ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
jo u r n al ho me p a g e :w w w . c a s e r e p o r t s . c o m
Case
Series
Left
iliac
fossa
mini-incision
sigmoidectomy
for
treatment
of
sigmoid
volvulus.
Case
series
of
six
patients
from
Qatar
Mahmood
Al
Dhaheri
a,
Mohamed
Abu
Nada
a,
Walid
El
Ansari
b,c,d,∗,
Mohamed
Kurer
a,
Ayman
Abdelhafiz
Ahmed
aaDepartmentofColorectalSurgery,HamadGeneralHospital,HamadMedicalCorporation,Doha,Qatar bDepartmentofSurgery,HamadGeneralHospital,HamadMedicalCorporation,Doha,Qatar cCollegeofMedicine,QatarUniversity,Doha,Qatar
dSchoolofHealthandEducation,UniversityofSkovde,Skovde,Sweden
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received14August2020
Receivedinrevisedform3September2020 Accepted3September2020
Availableonline8September2020 Keywords: Volvulus Sigmoidectomy Mini-incision Laparotomy
a
b
s
t
r
a
c
t
BACKGROUND:Midlinelaparotomyisthedefinitivetreatmentforsigmoidvolvulusafterinitial colono-scopicdetorsion.Wesuccessfullyadoptedanothertechniqueatourcenteron6patients,treatingsigmoid volvulusbyleftiliacfossamini-incision.
PRESENTATIONOFCASES:Wereportourexperienceofsixnon-consecutivecasesofsigmoidvolvulus treatedbyleftiliacfossamini-incision.Thecaseswerea33yearoldEgyptianfemale,a21yearold Bangladeshimale,a58yearoldQatarimale,a30yearoldEthiopianmale,a36yearoldUgandanmale, anda58yearoldIndianmale.Thesixcasesareuniqueinthesurgicaltechniqueemployedintheir management.Thisispossiblythesecondcaseseriesofleftiliacfossamini-incisionforsigmoidvolvulus intheMiddleEastandNorthAfricaRegion.
DISCUSSION:Allpatientsunderwentinitialcolonoscopicdetorsionfollowedbysigmoidectomyand anas-tomosis.Theprocedurewassuccessfulintreatingthevolvulusinfivepatientswithnocomplication orrecurrenceoverameanfollowupof8months(range:1–36months).Onepatientrequiredfurther laparotomyandresectionwithanastomosisduetoincompletelyremovedsigmoidcolon.
CONCLUSIONS:Leftiliacfossamini-incisionforsigmoidvolvulusissafe,feasible,cosmeticallyappealing andwithlowmorbidity.
©2020TheAuthors.PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Background
Sigmoidvolvulusisthemostcommonformofvolvulus, repre-senting3%–5%ofallacuteintestinalobstructions[1].Itoccurswhen aredundantlongsigmoidcolontwistsaroundanelongated nar-rowmesentery.Thereisdebateastowhethersigmoidvolvulusis congenital,acquired,oracombinationofboth[2].However,a high-fiberdiet, advancedage,chronicconstipation,previoussurgery, neurologicorpsychiatricconditionsandmegacolonhaveallbeen identifiedaspredisposingfactors[2–4].
Most(85%)colonicvolvuluspresentasanacuteobstruction[5], withabouthalfthepatientsreportingasimilarepisodeinthepast [6].Afterinitialcolonoscopicdetorsion,midlinelaparotomywith sigmoidectomyandprimaryanastomosisisthestandarddefinitive management[1].Recently,thelaparoscopicapproachemergedasa
∗ Correspondingauthorat:DepartmentofSurgery,HamadGeneralHospital, HamadMedicalCorporation,Doha,Qatar.
E-mailaddress:welansari9@gmail.com(W.ElAnsari).
minimallyinvasiveoption.However,ithasitstechnicallimitations duetothedistendedbowel,intoleranceofpneumoperitoneumin comorbidpatients,increasedcosts,anditisnotreadilyavailable, particularlyinlowerincomecountries[7].Inordertoaidthe reduc-tionofmorbidity,aleftiliacfossamini-incisionwasfirstdescribed in2014[8],associatedwithsignificantcostsaving,cosmetically appealingscar,potentiallyimprovedrecoveryandlesspain.We adoptedthismini-incisiontechniqueatourhospitalin2016,and sincethenwehaveoperatedon6casesofsigmoidvolvulusata singlecolorectalsurgerycenter.
Wereportthesesixretrospectivenon-consecutivecasesata singlecentreduetotheuniquenessofthemini-incisionsurgical technique and itsfindings, and in orderto debatethepossible advantagesofthistechnique.Thiscaseseriesisinlinewiththe updatedconsensus-basedcaseseries(PROCESS)guidelines[9].
2. Casepresentations
Table1depictsthesummaryofcharacteristicsofthesixpatents. https://doi.org/10.1016/j.ijscr.2020.09.014
2210-2612/©2020TheAuthors.PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Table1
Summaryofcharacteristicsofthesixpatients.
Characteristic Case1 Case2 Case3 Case4 Case5 Case6
Demographics
Age(years) 33 21 58 30 36 58
Gender Female Male Male Male Male Male
BMI(kg/m2) 24.9 21.32 23.35 22.15 23.54 28.67
Country Egypt Bangladesh Qatar Ethiopia Uganda India
Presentation Elective,3months
postdelivery
Emergency Emergency Emergency Emergency Emergency
History
Comorbidities Nil Nil Epilepsy,mental
retardation,cataract, hypertension, dyslipidemia
Nil Nil Hypertension
Previoussurgery 3cesareansections Nil Nil Nil Nil Nil
Previous episode/recurrent abdominalpain Recurrent abdominalpain Volvulus5months earlier
Nil Nil Nil Volvulus7months
earlier Pre-operative Allpatientshadsuccessfulcolonoscopicdetorsionanddecompressionwithrectaltubeinsertion
CTfindings Notdone Whirlpoolsign Whirlpoolsign Whirlpoolsign Whirlpoolsign Whirlpoolsign
Operative
Procedure Leftiliacfossamini-incisionandsigmoidectomywastechnicallyfeasibleinallpatients
Operativetime(min) 120 90 160 90 90 100
Bloodloss(ml) 20 30 50 20 30 20
Lengthofhospitalstay (days)
4 4 4 4 5 5
Post-operative
Complication/s Nil Nil Persistentvolvulus* Nil Nil Nil
Mortality Nomortalityacrossallpatients,withmeanfollowupof8±SD27months(range:1–36months)
*Persistentvolvulus(after5days,duringsameadmission)duetoincompleteremovaloftheredundantsigmoidcolon.
2.1. Case1
A33yearoldEgyptianfemalewhowas33weekspregnant, pre-sentedtotheemergencydepartmentatourinstitution(Hamad General Hospital, largest tertiary care hospital in Qatar) with abdominal pain,constipation and abdominal distention 2 days. Past history was remarkable for recurrent abdominal pain for around5yearsandpreviouscesareansections.Norelevant fam-ilyhistory.Uponexamination,shewashemodynamicallystable, withdistendedabdomen. Bloodinvestigations were unremark-able. AbdominalX-ray showed severelydilated colon withthe coffeebeansignofsigmoidvolvulus.Shewasadmitted, success-fullyunderwentsigmoidoscopy,detorsionanddecompressionand was discharged home after 3 days. Then, after delivery of the child,shestartedhavingintermittentabdominalpainagain,and3 monthsfollowingthefirstattack,shewasadmittedelectivelyand underwentleftiliacfossamini-incisionsigmoidectomyandwas dischargedonpost-operativeday5.Atonemonthfollowupafter theprocedure,therewerenopost-operativecomplicationsnoted.
2.2. Case2
Apreviouslyhealthy21yearoldBangladeshimalepresentedto theemergencydepartmentatourinstitutionwithabdominalpain fortwodaysassociatedwithconstipationandvomiting.Past his-toryrevealedthathehadanattackofsigmoidvolvulus5months priortothispresentation.Nopasthistoryofsurgery,andno rele-vantfamilyhistory.Uponexamination,hewashemodynamically stable,withdistendedabdomenbutnonperitonitic.Blood inves-tigations were unremarkable. Preoperative CT of the abdomen showeddilatedcolon withthewhirlpool sign, features impres-siveofsigmoidvolvulus.Heunderwentsigmoidoscopy,detorsion anddecompressionwithrectaltube.Onday5postdetorsion,he underwentsigmoidectomyvialeftiliacfossamini-incisionandwas dischargedonpost-operativeday5.Therewerenopost-operative complicationsuponfollowupto36months.
2.3. Case3
A 58 yearold Qatarimale living ina residential homewith medicalhistoryofmentalretardation,cataract,hypertension, dys-lipidemia,andepilepsycontrolledbymedication.Thepatienthad pasthistory ofchronic constipationwhich wasusuallyrelieved by rectal enema. History taken from the accompanying nurse indicatedthathehadconstipationandprogressiveabdominal dis-tentionfor three days.Over the2 days prior tothe admission toourhospital,thepatienthadbecomeirritableand uncooper-ative, andthis wasattributed tohisabdominalpain. Hisblood investigationswereunremarkable.PreoperativeCToftheabdomen showeddilatedcolonwithtwistedmesenteryandthewhirlpool sign,featuresremarkableofsigmoidvolvulus.Heunderwent sig-moidoscopy,detorsionanddecompressionwithrectaltube.Eight days postdetorsion, heunderwent sigmoidectomy vialeft iliac fossa mini-incision. Post operatively, although he did not pass motionsorflatus,hewasstartedonsurgicalfluid,afterwhichhe developedgradualabdominaldistentionoverpostoperativedays 3 and4.Hence apostoperativeCT oftheabdomenwas under-taken and again showed features of sigmoid volvulus. A rectal tube wasinsertedand the distention partiallyimproved. How-ever,heagaindevelopeddistensionandconstipationforwhichhe underwentexploratorymidlinelaparotomyonpost-operativeday 5.Intraoperatively,therewasdilatedcolondistal tothe anasto-moticsite,withabanddiscoveredextendingfromleftcolontothe smallbowelmesenteryaroundwhichtheremainingsigmoidwas twisted.Thisbandwasdivided,andsigmoidectomyofthe remain-ingsigmoidandprimaryanastomosisweredone.Thepatienthad asmoothpost-operativecoursewithopenbowelandwasstarted onregulardietonpost-operativeday4.Onfollowup,hewaswell until29monthspost-surgery,afterwhichhepresentedagainwith abdominaldistensionandconstipationbutpassingflatus.CTofthe abdomenshoweddilatedcolonandsmallintestinewithtransient pointat theanastomoticsite.Heunderwentcolonoscopy anda stricturewasfoundattheanastomoticsitewhichwastreated endo-scopicallywithserialCRETMBalloondilatationinthreeintervalsup
to16.5cm.Onfollowup,todate,hewaswellandpassingmotion onbulklaxativeintermittently.
2.4. Case4
A30yearoldEthiopianmalewithnomedicalillnesspresented toouremergencydepartmentwithcolickyabdominalpain and constipationfor3days.Nopasthistoryofsurgery,andnorelevant familyhistory.Uponexamination,hewashemodynamicallystable withdistendedabdomen.Bloodinvestigationswereunremarkable. PreoperativeCToftheabdomenshoweddistensionofcolonwith thewhirlpoolsign, featuresremarkableof sigmoidvolvulus. On thesamedayheunderwentsigmoidoscopy,detorsionand decom-pressionwithrectaltube.Onday3postdetorsion,heunderwent sigmoidectomyvialeftiliacfossamini-incisionandwasdischarged onpost-operativeday4.Atonemonthfollowup,therewereno post-operativecomplications.
2.5. Case5
A36yearoldUgandanmalepresentedtoouremergency depart-mentwith colickyabdominal pain for onedayassociated with vomitingandpassageofloosemotionsfor3days.Nohistoryof medicalillnessorprevioussurgery,andnorelevantfamilyhistory. Uponexamination,hewashemodynamicallystablewithdistended abdomen.Bloodinvestigationswereunremarkable.Preoperative CT of theabdomenshowed twisting of thesigmoidaround its mesenterywith the whirlpool sign, and a massivelydistended proximalcolonwithanair-fluidlevel.Onthesameday,he under-went sigmoidoscopy, detorsion and decompression with rectal tube.Onday5postdetorsionheunderwentsigmoidectomyvia leftiliacfossamini-incision andwasdischarged onpost opera-tiveday5.Attwomonthsfollowup,therewerenopost-operative complications.
2.6. Case6
A58yearoldIndian malewithpresentedtoouremergency departmentwithabdominalpainandabdominaldistentionthat developedgraduallyoverthepastweek.Hehadhistoryofsigmoid volvulus7monthspriortothispresentation,medicalhistory of hypertensioncontrolledwithmedication,andnorelevantfamily history.Uponexamination,hewashemodynamicallystablewith distendedabdomen.Bloodinvestigationswereunremarkable. Pre-operativeCToftheabdomenshowedtwistingofthevesselsand mesenteryofthesigmoidcolon,consistentwithwhirlpoolsign.On thesameday,heunderwentsigmoidoscopy,detorsionand decom-pressionwithrectaltube.Onday5postdetorsion,heunderwent sigmoidectomyvialeftiliacfossamini-incisionandwasdischarged onpost-operativeday5.Atsevenmonthsfollowup,therewereno post-operativecomplications.
3. Surgicaltechnique:leftiliacfossamini-incision sigmoidectomy
Afterinitialcolonoscopic detorsionand decompressionwith insertionofrectaltube,patientswererestartedonoralfluids.Once patientscantolerateoralfluids,allpatientsshouldhavemechanical bowelpreparationandfullcolonoscopytocheckforany pathol-ogy.Onceconfirmationisavailablethatthereisnopathologyin thecolonotherthanthevolvulus,leftiliacfossamini-incision sig-moidectomyandprimaryanastomosisisundertakenlater.
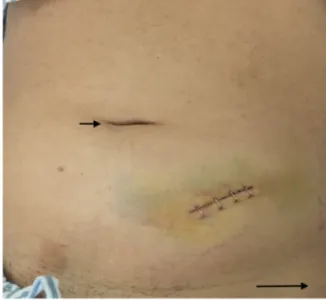
Theprocedureswereperformedbyconsultantswithexperience incolorectalsurgeryofatleast5years.Undergeneralanesthesia, thepatientinsupineposition,aleftiliacfossaskinincisionofabout 5cmwasundertaken(mirrorimageofMcBurneyincision)(Fig.1).
Fig.1.Leftiliacfossamini-incisiononpostoperativeday4(Shortarrow:umbilicus, Longarrowleftanteriorsuperioriliacspine).
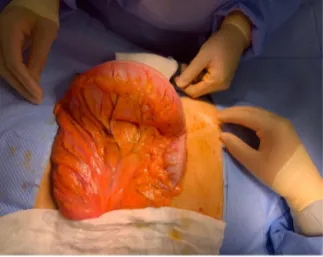
Fig.2.Exteriorizationofthesigmoidcolonshowingthemini-incisioninleftiliac fossa.
Theexternalobliqueaponeurosiswasdividedalongitsfibersand themuscleswereseparated.Theperitoneumwascarefullyopened withscissors.Thedilatedredundantcolonwasexteriorizedand carefullyinspectedforviability(Fig.2).Acriticalstepwastoensure theretrievalofthewholeredundantcolonproximallyanddistally untiltherectosigmoidjunction,inordernottoleaveanyredundant colonicsegmentwhichcouldlaterpredisposetorecurrenceofthe volvulus(Fig.3).Oncethesigmoidwasexteriorized,the mesen-terywasthendividedinaVshapemanner,andcolonicresection oftheredundantsigmoidcolonwasundertakenleavingawell vas-cularizedproximaland distalpartofthecolonforanastomosis. Re-establishmentoftheintestinalcontinuitywasdonebysideto sideanastomosisusingGIAlinearstapler80[8].
4. Discussion
The initial assessment of sigmoid volvulus comprises an appraisal of signs of perforation, gangrene or peritonitis. For patientswithsignsofperforationorgangrene,animmediate mid-linelaparotomyshouldbeperformed[10]. Forpatientswithout
Fig.3.Exteriorizationofthewholeredundantsigmoidcolon.
peritonitis,primarytherapyiscolonoscopicdetorsionusinga flex-ibleendoscope,wheresuccessfuldetorsionisachievedin upto 80–90%ofcases[4,6],andmaintainedwiththeinsertionofa rec-taltubeand concomitantresuscitationof thepatient.Detorsion anddecompressionaloneisfrequentlyfollowed bya significant recurrencerate[4,10].Hence,definitiveearlysurgeryshouldbe performed.
Definitivesurgicalmanagementofpatientswithout peritoni-tisfollowingsuccessfulendoscopicdecompressioniscontroversial. Theclassicaldefinitivesurgicalapproachhasbeenmidline laparo-tomy and sigmoid colectomy with primary anastomosis [10]. But such approach has the disadvantage of colonic resection andpossibleanastomoticleakage.Hence,non-resectionalsurgical approaches,aimedatdecreasingsuchmorbidity havealsobeen described. These include open, laparoscopicor endoscopic sig-moidopexy, as wellas extraperitonealizationof the sigmoidor meso-sigmoidoplasty[11–14].Thesethreealternativeshavebeen usedwithvariablesuccesses,butsuchapproacheshaveamajor drawbackintermsofhigherrecurrencerateofthevolvulus[15].To date,nolargerandomizedcontrolledtrialshavebeenconductedto comparetheeffectivenessofsigmoidcolectomywithprimary anas-tomosisvssigmoidopexy,extraperitonealizationofthesigmoidor meso-sigmoidoplasty.
Thelaparoscopicapproachhasbeenincreasinglydescribedfor sigmoidvolvulusandisgenerallyassociatedwithimproved mor-bidity[16–19].However,someauthorsclaimthatlaparoscopyfor sigmoidvolvulusisunwarrantedasitistechnicallydifficultand toocostly[7,18].Inordertosimplifythetechnicaldifficultiesof laparoscopiccolectomyinsigmoidvolvulus,itwasproposedthat laparoscopybeusedonly tohelpexteriorize thesigmoidcolon throughamini-incisionwithoutpreliminarydissection[17].
However,inourexperience,weobservedthatthereisnoneed foreitheralongincisionorlaparoscopy,asinpatientswith volvu-lus,thesigmoidcolonisquitelong,redundantandrathereasily broughtoutoftheabdominalcavity.Hence,weagreewithothers [8]thatleftiliacfossamini-incisionwithoutlaparoscopyis suffi-cient.Inourinitialexperiencewithsixpatientsduringthepast 2.5years,theprocedurewasstraightforward,andtechnicallyless challengingthan thelaparoscopicapproach. In agreement, oth-ershavesupportedthatthatleftiliacfossamini-incisionwithout laparoscopyhasexcellentresultsand couldalsobeundertaken underlocalanesthesia[8,20,21].Furthermore,intherareeventof failedexteriorization(e.g.,inobesepatients)ofwhichwedidnot encounterany,theprocedurecouldbeconvertedtotheopenor laparoscopicapproach.
Oursixpatientswhounderwentleftiliacfossamini-incision sigmoidectomyandprimaryanastomosisfortreatmentofsigmoid volvuluswereallsatisfiedandpleasedwiththesmallincisionthat wascosmeticallyappealing.Fromthesurgeons’ side,there was minimalblood loss,decreasedlengthofhospital stayand post-operativeanalgesiawhichminimizedthecosts.Weobservedno complicationswiththismini-incision surgicalapproach, in con-trasttomidlinelaparotomywhichgenerallycarriesa10–30%risk ofincisionalherniaasalatecomplication[22–26].
Oneofourpatients(Case3)hadtobere-operated4daysafter theindexprocedurebyamidlinelaparotomy,duepersistenceof thevolvulusbecausetheredundantsigmoidcolonwasnot com-pletelyresected.Here,wehighlightthecriticalstepofretrieving thewholeredundantproximalanddistalcolon.Thisisanimportant pointinthelearningcurveoftheprocedure.
5. Conclusion
In this case series, we highlightsigmoidectomy for sigmoid volvulusbyleftiliacfossamini-incisionasapossiblealternative totheclassicalmidlinelaparotomy.Itissafe,feasible,cost effec-tive,haslowmorbidity,andcosmeticallyappealing.Althoughthe majorityofourpatientswereyoung,sigmoidectomyforsigmoid volvulusbyleftiliacfossamini-incisioncouldbeevenmore advan-tageousforolderpatientswithmultiplemorbiditiesasitcanbe undertakenunderlocalanesthesia.Weencouragethepracticeof suchtechnique,howeverthereisaneedforheadtoheadrigorous comparisonswithmidlinelaparotomyandlaparoscopy.
DeclarationofCompetingInterest
Theauthorsreportnodeclarationsofinterest. Funding
Nothingtodeclare. Ethicalapproval
ApprovedbyMedicalResearchCenter,HamadMedical Corpo-rationreferencenumber(MRC-01-20-086).
Consent
Itwasnotpossibletoobtainwritteninformedconsentfromthe patients.Mostpatientsprobablytravelledoutofthecountryafter surgery.Theheadofoursurgicalteamhastakenresponsibilitythat exhaustiveattemptshavebeenmadetocontactthepatientsortheir familiesandthatthepaperhasbeensufficientlyanonymizednot tocauseharmtothepatientsortheirfamilies.Acopyofasigned documentstatingthisisavailableforreviewbytheEditor-in-Chief ofthisjournalonrequest.
Authorcontribution
MahmoodAlDhaheri:Conceptualization,Datacuration, Inves-tigation,Projectadministration,Writing-originaldraft,Writing -review&editing.MohamedAbuNada:Datacuration, Investiga-tion,Methodology,Writing-review&editing.WalidElAnsari:Data curation,Methodology,Writing-originaldraft,Writing-review& editing.MohamedKurer:Datacuration,Investigation, Methodol-ogy,Writing-review&editing.AymanAbdelhafiz:Datacuration, Methodology,Validation,Writing-originaldraft,Writing-review &editing,Writing-review&editing.Allauthorsreadandapproved thefinalmanuscript.
Registrationofresearchstudies researchregistry5909.
https://www.researchregistry.com/register-now#home/ registrationdetails/5f36449b945da30018d17556/.
Guarantor
ProfDrWalidElAnsari. Provenanceandpeerreview
Notcommissioned,externallypeer-reviewed. Acknowledgement
Theauthorswishtoacknowledgethepatientsincludedinthis report.
References
[1]A.K.W.Ifversen,D.W.Kjaer,Morepatientsshouldundergosurgeryafter sigmoidvolvulus,WorldJ.Gastroenterol.20(48)(2014)18384–18389. [2]H.J.Asbun,H.Castellanos,B.Balderrama,etal.,Sigmoidvolvulusinthehigh
altitudeoftheAndes.Reviewof230cases,Dis.ColonRectum35(1992) 350–353.
[3]M.D.Hellinger,R.M.Steinhagen,ColonicVolvulus,1sted.,Springer,NewYork, 2009,pp.286–298.
[4]A.Sadatomo,Y.Miyakura,T.Zuiki,etal.,Sigmoidvolvulusafterlaparoscopic surgeryforsigmoidcoloncancer,AsianJ.Endosc.Surg.6(2013)217–219. [5]G.H.Ballantyne,M.D.Brandner,R.W.Beart,D.M.Ilstrup,Volvulusofthecolon.
Incidenceandmortality,Ann.Surg.202(1985)83–92.
[6]Z.Lou,E.D.Yu,W.Zhang,R.G.Meng,L.Q.Hao,C.G.Fu,Appropriatetreatment ofacutesigmoidvolvulusintheemergencysetting,WorldJ.Gastroenterol.19 (2013)4979–4983.
[7]S.B.Osiro,D.Cunningham,M.M.Shoja,R.S.Tubbs,J.Gielecki,M.Loukas,The twistedcolon:areviewofsigmoidvolvulus,Am.Surg.78(2012)271–279. [8]I.Seow-En,F.Seow-Choen,Sigmoidvolvulustreatedbymini-incision,Tech.
Coloproctol.18(12)(2014)1169–1171.
[9]R.A.Agha,M.R.Borrelli,R.Farwana,K.Koshy,A.Fowler,D.P.Orgill,Forthe PROCESSGroup,ThePROCESS2018statement:updatingconsensusPreferred
ReportingofCaseSeriesinSurgery(PROCESS)Guidelines,Int.J.Surg.60 (2018)279–282.
[10]D.Gingold,Z.Murrell,Managementofcolonicvolvulus,Clin.ColonRectal Surg.25(2012)236–244.
[11]D.Choi,R.Carter,Endoscopicsigmoidopexy:asaferwaytotreatsigmoid volvulus?J.R.Coll.Surg.Edinb.43(1998)64.
[12]B.N.Bhatnagar,C.L.Sharma,Nonresectivealternativeforthecureof nongangrenoussigmoidvolvulus,Dis.ColonRectum41(1998)381–388. [13]R.Miller,A.M.Roe,W.K.Eltringham,H.J.Espiner,Laparoscopicfixationof
sigmoidvolvulus,Br.J.Surg.79(1992)435.
[14]Y.Akgun,Mesosigmoplastyasadefinitiveoperationintreatmentofacute sigmoidvolvulus,Dis.ColonRectum39(1996)579–581.
[15]M.Bagarani,A.S.Conde,R.Longo,A.Italiano,A.Terenzi,G.Venuto,Sigmoid volvulusinWestAfrica:aprospectivestudyonsurgicaltreatments,Dis.Colon Rectum36(1993)186–190.
[16]J.A.Sundin,D.Wasson,M.M.McMillen,G.H.Ballantyne,Laparoscopic-assisted sigmoidcolectomyforsigmoidvolvulus,Surg.Laparosc.Endosc.2(1992) 353–358.
[17]C.C.Chung,S.P.Kwok,K.L.Leung,K.H.Kwong,W.Y.Lau,A.K.Li,
Laparoscopy-assistedsigmoidcolectomyforvolvulus,Surg.Laparosc.Endosc. 7(1997)423–425.
[18]J.T.Liang,H.S.Lai,P.H.Lee,Electivelaparoscopicallyassistedsigmoidectomy forthesigmoidvolvulus,Surg.Endosc.20(2006)1772–1773.
[19]T.Cartwright-Terry,S.Phillips,G.L.Greenslade,A.R.Dixon,Laparoscopyinthe managementofclosedloopsigmoidvolvulus,ColorectalDis.10(2008) 370–372.
[20]A.Tavassoli,G.Maddah,S.Noorshafiee,M.Salehi,S.Imannezhad,E. Ghorbanian,Anovelapproachtominimallyinvasivemanagementofsigmoid volvulus,ActaMed.Iran.54(10)(2016)640–643.
[21]E.L.Enrique,K.A.Hamdy,Minilaparotomywithoutgeneralanesthesiaforthe treatmentofsigmoidvolvulusinhigh-riskpatients:acaseseriesof4patients, Int.J.Surg.CaseRep.34(2017)23–26.
[22]D.Millbourn,Y.Cengiz,L.A.Israelsson,Effectofstitchlengthonwound complicationsafterclosureofmidlineincisions:arandomizedcontrolled trial,Arch.Surg.144(11)(2009)1056–1059.
[23]C.M.Seiler,T.Bruckner,M.K.Diener,A.Papyan,H.Golcher,C.Seidlmayer, etal.,Interruptedorcontinuousslowlyabsorbablesuturesforclosureof primaryelectivemidlineabdominalincisions:amulticenterrandomizedtrial, Ann.Surg.249(4)(2009)576–582.
[24]J.B.Trimbos,I.B.Smit,J.P.Holm,J.Hermans,Arandomizedclinicaltrial comparingtwomethodsoffasciaclosurefollowingmidlinelaparotomy,Arch. Surg.127(10)(1992)1232–1234.
[25]R.E.Brolin,Prospective,randomizedevaluationofmidlinefascialclosurein gastricbariatricoperations,Am.J.Surg.172(4)(1996)328–331.
[26]M.Colombo,A.Maggioni,G.Parma,S.Scalambrino,R.Milani,Arandomized comparisonofcontinuousversusinterruptedmassclosureofmidline incisionsinpatientswithgynecologiccancer,Obstet.Gynecol.89(5Pt1) (1997)684–689.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.