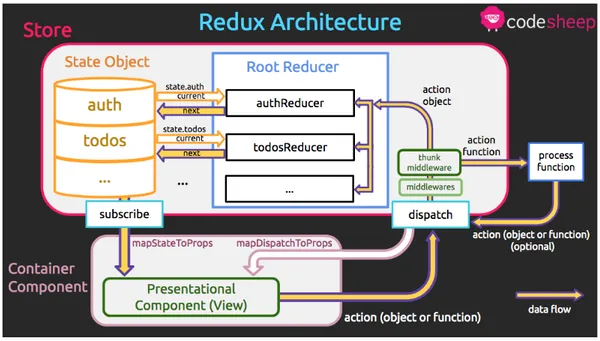
To prevent state fragmentation and to keep side effects from events to a minimum, the prototype makes use of an architectural pattern based on Redux11. As shown in Figure 4.
Figure 4: Diagram of redux data flow12
5.3 System design
The prototype involves two designs, the purely technical design as well as the scenario design. The scenario design relates to what tasks the user is supposed to complete and the means by which the user can complete said tasks.
5.3.1 Technical design
Hardware and software platform
The design of the prototype is constrained by what software and hardware was provided
11
https://github.com/reactjs/redux/tree/master/docs
by Jayway. Due to the project being requested by Jayway, the HMD and game engine was chosen prior to the project’s start. Jayway requested that the prototype were to be built for HTC Vive Pro using Unity3D. Should this request never have occurred, would Unreal engine13in combination with Oculus Rift14also have been considered for the design.
5.3.2 State management
By default, Unity3D proposes an architecture, in which every object within the system gets a script bound to it. These scripts in turn consists of a new C# class derived from the predefined class MonoBehaviour. By convention, the developer then have the option of overriding the Start and Update methods derived from the parent class. Every instruction in the Start method will be executed during the initialization of the object itself. This means that every time such an object is instantiated, the provided override of Start is run. The Update method will in turn be executed every iteration of the game loop. This means that it will execute for every new frame produced by the engine.
The conventional way of implementing object behaviour in Unity3D forces a state frag-mentation since every object will be responsible for updating its own state in accordance with the system’s global state. In order for objects to act in reaction to other objects in the scene, the observer pattern[14, p.488] will have to be implemented. The observer pattern demands explicit registration of observers in order to let said observers react upon the object that it observes. When an observer is notified of a state change or event in the observed object, a reaction occurs in the form of a function call from the observer. In order to promote easily extendable and easy to read code, the design pattern chosen for the prototype is UniDux. UniDux is a pattern utilizing unidirectional data flow. UniDux15 is an adaptation of redux, spefically for Unity3D.
5.3.3 Audio
ResonanceAudio for Unity3D from Google was used to implement the audio features of the prototype. ResonanceAudio offers ways to implement and customize 3D spatial audio in term of reverb and audio occlusion.
13
https://www.unrealengine.com/en-US/what-is-unreal-engine-4
14https://www.oculus.com/ 15
5.3.4 Scenario design
Figure 5: Scenario structure
As shown in Figure 5 the scenario is constructed from a linear story progression. The user starts in the bedroom where an alarm clock has gone off. They proceed to turn the alarm clock off. Auditory hallucinations in the form of voices, speaking to the user, and strange noises such as knocks and laughter will appear seemingly random throughout the entire scenario. The auditory hallucinations starts as soon as the simulation starts.
Once the alarm has been shut off, the user will proceed into the bathroom in order to ingest the medication. The medication container is placed on the sink. Once the user lifts up the container the label will change into a warning label, saying that the content is poisonous. During the time the user takes the medication voices will appear to come from inside the characters head. These voices will then continue throughout the entire simulation.
After ingesting the medication, the participant heads for the kitchen in order to prepare breakfast. The phone disturbs the participant when preparing the breakfast. When the participant answers the phone, there is no one on the other side and the participant is met with a dial up tone. Shortly after the phone event, the voices starts to raise a concern
for the characters family. The voices warns the participant that their family is in grave danger and make comments about it being the participants fault, placing the blame for the non existing accident on the participant.
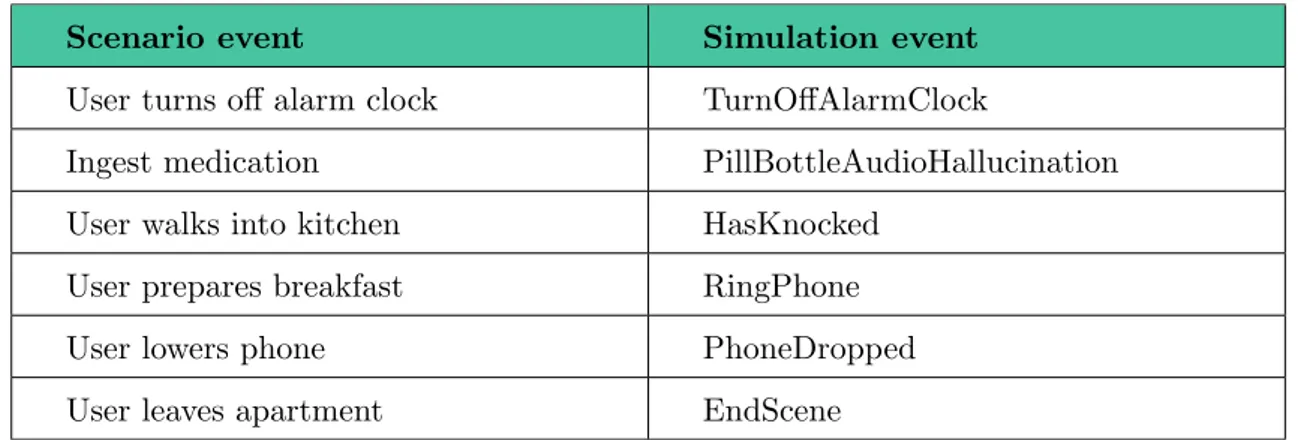
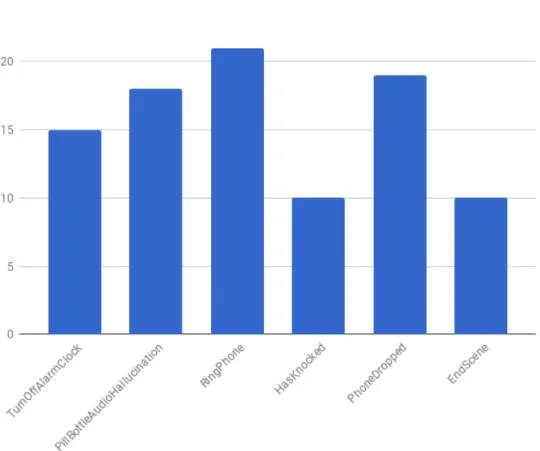
Scenario event Simulation event User turns off alarm clock TurnOffAlarmClock
Ingest medication PillBottleAudioHallucination User walks into kitchen HasKnocked
User prepares breakfast RingPhone User lowers phone PhoneDropped User leaves apartment EndScene
Table 1: Eventmappings
As shown in Table 1, each event in the scenario design corresponds to a matching event in the simulation. The simulation events shown in table 1 are those that impacts the participant directly. They are all need to be triggered at least once in order for the simulation to be considered complete.
6
Implementation
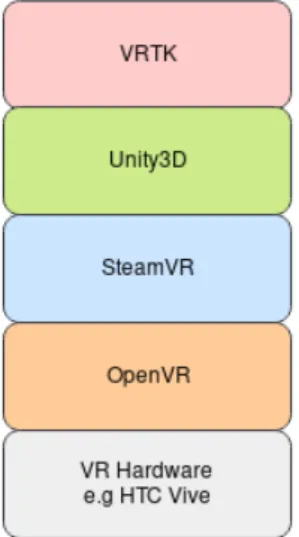
This chapter describes which technologies was used to implement the prototype and ex-plains the motivation for using them. VR consists of a technology stack as shown in Figure 6. This chapter aims to describe each layer of this thechnology stack.
Figure 6: Diagram illustrating the relationship between the VR technologies
6.1 VRTK
VRTK is an open source library that solves the problem of interfacing the HTC Vive HMD programmatically. VRTK provides the developer with a wide range of functionality such as user input detection, user position, locomotion alternatives and more.
It is possible to develop for the HTC Vive using nothing but Unity3D’s standard library. This would take a long time since the developer would have to write all the code to manage the HMD and interface SteamVR.
6.1.1 Unity3D
When implementing an interactive, three dimensional software lot of computations is needed. It is supposed to react on user input and render graphics in what is perceived as real time a. These computations may for example involve the graphics rendering, listening for user input and the physics calculations. There are pre-built software that solves the problem of all the aforementioned calculations. Such software is referred to as a game engine.
Unity3D handles the physics, graphic rendering and also the main execution loop. Unity3D then provides the developer with and API to which the developer then makes calls through
the scripts created.
One of main reasons to use Unity3D for the development of the prototype is Unity’s support for VR development. This support is made clear by the availability of VR development libraries for Unity3D.
6.1.2 Steam VR
Unity3D interconnects with SteamVR, which is a middleware that lies between the appli-cation and OpenVR16. Devices being the HTC Vive HMD and the controllers.
6.2 Resonance Audio
ResonanceAudio is a spatial audio framework develop by Google. The purpose of Reso-nanceAudio is to enable developers to implement audio that respects it’s environment. In the context of games and VR, having audio that respect it’s environment means that the audio gets affected by the materials it travels trough. It respects positioning and angle of the player. Effectively the audio will be dampened if traveling through a wall. When the player turns their head, the audio will phase over from one ear to the other. Making audio behave in such a way is referred to as spatializing the audio. The dampening as it travels through different materials is referred to as audio occlusion.
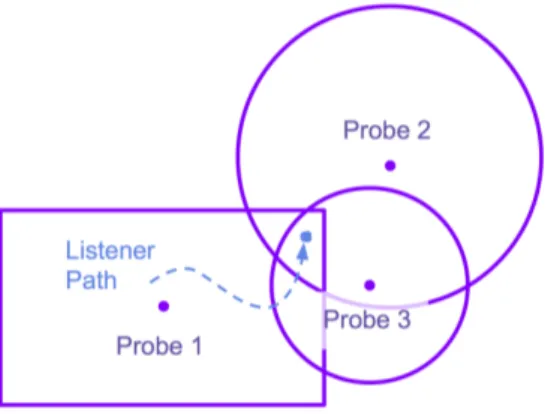
Resonance audio presents four core building blocks. These are audio listeners, audio sources, audio rooms and reverb probes. Audio sources provides a point from which the sound is emitted. The audio then travels outwards from the source and gets registered at every audio listener it hits. In order to simulate acoustics the audio room component is placed in the system. The audio room component provides a room consisting of four walls, a floor and a ceiling, all of which can have a material assigned to them. These materials have different acoustic profiles and will shape the sound reflected off them in different ways. The reverb probe provides the developer with a way to tie the audio rooms together. If two audio rooms where to be placed next to each other, and the player went from one room to the other the gap in between the rooms would have a different acoustic profile than the rooms themselves. This means that the audio do not transition between the rooms in a natural, authentic way. Instead, a reverb probe is placed in between the two audio rooms, tying them together. The transition can be configured in such a way that the audio keeps a realistic acoustic profile. An example use case for audio probes in conjuction with audio rooms can be seen in Figure 7.
16
Figure 7: Illustration of audio room (rectangle) in relation to audio probe (circle)
The implementation of the prototype utilizes two of the core components from Reso-nanceAudio i.e. audio sources and audio listeners. The audio listeners are used as audio mixers for the audio sources provided by Unity.
7
Results and discussion
The tests were all performed using an HTC Vive pro, HTC Vive controllers and executed on a desktop computer running Windows 10.
Prior to the actual tests a pilot test was carried out in order to determine the amount of time needed for the tests. During the pilot test the instructions for the participants was also established.
7.1 Participants
Ten participants were recruited among Jayway’s employee staff. The criterion that they were chosen on was that they could not have any history of psychotic episodes or illnesses prior to the test. Prior to the test all participants were questioned on their experience with VR. All the participants had tried VR at least once and the most experienced participant was a VR developer, which utilize VR-headsets on a near daily basis.
7.2 Survey design
The surveys is based on a study performed by Angermeyer and Dietriech[1]. The study concluded that a large portion of the population think of psychotic individuals as un-predictable, violent and/or dangerous. Within this study it is also presented that those holding these aforementioned beliefs are more likely to seek out a greater social distance. They are also more likely to be in favour of forced treatment for those suffering from schizophrenia and/or psychosis. The surveys aims to ask questions in accordance to these beliefs, investigating these aspects of the attitudes and beliefs held towards those suffer-ing from psychosis. The survey was filled out by the participants before and after the simulation in order to show the potential impact on attitude by the simulation.
As mentioned in the method chapter the surveys are designed using the Likert scale. In practice this means that each question consists of a statement and the four alternatives Strongly disagree, Disagree, Agree and Strongly agree. By using this design the results attempts to reflect to what degree the participants hold the belief stated in the ques-tion.
7.3 Procedure
The design of the test allows for collection data to answer RQ1 and RQ2. The results of the forms make out the basis on which RQ2 will be answered and the automated logs make out the basis on which RQ1 is answered.
form. In the second stage the participant partake in the simulation and in the third and last stage the participant fills out the last form. Only one participant is involved in a test at each time and have a set time frame of 30 minutes to complete all three stages. The first stage begins with the instructor asking the participant about their experience with VR and whether or not they have suffered from psychotic illnesses in the past. The test instructor then asks the participant to fill out the first form. During the time the participant fills out the form, the instructor leaves the room. The instructor leaves the room in order to prevent any linking between a specific form and a participant. All in order to retain anonymity. Once the form is filled out, the participant calls for the instructors attention and the instructor re-enters the room and initiates the second stage of the test.
Figure 8: Simulation test demonstrated by Jayway employee
Before the participant can start the simulation, the instructor explains the controller mapping and the ways of movement in the simulation to the participant. The instructor also explains in what order the rooms should be visited in the simulation. The participant equips the VR-headset, as shown in Figure 8 and the instructor stays in the room in order to answer questions and to take note of how many times he needs to help the participant progress in the simulation. During the test, each action triggered by the participant in the simulation is logged to a file.
instructor once again asks the participant to fill out a form and leaves the room. Once the form is filled out the participant informs the instructor and the test is over.
7.4 Results
7.4.1 Simulation
During the simulation the instructor observed the participant in order to track the amount of times the participant asked for help.The instructor also observed whether the participant needed any intervention in order to complete the test within the given time frame. All of the participants finished all of the three stages within the time frame without any intervention from the instructor. None of the participants asked for help or clarification at any point during the simulation.
Figure 9: Amount of actions triggered during all tests
7.4.2 Attitudes
The results will be presented by the mean of each question. Calculated by assigning each al-ternative a weight corresponding to it’s index e.g. Strongly disagree = 1 and Strongly agree = 4. Then multiplying each of these weights with the number of participants choosing that alternative, summing up the results and dividing it by the number of participants:
P4
i=1
i·x
n
where n is the number of participants.
This means that the closer the score is to 1 the more the group of participants disagree with the proposed statement, and the closer the score gets to 4 the more they disagree. A summary of the mean scores can be seen in Table 2.
Statement Pre simulation Post simulation
Q1 2.4 3 Q2 1.8 2.6 Q3 1.2 2.8 Q4 2.5 2.2 Q5 3 3.2 Q6 2.7 3.3 Q7 2.9 3.2
Table 2: Survey results mean
On the last statement (Q8) ”My understanding of people suffering from psychosis has increased after partaking in the simulation” nine out of ten participants answered ”Yes”. The alternatives for the statement was ”Yes” and ”No”.
The surveys can be seen in their entirety in A.1 along with graphs showing the results in A.2.
7.5 Discussion
All participants did trigger all of the crucial events at least once. This means that they all experienced a full simulation including every phase of the scenario. The participants all managed to trigger every event without any intervention by the test instructor. The events was triggered as a direct consequence of the participants behaviour and decisions during the simulation. This in combination with the events being triggered correspondingly to the
scenario design suggests that the simulation was constructed in a successful manner. In contrast, the worst of simulations would not have had the participants trigger any events. During the tests, the simulation did not showcase any bugs or unintended behaviours. Due to the utilization of the Redux pattern, state changes and triggered events could be logged to file in a quantifiable manner. Showing the state changes in chronological order with high granularity indicating that no state fragmentation occurred and that the state changes happened in accordance to the scenario design.
Angermeyer and Dietriech[1] concludes that a large portion of the general population hold negative attitudes and beliefs towards mental illnesses, schizophrenia and psychosis in particular. In this thesis we aimed to investigate whether these attitudes and beliefs could be affected using VR technology and in what ways they would be affected. The results shown in Table 2 suggests a shift in attitude. The actual result lies in contrast with the expected result. The initial hypothesis was that the participants would disagree with the statement to a higher degree post simulation. We initially thought that the participants would be inclined to side with the character in the simulation. Leading to them seeing the statements post simulation as more aggressive and thereby taking a stronger stance against them. The shift in attitude shown in Table 2 and the increased understanding suggested by the answers to Q8, rather indicates the opposite, the participants being inclined to agree with the statements to a greater extent. This could also suggest that VR has the potential to affect peoples attitudes when used for simulations. Due to the number of participants being relatively small, consisting of only ten participants, the results are to be viewed as indications and not as evidence.
8
Conclusions and future work
One of the great challenges when implementing a simulation in VR is to guide the user through the experience. Due to the open and free nature of VR applications the user may choose to stray from the intended path or to interact with the environment in unforeseen ways. This in itself presents a challenge of presenting narratives and guidance that will not intervene with the experience. It also presents the risk of the user triggering events in an order that is not prepared for. With these challenges in mind this thesis asks the question of how to build a simulation using VR. One answer to that question is presented within this thesis. The combination of every participant triggering every action in the correct order and that the prototype do not present any bugs due to unintended interaction, shows that the design and implementation present in this thesis is one way of building such a simulation.
The results from the surveys show a change in attitude towards people suffering from psychosis. The greatest of which being a change of 1.6 units on a scale of 4. This change indicates that VR as a medium holds potential to affect peoples opinions and perceptions of a subject. The question presented in this thesis read ”In what way can a VR-simulation simulating the symptoms of psychosis affect non-psychotics attitude towards those experi-encing psychosis?”. What the results indicates on this matter is that the participants took a firmer stance towards people suffering from psychosis after going through the simulation. Had the number of participants been bigger so would the resulting data set. This would have made it possible to analyze potentially finer nuances in attitude changes as well. The results should therefore be interpreted as an indication of VR’s potential to affect the user is contexts like the one presented here, rather than this specific simulation inducing permanent change in the participants attitudes. If this study where to be repeated in collaboration with a psychiatric professional, that professional could have validated the prototype. A validation of the prototype combined with a greater data set would have had the potential to investigate RQ2 further and with higher precision.
8.1 Future work
This thesis has presented the possibility of using VR as a medium for simulations and a tool to place people in situations that might otherwise be unlikely to experience. Future work might consist of establishing a methodology and framework for the development of such simulations in order to attain maximum authenticity. The scenario implemented in the simulation used during the work with this thesis was based solely on the literature regarding psychosis. It was also purposely designed in a general manner not focusing on one particular case of psychosis. With the help of professionals in the subject area future work could consist of developing more specific simulations producing results of higher precision. For any future attempts on measuring shifts in attitudes after a simulation like the one in this thesis a much larger group of participants are needed. In a group of ten (as in this thesis) one participants shift in attitude has to great of an impact on the overall result. If a bigger group is utilized the impact of one participant will be smaller and the
A
Appendix
A.1 Surveys
The pre simulation and post simulation surveys are the same with the exception of an additional statement in the post simulation survey.
Statement Strongly disagree
Disagree Agree Strongly agree I think people with psy-chosis should be forced to partake in treatment I think people with psy-chosis should be institu-tionalized I think psychosis makes people more likely to commit acts of violence I think people with psy-chosis are dangerous towards other people Table 3: Survey
Statement Strongly disagree
Disagree Agree Strongly agree I think people with psy-chosis are dangerous towards them-selves I think people with psy-chosis hear voices that aren’t really there I think people with psy-chosis see things that aren’t really there
Table 4: Survey - continuation
Statement Yes No
My understanding of people suffer-ing from psychosis has increased after partaking in the simulation
References
[1] M. C. Angermeyer and S. Dietrich. Public beliefs about and attitudes towards people with mental illness: a review of population studies. Acta Psychiatrica Scandinavica, 113(3):163–179, 2006.
[2] Jasmine Banks, Geoffery Ericksson, Kevin Burrage, Peter Yellowlees, Sean Ivermee, and Jennifer Tichon. Constructing the hallucinations of psychosis in virtual reality. Journal of Network and Computer Applications, 27(1):1 – 11, 2004.
[3] Jasmine Banks, Geoffery Ericksson, Kevin Burrage, Peter Yellowlees, Sean Ivermee, and Jennifer Tichon. Constructing the hallucinations of psychosis in virtual reality. Journal of Network and Computer Applications, 27(1):1 – 11, 2004.
[4] Seth A. Brown. Implementing a brief hallucination simulation as a mental illness stigma reduction strategy. Community Mental Health Journal, 46(5):500–504, Oct 2010.
[5] Adolfo J. Cangas, Noelia Navarro, Jos´e M. A. Parra, Juan J. Ojeda, Diego Cangas, Jose A. Piedra, and Jose Gallego. Stigma-stop: A serious game against the stigma toward mental health in educational settings. Frontiers in Psychology, 8:1385, 2017. [6] A Cook. Undestanding psychosis and schizophrenia. British Psychological Society,
2014.
[7] Nicholas J. Formosa, Ben W. Morrison, Geoffrey Hill, and Daniel Stone. Testing the efficacy of a virtual reality-based simulation in enhancing users’ knowledge, attitudes, and empathy relating to psychosis. Australian Journal of Psychology, 70(1):57–65. [8] Daniel Freeman. Studying and treating schizophrenia using virtual reality: A new
paradigm. Schizophrenia Bulletin, 34(4):605–610, 2008.
[9] Kjell Lindstr¨om H˚akan Jarbin and Mussie Msghina. L¨akemedelsboken. L¨ akemedelsver-ket, 2017.
[10] E.M. Kolasinski, U.S. Army Research Institute for the Behavioral, and Social Sci-ences. Simulator sickness in virtual environments. Number v. 4, nr. 1027 in Technical report (U.S. Army Research Institute for the Behavioral and Social Sci-ences). U.S. Army Research Institute for the Behavioral and Social Sciences, 1995. [11] R. Likert. A technique for the measurement of attitudes. Archives of Psychology, 22
140:55–55, 1932.
[12] Jay F Nunamaker Jr, Minder Chen, and Titus DM Purdin. Systems development in information systems research. Journal of management information systems, 7(3):89– 106, 1990.
[13] G. M. Rodriguez, M. Cruz, A. Solis, P. Ord´o˜nez, and B. C. McCann. An immersive approach to visualizing perceptual disturbances. In 2017 IEEE Virtual Reality (VR), pages 291–292, March 2017.
[14] R. Farmer S. Bennet, S. McRobb. Object-oriented systems analysis and design using UML. Number v. 4. McGraw-Hill International (U.K) Limited, 2010.
[15] Sriram ”Sri Kalyanaraman, David L. Penn, James D. Ivory, and Abigail Judge. The virtual doppelganger: Effects of a virtual reality simulator on perceptions of schizophrenia. The Journal of Nervous and Mental Disease, 198(6), 2010.
[16] Jennifer Tichon, Jennifer Loh, and Robert King. Psychology student opinion of virtual reality as a tool to educate about schizophrenia. International Journal on E-Learning, 3(4):40 – 46, 2004.
[17] Lucia R. Valmaggia, Fern Day, and Mar Rus-Calafell. Using virtual reality to inves-tigate psychological processes and mechanisms associated with the onset and mainte-nance of psychosis: a systematic review. Social Psychiatry and Psychiatric Epidemi-ology, 51(7):921–936, Jul 2016.
[18] Peter M. Yellowlees and James N. Cook. Education about hallucinations using an internet virtual reality system: A qualitative survey. Academic Psychiatry, 30(6):534– 539, Nov 2006.
![Figure 1: Workflow as suggested by Nunamaker[12]](https://thumb-eu.123doks.com/thumbv2/5dokorg/4159583.89711/12.892.389.504.585.900/figure-workflow-as-suggested-by-nunamaker.webp)