Master thesis in Criminology Malmö University Criminology Master’s Programme Health and Society
120 credits 205 06 Malmö
May 2018
THE RELATIONSHIP BETWEEN ONLINE
GAMBLING, PSYCHOSOCIAL
PROBLEMS AND CRIME FOR
HELP-SEEKERS CALLING A HELPLINE
DIFFERENCES BETWEEN GAMBLERS AND RELATIVES
OVER AN EIGHT-YEAR PERIOD
2
THE RELATIONSHIP BETWEEN ONLINE
GAMBLING, PSYCHOSOCIAL
PROBLEMS AND CRIME FOR
HELP-SEEKERS CALLING A HELPLINE
DIFFERENCES BETWEEN GAMBLERS AND RELATIVES
OVER AN EIGHT-YEAR PERIOD
ERIK ROSENBERG
Rosenberg, EDifferences between gamblers and relatives calling a helpline. Examining online gambling, crime, and psychosocial problems.
Masters thesis in criminology, 30 points.
Malmö University: Faculty of Health and Society, Department of Criminology, 2018.
Abstract
Problem gambling is a public health issue that affects gamblers, relatives and society in general. The Swedish National Gambling Helpline, Stödlinjen, operates as a primary help to people with problems related to gambling. The 22,260 calls made to the helpline from 2009 to 2016 were studied with regards to gender, age, online gambling, psychosocial problems, and crime. Comparison between gamblers and relatives revealed gender and age differences. Reports of online gambling increased for both groups as time progressed, while crime declined. The results are discussed, and it is concluded that more research on the connection between gambling and crime is needed, as well as further develop a crime-aspect in the counsellors’ documentation of helpline callers.
Keywords: Crime, gambling, helpline, online gambling, problem gambling,
3
TABLE OF CONTENTS
INTRODUCTION ... 4
Gambling ... 4
Why people gamble and why some gamble excessively ... 4
Game types ... 5
Prevalence ... 5
Demographics ... 6
Gambling and crime ... 6
Addiction ... 7 Problem gambling ... 7 Treatment ... 7 Helpline ... 8 Stödlinjen ... 9 Objective ... 9 Method ... 9 Variables ... 10 Limitations of data ... 11 Statistics ... 11 Ethics ... 12 Results ... 12
Differences between gamblers and relatives ... 13
Variations between different years ... 14
Differences between years for gamblers ... 14
Differences between years for relatives ... 16
Associations of factors ... 16 Online gambling ... 16 Financial problem ... 17 Health problem ... 17 Social problem ... 17 Crime ... 17 Discussion ... 18 Conclusion ... 20 References ... 21 Appendices ... 26 Appendix 1 ... 26 Appendix 2 ... 27
Psychosocial problems recoding ... 27
4
INTRODUCTION
Most people gamble as a leisure activity (PHAS 2016). For those that gamble excessively, gambling can lead to adverse financial, health, and social problems, and in some cases even illegal behaviour. The negative effects of gambling can also affect relatives, leading to financial, health, and social problems of their own. Some relatives get victimised by the gambler through steeling (Meyer & Stadler 1999) or physical and psychological abuse (Roberts, Landon, Sharman, Hakes, Suomi & Cowlishaw 2017). For gamblers entrenched in debt, surrounded by triggers, and filled with feelings of shame, the only answer is to continue gambling. Fortunately, help can be found by calling Stödlinjen, the Swedish National Gambling Helpline. For those that do reach out and seek help it has, in Sweden, become easier lately due to changes in clinical assessments (DSM-V1)
and legal changes governing social services (The Social Services Act 2001:453 SoL2) and healthcare (The Health and Medical Services Act 2017:30 HSL3) However, online gambling poses a challenge due to the availability and solitary nature (Abbott, Binde, Clark, Hodgins, Korn, Pereira, Quilty, Thomas, Volberg, Walker & Willams 2015) of the platform. Because problem gambling is
considered a public health issue affecting individuals, their relatives and society in general, research has been conducted from the Public Health Agency of Sweden4
(PHAS) but no research in Sweden has focused on problem gambling and crime. With the increase in number of gambling ads and online casinos, and young members of society being a vulnerable group in the beginning of their working careers, this is a topic that requires attention.
Gambling
Gambling is when two or more parties wager value on an uncertain outcome in order to gain greater value (PHAS 2016). This is a broad definition and can be applied to many things that people do not necessarily associate with gambling. For the intents and purposes of this paper gambling refers to the game types listed below. Even though there might be value wagering in computer games; gaming in the sense of computer games, video games, and TCG:s (trading card games) are excluded from the definition.
Why people gamble and why some gamble excessively
For the most part gambling is seen as an entertainment. Binde (2013) suggest that there are five motives for (leisure) gambling 1) the dream of hitting the jackpot, 2) social rewards, 3) intellectual challenge, 4) mood change, and 5) the chance of winning. The fifth motive is essential, while the others compliment or vary depending on the individual and the game. (ibid).
Blaszczynski and Nower (2002) propose a framework including an integrated model consistent of ecological factors, classical and operand conditioning, habituation and chasing leading to problem or pathological gambling. They also propose that while some start to gamble for entertainment or socialization, others
1 Diagnostic and Statistical Manual of mental disorders - fifth edition. 2 SoL – Socialtjänstlagen
3 HSL – Hälso och sjukvårdslagen
5
gamble to avoid negative affects by means of escape or temporary arousal. For both, ecological factors (availability and accessibility) like legislation or
technological advancements (online casinos in one’s phone) play an instrumental part in exposure to gambling. Classical and operant conditioning refers to the cognitive learning processes where something is seen as good by positive or negative reinforcement (operant) and triggers reminding the individual of that good thing creates an urge to pursue (classical). Following more frequent gambling is the process of habituation which further fortifies faulty beliefs in personal skill, biased evaluation of probability outcomes or superstitious thinking. With the inevitable losses, chasing occurs where the individual tries to win back losses which ultimately increases the negative spiral of gambling leading to problem or pathological gambling (Blaszcynski & Nower 2002).
Game types
There are many different ways to gamble but focusing on the commercial
gambling market in Sweden, a rough categorisation can be made to slot machines, casino games, poker, sport, and number games.
The focus of this paper is online gambling, which is not a game type but a platform for gambling. Previous research has to some extent tried and categorise game types as strategic versus non-strategic (Challet-Bouju, Hardouin, Renard, Lagauffre, Valleur, Magalon, Fatséas, Chéreau-Boudet, Gorsane, Vénisse & Grall-Bronnec 2014), or fast versus slow (Harris & Griffiths 2018). With the increase of online casinos offering a wide variety of games this matters less. A slow game like live poker can now be played fast by digital timers or by playing multiple cash games and tournaments at once. The problem with dichotomising games into strategic or non-strategic is that poker and sport betting consist of a combination of strategy and probability, and it is quite possible for someone to play poker or make bets on sporting events completely without any strategy. Furthermore, some gamblers believe there is strategy involved in games like black jack or roulette due to misconceptions, which then raises the question of what is being measured.
Online gambling offers new challenges due to its availability and accessibility, solitary nature, and lack of regulation. Gambling is for the most part in Sweden provided by the government. International online casino sites placed abroad (e.g. Malta) is not only available for Swedes but also to an extent marketed towards Swedes. Advertising for online casinos are highly regulated in Sweden; this is bypassed by having TV-channels located abroad (e.g. Great Britain) being allowed to advertise gambling and then broadcasting to Sweden.
Prevalence
Measuring worldwide prevalence of problem gambling can be difficult because of different methodologies, definitions of problem gambling, and legal and cultural contexts. With that in mind, Calado and Griffiths (2016) conducted a systematic review on worldwide prevalence of problem gambling between 2000 and 2015 and found a past-year rate of between 0.12% and 5.8%. In Europe the prevalence of problem gambling varied between 0.12% and 3.4%, of which it was most prevalent in Switzerland (the German and French speaking part) (Calado & Griffiths 2016).
6
Approximately 2% of the Swedish population are problem gamblers, of which 0.4% could be diagnosed as having a gambling disorder (pathological gambling). Another 5% of the population are at risk of developing problem gambling. Each year three quarters of the problem gamblers gets replaced by ‘new’ problem gamblers, of which 20% have been problem gamblers before. This means that approximately 450,000 people in Sweden are struggling with gambling in differing degrees each year, and another 260,000 relatives, of which 76,000 are children, are in close proximity to the problems of gambling (PHAS 2016).
Demographics
Generally speaking, problem gamblers is not a homogenous group (Blaszczynski & Nower 2002), people in various demographical groups can become a problem gambler. There are however some variations in demographics as shown by
SWELOGS5. Men gamble more than women, (73% of males compared to 67% of females gambled in the last 12 months). Approximately 73% of problem gamblers are male and the problems are most severe for 18-24-year olds where one in ten males are a problem gambler. People with higher education tend to have less gambling problems, and problem gamblers tend to have lower income (lowest quartile of income) (PHAS 2016).
Gambling and crime
The highest rate of problem gamblers was found in forensic populations ( May-Chahal, Humphreys, Clifton, Francis & Reith 2016). A literature review from Williams, Royston and Hagen (2005) revealed that one third of the forensic population met criteria for problem or pathological gambling, of which half state they committed crime to support their gambling.
Another systematic review and meta-analysis of 14 studies from Australia, Canada, New Zealand, Spain and USA by Dowling, Suomi, Jackson, Lavis, Patford, Cockman, Thomas, Bellringer, Koziol-Mclain, Battersby, Harvey & Abbott (2016a) found a significant relationship between problem gambling and intimate partner violence (IPV). The relationship was more consistent between problem gambling and IPV perpetration than IVP victimization. A national study in the USA by Roberts and colleagues (2017) found that problem gambling was associated with increased odds ratio (OR) of physical IPV perpetration for both men and women while increased levels of victimization was only found in female respondents. The authors suggest that IPV might be a consequence of problem gambling, but gambling could also be used as a coping mechanism to escape negative emotional states (especially for women) (ibid). Muelleman, DenOtter, Wadman, Tran & Anderson (2002) interviewed women in the hospital emergency department and found that women with a partner with a drinking problem (OR: 6.1), gambling problem (OR: 10.5) or both (OR: 50) were more likely to have suffered from IPV.
A comparative study in Germany by Meyer and Stadler (1999) found that gamblers show a high intensity of criminal behaviour, and in cases where
gambling addiction led to property crimes the treatment of pathological gambling
7
reduced the risk for relapse to crime. Comorbidity and co-occurring issues seem to follow problem gambling (Arthur, Williams & Belanger 2014; Dowling, Merkouris & Lorains 2016b), but even if the causal directionality is not proven it does show that problem gambling is part of a multifaceted situation for those involved.
Addiction
Addiction can be divided into two major categories, substance addiction and behavioural addiction (Ascher & Levounis 2015; Orford 2001). As of DSM-V gambling addiction is categorised under SAD (Substance-related and Addictive Disorders) (Fauth-Bühler, Mann & Potenza 2017) due to the many similarities concerning phenomenology, neurobiological mechanisms, overlapping genetic contribution, comorbidity, tolerance and response to treatment (Grant, Potenza, Weinstein & Gorelick 2010). It is also renamed gambling disorder and the criteria ‘illegal acts’ has been removed (Petry, Blanco, Stinchfield & Volberg 2012; Rennert, Denis, Peer, Lynch, Gelernter & Kranzler 2015). The World Health Organisation have yet to make this inclusion in ICD-106 but some researchers and clinicians are pushing for this to change in the upcoming ICD-11 as it did for DSM-V (Fauth-Bühler et al. 2017).
Even though there is an ongoing debate whether addiction is a brain disease or not (Leshner 1997; Nutt 2013; Lewis 2015; Satel & Lilienfeld 2016), and there is inconsistency in the usage of the word ‘addiction’ as opposed to ‘dependence’ (Altman, Everitt, Glautier, Markou, Nutt, Oretti, Phillips & Robbins 1997), most agree that the dopamine reward system in the brain is central to developing an addiction (Koob & Le Moal 1997; Lewis 2015). There is also a common
agreement that the biopsychosocial approach explains the aetiology of addictive behaviour (Williams, West & Simpson 2007).
Problem gambling
Problem gambling is sometimes used interchangeably with pathological gambling, and yet there is an important difference, the former refers to a
behaviour (gambling) that leads to problems and the latter refers to a compulsion to gamble (Blaszcynski & Lower 2002). Problem gambling is therefore to a degree subjective; the same amount of money lost affects people differently (ibid). For the intents and purposes of this paper problem gambling is defined as
‘gambling that leads to financial, health, social and legal problems’. Similar definitions can be found in previous research (Blaszcynski & Lower 2002; PHAS 2016; Wardell, Quilty, Hendershot & Bagby 2015).
Treatment
An individual suffering from problem gambling can make an appointment at any psychiatric or health care centre. The treatments differ depending on which organisation the individual turns to; the standard treatment in the governmental health care system is CBT (cognitive-behavioural therapy). A systematic review and meta-analysis of CBT interventions was conducted by Gooding and Tarrier (2009) showing a highly significant effect in reducing gambling behaviour. While
8
CBT is an effective method it might be necessary to treat multiple disorders due to psychiatric comorbidity like alcohol and substance use disorder, mood disorder, anxiety disorder, and ADHD7 (Dowling, Cowlishaw, Jackson, Merkouris, Francis & Christensen 2015; Dowling et al. 2016b; Håkansson, Mårdhed & Zaar 2017). Despite available treatments few problem and pathological gamblers seek help due to shame, denial, issues with treatment, and wanting to handle it themselves (Suurvali, Cordingley, Hodgins & Cunningham 2009).
Helpline
Helplines are organisations that try to help people over the phone that are
experiencing crisis. The appeal is that nationwide help can be provided so long as there is a counsellor available. There are many types of helplines specialised at specific problems or crisis. Helplines for problem gambling have been shown to be an effective way of promoting treatment for problem gamblers that would not otherwise seek professional help (Bastiani, Fea, Potente, Luppi, Lucchini & Molinaro 2015; Ledgerwood, Arfken, Wiedemann, Bates, Holmes & Jones 2013). According to Valdivia-Salas, Blanchard, Lombas and Wulfert (2014) gambling helplines should be seen as a resource in the prevention process and development of knowledge. Research on gambling helplines show that financial problems and previous gambling-related treatment predict seeking help (Ledgerwood et al. 2013; Pulford, Bellringer, Abbott, Clarke, Hodgins & Williams 2009a). Barriers to seeking help are similar to those found in Suurvali and colleagues’ (2009) literature review: shame, pride, denial, and wanting to handle it themselves (Hing, Tiyce, Holdsworth & Nuske 2013; Pulford, Bellringer, Abbott, Clarke, Hodgins & Williams 2009b; Rodda, Hing & Lubman 2014), and Gainsbury, Hing and
Suhonen (2013) found that awareness of treatment services is relatively low.
More men than women call a helpline for their problem gambling (Griffiths, Scarfe & Bellringer 1999; Potenza, Steinberg, McLaughlin, Wu, Rounsaville & O’Malley 2001), while more women than men call a helpline as a relative or significant other to a problem gambler (Hing et al. 2013). This is consistent with the annual report of 2016 from Stödlinjen (79% male gamblers calling)
(Stödlinjen 2016). Women calling a gambling helpline appear to experience greater gambling disorder severity and more psychosocial problems related to their gambling (Ledgerwood, Wiedemann, Moore & Arfken 2012; Kim, Hodgins, Bellringer & Abbott 2016). Slot machines (EGM:s, VTL:s, fruit machines) seem to be the most prominent problem game for helpline callers, especially for adolescents, women and older adults (Griffiths et al. 1999; Kim et al. 2016; Potenza, Steinberg, Wu, Rounsaville & O’Malley 2006; Potenza et al. 2001).
Comorbidity of gambling helpline callers was most prominently substance use, suicidality, anxiety, and depression (Glenn, Diaz & Moore 2006; Ledgerwood, Steinberg, Wu & Potenza 2005; Sinclair, Pretorius & Stein 2014; Potenza et al. 2006; Potenza et al. 2001). Hawley, Glenn and Diaz (2007) found that 70% of callers to the gambling helpline were employed at the time of the call and 28% were 18-35-year olds, suggesting that employers might be an untapped resource for helping problem gamblers.
9 Stödlinjen
The Swedish National Gambling Helpline, Stödlinjen, was established in 1999 and in 2011 the operation transferred to a state capacity at the Centre for Psychiatry Research, part of the Stockholm County Council and Karolinska Institutet (KI), under the aegis of the PHAS. Since autumn of 2015 Stödlinjen is run on behalf of the Swedish Ministry of Health and Social Affairs as one of several preventive efforts. The primary focus of Stödlinjen is to provide support and information to people with gambling problems and relatives seeking help and information. Stödlinjen also acts as a source of information to the public regarding problem gambling related questions. The counsellors at Stödlinjen are trained professionals using Motivational Interviewing (MI) and Cognitive-Behavioural Therapy (CBT) as a first response to problems the caller highlights in the conversation. The counsellors are available via telephone, chat and e-mail, weekdays between 9 am and 9 pm. As a secondary focus, counsellors take notes during the calls which is put together in a data base for research purposes
(Stödlinjen 2016). Even though Stödlinjen is primarily focused on gambling they get many calls about playing computer and video games which in of itself can be detrimental for the individual’s health and work/studies but is only a risk factor for problem gambling to a certain degree (Delfabbro, King, Lambos & Puglies 2009).
Objective
In a material collected by counsellors at the Swedish National Gambling Helpline from 2009 to 2016 that includes information given by help-seeking gamblers and relatives during these calls, study the relationship between online gambling, psychosocial problems, and crime.
Specific aims
Concerning gender and age; proportion of help-seekers referring to online gambling as primary platform of problem gambling; proportion of help-seekers reporting negative financial, health, and social consequences of gambling; and proportion of help-seekers that have reported crime perpetration or victimisation:
- study differences between gamblers and relatives.
- study variations between different years for gamblers and relatives respectively.
- study which factors are associated with online gambling, financial, health, and social problems, and crime for gamblers and relatives respectively.
METHOD
The helpline documented information from each call from December 2008 to December 2016 (2008 was excluded, see appendix 1) in cooperation with PHAS. Counsellors made notes of demographics, game type and psychosocial problems related to gambling. The caller steered the conversation which means that the documented information is primarily of what the caller highlighted. Counsellors have to some extent been apart of the call, and also made interpretations and
10
categorisations of what has been said. The documentation was put together into a data base with variables similar to that of SWELOGS (PHAS 2016).
The study was initiated through a contact between the author and the helpline project manager. Before receiving the full data set an agreement was made stipulating that the data could only be used for the current thesis. The full data set was received in an unprocessed form. The following steps have been taken to establish a processable data file: (1) conversion of excel-file to SPSS-file and assignment of values, (2) identification, categorisation, and exclusion of non-gambling related calls, and (3) identification and categorisation of whether the call was made by a gambler or relative (see appendix 1 for in-depth process).
Variables
To study differences between years, nine variables were created, one ordinal 1-8 and eight dummy variables coded ‘1’ for the year in question and ‘0’ for all the other years. This way it is possible to study overall directionality of change but also which years that were significantly more different in regard to the specific aims.
Gender and age of the caller were used as demographic variables. Because the aim of the study was to study differences in and between help-seekers (i.e. those that call the helpline), gender and age of the player precipitating relatives to call the helpline was not used.
Age was dichotomised as young (34 and younger) and not young (35 and older). The original age variable had an uneven distance between categories and
counsellors did not always get a specific age from the caller. A cut-off point of 35 years has been used in previous research (Hawley et al. 2007) and seemed
reasonable for a binary variable.
Which particular game played (e.g. poker, EGM:s) was not measured. Instead, the platform of gambling was used because of the availability and accessibility, lack of formal regulation, solitary nature and harmful effects of online gambling (Binde 2011).
A comparison of help-seekers (gamblers and relatives) concerning psychosocial problems was done by dichotomising whether or not any financial, health, and/or social problems were highlighted during the call. Only the negative effects of problem gambling were included, which means that a caller stating their finances are good have been group together with ‘no response’. The specifics of each psychosocial aspect differ to an extent between gamblers and relatives which is why the results of inter-group analysis should be interpreted with this in mind.
Crime variables differ from gamblers and relatives. Information about gamblers’ crime perpetration was only found as financial crime such as theft, fraud and embezzlement. For relatives, however, they reported having had money or
valuables stolen, as well as physical and psychological abuse. This lead to having gamblers’ crime variable as perpetration, and relatives’ crime variable as
victimisation.
11 Help-seeker: Gamblers and relatives
Year: 8 years in total (2009 – 2016) and dummy variables for each year. Demographics: Gender (male - female), age (34 and younger - 35 and older). Type of gambling: Online – Offline
Psychosocial problems: Financial, Health, and Social.
Crime: Gambler calling, any perpetration. Relative calling, any victimization.
Limitations of data
Without a variable specifically stating that the caller was a gambler or relative, and because counsellors had input data in both ‘variable blocks’ it is not certain that the dichotomisation of help-seekers is accurate. It is also recognised that by using variables to distinguish gamblers from relatives calling, means that the variables with the highest response rate have a greater correlation, for instance gender and help-seeker. Therefore, the results of inter-group analysis (gambler compared to relative) should be interpreted with this in mind.
Combining callers’ ‘positive’ responses (e.g. good mental health, good finances, no debt) with no response or missing values is cutting away an interesting
dimension of gambling-related problems. If a caller says he/she has good finances but also suicidal tendencies, that could be quite interesting to explore deeper. Future research might want to look into such complexities but for this paper the objective is differences between negative effects of gambling.
It is recognised that the helpline for gambling is not primarily a research study on the association between gambling and crime. It is also recognised that the helpline operates under PHAS and therefore takes a public health perspective on gambling. Crime might therefore be underreported.
Statistics
The data is in the form of frequencies that are presented along with percentages. Chi-square test for independence was used to study the first and second aim. Using Yates’ correction for continuity in 2 by 2 tables allow for more accurate results (Pallant 2010) and phi presents effect size using Cohen’s criteria of .10 = small, .30 = medium, .50 = large (ibid). The third specific aim was studied by running binary logistic regressions, presenting odds ratio, 95% confidence interval and significance at less than .05.
Chi-square test for independence was used for:
- comparing gamblers to relatives concerning gender, age, online gambling, financial, health, social, and crime.
- comparing different years, gamblers and relatives separately concerning gender, age, online gambling, financial, health, social, and crime. Five binary logistic regressions were run for gamblers and relatives separately with year, gender, and age recurring independent variables while gambling, financial, health, social, and crime alternated as dependent and independent variables to assess associations.
12 Ethics
Anyone calling the helpline can do so with total anonymity. Information about the person, as stated in The Data Protection Act (1998:204 PUL8), was not registered by the counsellors. All analyses were done on aggregate group level. Consent was neither ask for, explicitly given, nor needed due to the anonymity, absence of personal information, and the level of analysis. The data did, however, contain information about crime and health issues which are considered ethically sensitive data. The Ethical Review Act9 concerning research involving humans (2003:460)
sate in 2 § that research done in the context of higher education is not governed by this law. Malmö University does, however, state that students within the Faculty of Health and Society that conduct research with ethically sensitive data must apply for ethical approval at the university’s ethics council (mah.se/etikprovning). Before processing the data, an application was made to Malmö University’s ethics council who had no objection to the study being conducted. The decision from the ethics council, reference number 2018/17, is attached to the present thesis
(appendix 3).
The data set was retrieved from the project manager of Stödlinjen by means of box.com, an encrypted data sharing site. The processing and data analysis have been done from a stationary password protected computer and the data has been stored securely and will be deleted after the thesis has been completed.
RESULTS
Between 2009 and 2016 the helpline received 22,260 calls. Of these, 13,574 (61%) were gambling related calls. The total frequency of calls in relation to frequency of gambling related calls are shown by year in figure 1. Of the gambling related calls, 10,816 (80%) were made by help-seekers calling for counselling. The help-seekers consist of 6110 (56.5%) gamblers and 4706
(43.5%) relatives. The frequency of help-seeking relatives in relation to frequency of gamblers calling the helpline are presented by year in figure 2. There is a slight downward trend in frequency both in total and by gambling related calls (figure 1). The trend of number of gamblers calling seem to be relatively stable while the trend of relatives calling seem to be slightly increasing (figure 2).
8 PUL – Personuppgiftslagen
9 Svensk författningssamling 2003:460, Lag om etikprövning av forskning som avser
13
Figure 1. Diagram depicting number of calls in total and number of
gambling-related calls made to the helpline from 2009 to 2016.
Figure 2. Diagram depicting number of calls made to the helpline by gamblers
and relatives between 2009 and 2016.
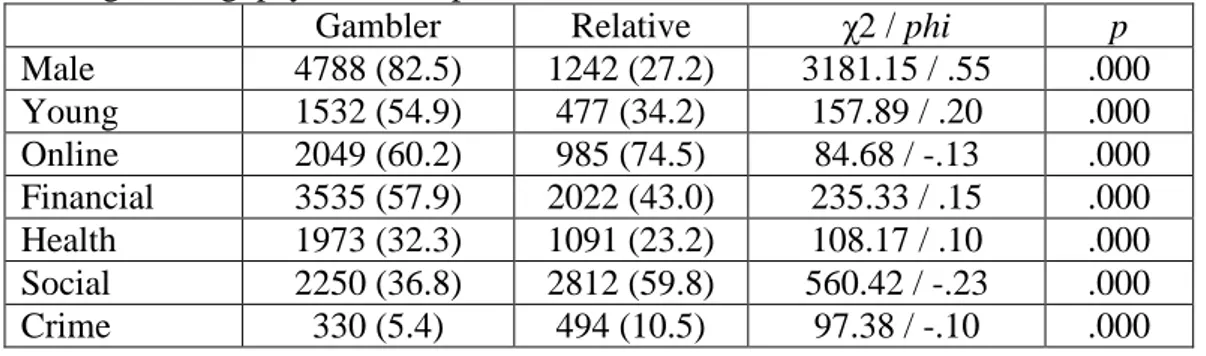
Differences between gamblers and relatives
Table 1 presents frequency and proportion of gamblers and relatives respectively concerning gender, age, online gambling, financial, health, and social problems, and crime. Also tabulated are chi-square and phi values of how gamblers and relatives differ in total. Significant differences were found indicating that in total, gamblers compared to relatives tend to be male, young, gamble offline, report financial and health problems. Relatives compared to gamblers tend to be female, older, report online gambling, social problems and crime. The largest effect size was the difference between gamblers and relatives regarding gender. The remaining effect sizes were small.
0 100 200 300 400 500 600 700 800 900 1000 2009 2010 2011 2012 2013 2014 2015 2016 Relative Gambler 0 500 1000 1500 2000 2500 3000 3500 4000 2009 2010 2011 2012 2013 2014 2015 2016
14
Table 1. Differences between gamblers and relatives concerning gender, age,
online gambling, psychosocial problems and crime.
Gambler Relative χ2 / phi p
Male 4788 (82.5) 1242 (27.2) 3181.15 / .55 .000 Young 1532 (54.9) 477 (34.2) 157.89 / .20 .000 Online 2049 (60.2) 985 (74.5) 84.68 / -.13 .000 Financial 3535 (57.9) 2022 (43.0) 235.33 / .15 .000 Health 1973 (32.3) 1091 (23.2) 108.17 / .10 .000 Social 2250 (36.8) 2812 (59.8) 560.42 / -.23 .000 Crime 330 (5.4) 494 (10.5) 97.38 / -.10 .000
Variations between different years
Table 2 presents the same variables as table 1 in frequencies (%) over the eight-year period 2009 to 2016. Intra-group analysis (i.e. gamblers and relatives separately) using chi-square test for independence showed multiple significant differences, however, the effect size ranged from .03 to .18 indicating that the differences were very small to small (Pallant 2010).
Differences between years for gamblers
The only significant difference in gender of gamblers calling the helpline was during 2011 when more males called, and 2016 when more females called, indicating that the gender distribution of gamblers was relatively stable.
During 2011, 2013, 2014, and 2015 significantly more young gamblers called the helpline while in 2012 significantly fewer young gamblers called the helpline, indicating an inclining trend in number of young gamblers calling the helpline.
Offline gambling was found to be significantly more prevalent during 2009, 2010, and 2011, while online gambling was found to be significantly more prevalent during 2014, 2015, and 2016 among gamblers calling. This indicates an increase of online gambling compared to offline gambling.
Gamblers reporting at least one financial problem was significantly less prevalent during 2009 and 2015, while significantly more prevalent during 2011 and 2012, indicating fluctuations but neither increase nor decrease over the time period.
Gamblers reporting at least one health problem was significantly more prevalent during 2011 and 2012, while significantly less prevalent during 2015 and 2016, indicating a declining trend.
Gamblers reporting at least one social problem was significantly more prevalent during 2010, 2011, and 2012, while significantly less prevalent during 2013, 2014, 2015, and 2016, indicating a declining trend of reporting at least one social problem.
Gamblers reporting having committed at least one financial crime was
15 T abl e 2. F re que nc y ( % ) of ge nde r, age , g am bl ing, pr obl em s a nd c ri m e for ga m bl er s a nd r el at ive s c a ll ing t he he lpl ine by ye ar 2009 – 2016. Y ear 2016 512 ( 77. 7) * 122 (72. 2) 343 ( 81. 3) * 348 ( 52. 4) 188 ( 28. 3) * 208 ( 31. 3) * 14 ( 2 .1) * 207 ( 30. 9) * 28 ( 3 4. 6) 177 ( 87. 2) * 265 ( 39. 0) * 113 ( 16. 6) * 366 ( 53. 9) * 53 ( 7 .8) * *= s ig. a t . 05 o r l ess . 2015 577 ( 79. 6) 120 ( 69. 8) * 342 ( 74. 7) * 393 ( 52. 4) * 181 ( 24. 1) * 224 ( 29. 9) * 32 ( 4 .3) 210 ( 29. 0) 32 ( 2 7. 6) 151 ( 80. 3) * 316 ( 42. 4) 127 ( 17. 0) * 393 ( 52. 8) * 57 ( 7 .7) * 2014 720 ( 83. 7) 124 ( 65. 6) * 361 ( 68. 2) * 498 ( 57. 0) 260 ( 29. 8) 267 ( 30. 6) * 50 ( 5 .7) 176 ( 30. 7) * 30 ( 3 1. 9) 85 ( 7 0. 8) 234 ( 39. 6) 123 ( 20. 8) 328 ( 55. 5) * 41 ( 6 .9) * 2013 583 (83. 9) 146 ( 64. 3) * 237 ( 62. 2) 425 ( 60. 2) 231 ( 32. 7) 205 ( 29. 0) * 19 ( 2 .7) * 154 ( 28. 7) 29 ( 2 2. 1) * 65 ( 6 8. 4) 199 ( 36. 4) * 138 ( 25. 3) 307 ( 56. 2) 35 ( 6 .4) * 2012 689 ( 82. 0) 262 ( 43. 0) * 331 ( 56. 9) 551 ( 65. 1) * 342 ( 40. 4) * 378 ( 44. 6) * 58 ( 6 .8) * 157 ( 27. 1) 108 (34. 2) 178 ( 79. 8) * 310 ( 53. 1) * 190 ( 32. 5) * 427 ( 73. 1) * 87 ( 1 4. 9) * 2011 708 ( 85. 5) * 289 ( 46. 8) * 218 ( 40. 3) * 566 ( 67. 5) * 328 ( 39. 1) * 378 ( 45. 1) * 73 ( 8 .7) * 152 ( 25. 8) 128 ( 34. 1) 122 ( 65. 9) * 310 ( 52. 0) * 173 ( 29. 0) * 399 ( 66. 9) * 86 ( 1 4. 4) * 2010 400 (80. 8) 196 ( 63. 2) 173 ( 43. 7) * 308 ( 60. 9) 158 ( 31. 2) 249 ( 49. 2) * 42 ( 8 .3) * 87 ( 2 0. 1) * 57 ( 4 2. 9) * 155 ( 64. 0) * 203 ( 43. 0) 93 ( 1 9. 7) 305 ( 64. 6) * 59 ( 1 2. 5) 2009 599 ( 82. 5) 273 ( 54. 8) 44 ( 4 5. 4) * 446 ( 48. 2) * 285 ( 30. 8) 341 ( 36. 8) 42 ( 4 .5) 99 ( 2 1. 2) * 65 ( 4 4. 2) * 52 ( 7 7. 6) 185 ( 37. 5) * 134 ( 27. 2) * 287 ( 58. 2) 76 ( 1 5. 4) * M al e Y oung O n lin e F in an ci al H ea lth S o ci al P er p etr atio n M al e Y oung O n lin e F in an ci al H ea lth S o ci al V ic tim is atio n G en d er Ag e G am b lin g P robl em Cr im e G en d er Ag e G am b lin g P robl em Cr im e G am b ler s R ela tiv es
16
prevalent during 2013 and 2016, indicating a decrease of help-seeking gamblers reporting at least one financial crime.
The trends seem to indicate that as time progressed, gamblers report being young, gamble online, report social and health problems and crime perpetration to a lesser extent.
Differences between years for relatives
Female relatives calling the helpline were significantly more prevalent during 2009 and 2010, while male relatives were significantly more prevalent during 2014 and 2016, indicating an increase in proportion of male relatives calling the helpline.
Significant differences in age were found in 2009 and 2010 where relatives tended to be younger, and in 2013 where relatives tended to be older.
Offline gambling was significantly more reported during 2010 and 2011 while online gambling was significantly more reported during 2012, 2015, and 2016, indicating an increase of relatives reporting online gambling as the primary platform for problem gambling.
Significant differences in relatives reporting at least one financial problem was found more prevalent during 2011 and 2012 while less prevalent during 2009, 2013 and 2016, indicating fluctuations and could suggest a declining trend.
Relatives reporting at least one health problem was significantly more prevalent during 2009, 2011, and 2012, while significantly less prevalent during 2015 and 2016, indicating a declining trend.
Similar trend was found in relatives reporting at least one social problem; most prevalent during 2010, 2011, and 2012, while least prevalent during 2014, 2015, and 2016.
Relatives reporting victimisation of at least one crime was significantly more prevalent during 2009, 2011, and 2012, while less prevalent during 2013, 2014, 2015, and 2016.
The trends seem to indicate an increase in male relatives, more online gambling, less financial, health, and social problems, as well as fewer relatives having been victimised as a result of problem gambling.
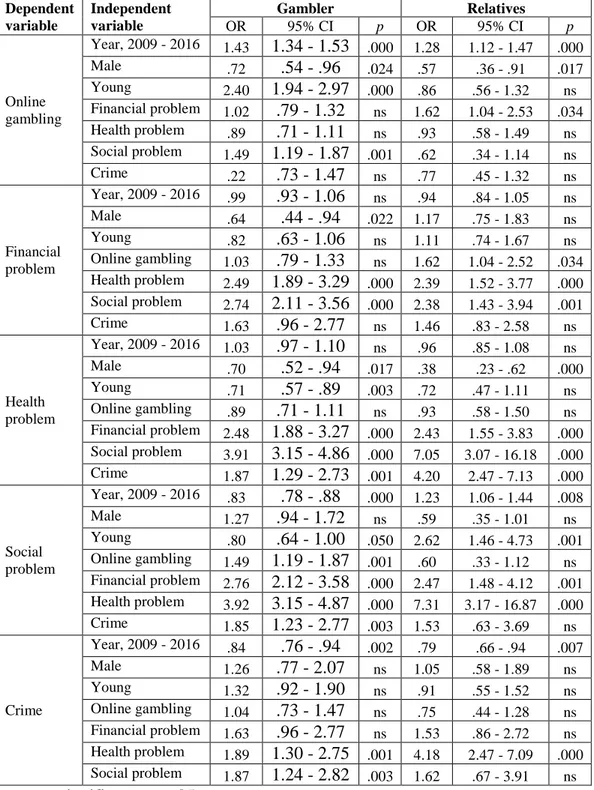
Associations of factors
Table 3 presents the results from the five binary logistic regressions showing odds ratios (OR, 95% CI) for online gambling, financial, health, and social problems as well as crime. Computations were done for gamblers and relatives separately, but the following text addresses the findings per dependent variable.
17
Chi-square analysis showed an increase in online gambling for both gamblers and relatives calling. The binary logistic regression with online gambling as dependent variable confirms this, showing a 43% increase for gamblers and 28% increase for relatives as time progressed. Furthermore, gamblers reporting online gambling is predicted by being young, having reported at least one social problem and being female. Relatives reporting online gambling is predicted by having reported at least one financial problem and being female.
Financial problem
No significant association between year and having reported at least one financial problem for either gamblers or relatives calling was found, indicating that
although specific years might differ in chi-square tests, there is no overall inclining or declining trend. Financial problems were, however, associated with health and social problems for both gamblers and relatives, and being a female gambler was also associated with having reported at least one financial problem.
Health problem
Gamblers reporting at least one health problem was associated with being female and older, but even more so by having reported financial and social problems. Having committed a financial crime was also a predictor in health problems. Relatives reporting at least one health problem was associated with being female. They were also 7 times as likely to report health problems if they also had
reported social problems, 4 times as likely if victimised and twice as likely is they had reported at least one financial problem. No significant association between year and health problems, which indicates that the declining trend in previous chi-square tests was negligible due to the small effect size.
Social problem
Having reported at least one social problem decreased for gamblers and increased for relatives as time progressed, indicating a confirmation of the previous chi-square test for gamblers but a contradiction for the chi-chi-square test run on relatives. Gamblers reporting at least one social problem is also associated with being 35-years and older, gamble online, having reported financial and health problems, and committed a financial crime. Relatives reporting at least one social problem is associated with being younger than 35 and having reported financial and health problems.
Crime
Gamblers reporting having committed at least one financial crime decreased as time progressed, which confirms previous chi-square tests. Having reported either health or social problem predicted having reported at least one crime, the
association is however not very strong. Relatives reporting having been victimised at least once decreased as time progressed, which also confirms previous chi-square tests. The only other independent variable associated with victimisation is having reported at least one health problem. The association is however strong indicating that relatives that report health problems are 4 times more likely to also have been victimised.
18
Table 3. Odds ratios (95% CI) for online gambling, gambling-related psychosocial
problems and crime in gamblers and relatives.
Dependent variable Independent variable Gambler Relatives OR 95% CI p OR 95% CI p Online gambling Year, 2009 - 2016 1.43 1.34 - 1.53 .000 1.28 1.12 - 1.47 .000 Male .72 .54 - .96 .024 .57 .36 - .91 .017 Young 2.40 1.94 - 2.97 .000 .86 .56 - 1.32 ns Financial problem 1.02 .79 - 1.32 ns 1.62 1.04 - 2.53 .034 Health problem .89 .71 - 1.11 ns .93 .58 - 1.49 ns Social problem 1.49 1.19 - 1.87 .001 .62 .34 - 1.14 ns Crime .22 .73 - 1.47 ns .77 .45 - 1.32 ns Financial problem Year, 2009 - 2016 .99 .93 - 1.06 ns .94 .84 - 1.05 ns Male .64 .44 - .94 .022 1.17 .75 - 1.83 ns Young .82 .63 - 1.06 ns 1.11 .74 - 1.67 ns Online gambling 1.03 .79 - 1.33 ns 1.62 1.04 - 2.52 .034 Health problem 2.49 1.89 - 3.29 .000 2.39 1.52 - 3.77 .000 Social problem 2.74 2.11 - 3.56 .000 2.38 1.43 - 3.94 .001 Crime 1.63 .96 - 2.77 ns 1.46 .83 - 2.58 ns Health problem Year, 2009 - 2016 1.03 .97 - 1.10 ns .96 .85 - 1.08 ns Male .70 .52 - .94 .017 .38 .23 - .62 .000 Young .71 .57 - .89 .003 .72 .47 - 1.11 ns Online gambling .89 .71 - 1.11 ns .93 .58 - 1.50 ns Financial problem 2.48 1.88 - 3.27 .000 2.43 1.55 - 3.83 .000 Social problem 3.91 3.15 - 4.86 .000 7.05 3.07 - 16.18 .000 Crime 1.87 1.29 - 2.73 .001 4.20 2.47 - 7.13 .000 Social problem Year, 2009 - 2016 .83 .78 - .88 .000 1.23 1.06 - 1.44 .008 Male 1.27 .94 - 1.72 ns .59 .35 - 1.01 ns Young .80 .64 - 1.00 .050 2.62 1.46 - 4.73 .001 Online gambling 1.49 1.19 - 1.87 .001 .60 .33 - 1.12 ns Financial problem 2.76 2.12 - 3.58 .000 2.47 1.48 - 4.12 .001 Health problem 3.92 3.15 - 4.87 .000 7.31 3.17 - 16.87 .000 Crime 1.85 1.23 - 2.77 .003 1.53 .63 - 3.69 ns Crime Year, 2009 - 2016 .84 .76 - .94 .002 .79 .66 - .94 .007 Male 1.26 .77 - 2.07 ns 1.05 .58 - 1.89 ns Young 1.32 .92 - 1.90 ns .91 .55 - 1.52 ns Online gambling 1.04 .73 - 1.47 ns .75 .44 - 1.28 ns Financial problem 1.63 .96 - 2.77 ns 1.53 .86 - 2.72 ns Health problem 1.89 1.30 - 2.75 .001 4.18 2.47 - 7.09 .000 Social problem 1.87 1.24 - 2.82 .003 1.62 .67 - 3.91 ns ns = not significant, p > .05
DISCUSSION
This study has explored the yearly differences regarding calls made to the national gambling helpline between 2009 and 2016 concerning gender, age, online
gambling, gambling related psychosocial problems, and crime. The slight
downward trend in total number of calls and number of help-seekers calling might be explained by increases in e-mail and chat contacts with the helpline (Stödlinjen 2016).
19
Help-seekers calling the gambling helpline tend to differ in gender and age depending on whether the caller is a gambler or a relative. Gamblers calling tend to be male and younger than 35 years, while relatives calling tend to be female and 35 years and older.
Online gambling was more commonly reported by relatives than gamblers, even though the majority of gamblers (60.2%) gambled online. There is also an association between being female and reporting online gambling for both gamblers and relatives confirming Svensson and Romilds’ (2011) assertion that online gambling is increasing for females. Being younger than 35 years was associated with online gambling for gamblers, but the age of the relative calling did not have any association with online gambling.
The significant differences in gambling related psychosocial problems between gamblers and relatives should be interpreted with caution due to the collection and processing of data. Variables included in determining whether any financial, health or social problem was reported, differ somewhat between gamblers and relatives calling. With that in mind, gamblers compared to relatives tend to report financial and health problems, while relatives tend to report social problems. Both gamblers’ and relatives’ health problems were associated with the caller being female. Gamblers’ but not relatives’ financial problems were associated with the caller being female. There also seems to be an association between all three psychosocial problems for both gamblers and relatives, indicating that problem gambling rarely only affects one area or one person.
More relatives compared to gamblers highlight crime in their conversation with the counsellors at the helpline. Differences between gamblers and relatives regarding crime should also be interpreted with caution due to the collection and processing of data. Nowhere in the data set was information about gamblers having been victimised due to gambling problems, nor relatives having committed crimes due to proximity to problem gambling. Furthermore, gamblers reporting having committed crime is solely financial, which is unlikely the only illegal behaviour (Dowling et al. 2016a; Meyer & Stadler 1999; Roberts et al. 2017). It is also strange that gamblers’ financial crimes are not associated with financial problems, but instead is associated with health and social problems.
Unlike for gamblers, there was no association between relatives’ highlighting crime and social problems. There was, however, a strong association between relatives reporting health problems and victimisation. Having been subjected to violence or having had money or valuables stolen by a close relative could not only affect one’s physical health but, perhaps even more so, one’s psychological health.
Over the eight-year period studied, online gambling increased for both gamblers and relatives; having reported at least one social problem decreased for gamblers and increased for relatives; and crime decreased for both gamblers and relatives.
Why there was an increase in online gambling cannot be determined by this study, only that there was an increase. Perhaps the increase could be due to additional new problem gamblers reaching the legal age for gambling and therefore choosing online gambling because of familiarity with computers, smartphones and tablets. Perhaps the increase indicates a shift from gambling in a casino or at a race track
20
to a more accessible and available platform. It might also be more difficult to stop gambling online compared to offline because even though one can ban oneself from a site, new sites keep starting up. For problem gamblers, gambling ads are triggers that increase the likelihood of relapse (Binde 2009), this in context to Swedish casinos being prohibited from advertising gambling might explain a transition from offline to online gambling among problem gamblers. These are, however, only speculations.
Even though fewer gamblers report social problems as time progressed, social problems seem to be interrelated with all of the other dependent variables. It could simply be that social problems are a talking point during calls to the helpline. However, based on previous research on comorbidities of problem gambling (Bonnaire, Kovess-Masfety, Guignard, Richard, Du Roscoät & Beck 2017; Lorains, Cowlishaw & Thomas 2011) it is more likely that gamblers’ social sphere is intrinsically bound to their well-being.
Why crime decreased for both gamblers and relatives cannot be determined based on this study of helpline callers, more research on this topic is needed.
CONCLUSION
Online gambling is predominant and increasing among help-seekers calling the helpline. Problem gambling affects people across multiple areas in life and it affects more than one person. The primary function of the gambling helpline is and should remain to offer support and information to people with a gambling related crisis. This study has shown crime to be associated with health and social problems among both gamblers and relatives seeking help. Because the
connection between gambling and crime has been highlighted in previous research it might be beneficial to include a crime-aspect to the counsellors’ training to fully capture the scope of gambling related crime among help-seekers calling the helpline.
21
REFERENCES
Abbott M, Binde P, Clark L, Hodgins D, Korn D, Pereira A, Quilty L, Thomas A, Volberg R, Walker D, Willams R, (2015) Conceptual framework of harmful
gambling: An international collaboration revised edition. Gambling research
exchange Ontario, Guelph, Ontario, Canada.
Altman J, Everitt B, Glautier S, Markou A, Nutt D, Oretti R, Phillips G, Robbins T, (1996) The biological, social and clinical bases of drug addiction: commentary and debate. Psychopharmacology, 125(4), 285-345.
Arthur J, Williams R, Belanger Y, (2014) The relationship between legal gambling and crime in Alberta. Canadian journal of criminology and criminal justice, 56(1), 49-84.
Ascher M, Levounis P, (2015) The behavioral addictions. Washington, DC and London, England. American psychiatric publishing.
Bastiani L, Fea M, Potente R, Luppi C, Lucchini F, Molinaro S, (2015) National helpline for problem gambling: A profile of its users’ characteristics. Journal of
addiction, 1-9.
Binde P, (2009) Exploring the impact of gambling advertising: An interview study of problem gamblers. International journal of mental health and addiction, 7(4), 541 – 554.
Binde P, (2011) What are the most harmful forms of gambling? Analyzing
problem gambling prevalence surveys. Center for public sector research,
University of Gothenburg, CEFOS.
Binde P, (2013) Why people gamble: A model with five motivational dimensions.
International gambling studies, 13(1), 81 – 97.
Blaszczynski A, Nower L, (2002) A pathways model of problem and pathological gambling. Addiction, 97(5), 487-499.
Bonnaire C, Kovess-Masfety V, Guignard R, Richard J B, Du Roscoät E, Beck F, (2017) Gambling type, substance abuse, health and psychological correlates of male and female problem gamblers in a nationally representative French sample.
Journal of gambling studies, 33, 343-369.
Calado F, Griffiths M D, (2016) Problem gambling worldwide: An update and systematic review of empirical research (2005-2015). Journal of behavioral addictions, 5(4), 592-613.
Challet-Bouju G, Hardouin J B, Renard N, Lagauffre C, Valleur M, Magalon D, Fatséas M, Chéreau-Boudet I, Gorsane M-I, Vénisse J-L, Grall-Bronnec M, (2015) A gamblers clustering based on their favorite gambling activity. Journal of
22
Delfabbro P, King D, Lambos C, Puglies S, (2009) Is video-game playing a risk factor for pathological gambling in Australian adolescents? Journal of gambling
studies, 25, 391-405.
Dowling N, Cowlishaw S, Jackson A, Merkouris S, Francis K, Christensen D, (2015) The prevalence of comorbid personality disorders in treatment-seeking problem gamblers: a systematic review and meta-analysis. Journal of personality
disorders, 29(6), 735-754.
Dowling N, Merkouris S, Lorains F, (2016b) Interventions for comorbid problem gambling and psychiatric disorder: Advancing a developing field of research. Addictive behaviors, 58, 21-30.
Dowling N, Suomi A, Jackson A, Lavis T, Patford J, Cockman S, Thomas S, Bellringer M, Koziol-Mclain J, Battersby M, Harvey P, Abbott M, (2016a) Problem gambling and intimate partner violence: A systematic review and meta-analysis. Trauma, violence & abuse, 17(1), 43-61.
Fauth-Bühler M, Mann K, Potenza M, (2017) Pathological gambling: A review of the neurobiological evidence relevant for its classification as an addictive
disorder. Addiction biology, 22(4), 885-897.
Gainsbury S, Hing N, Suhonen N, (2014) Professional help-seeking for gambling problems: Awareness, barriers and motivators for treatment. Journal of gambling
studies, 30, 503-519.
Glenn M, Diaz S, Moore L, (2006) Using problem gambling helpline data to inform addiction education. Journal of teaching in the addictions, 5(1), 31-44.
Grant J, Potenza M, Weinstein A, Gorelick D, (2010) Introduction to behavioral addictions. The American journal of drug and alcohol abuse, 36, 233-241. Griffiths M, Scarfe A, Bellringer P, (1999) The UK national telephone gambling helpline – Results on the first year of operation. Journal of gambling studies,
15(1), 83-90.
Harris, A., & Griffiths, M. D. (2018). The impact of speed of play in gambling on psychological and behavioural factors: a critical review. Journal of gambling studies, 34, 1-20.
Hawley C, Glenn M, Diaz S, (2007) Problem gambling in the workplace, characteristics of employees seeking help. Work, 29(4), 331-340.
Hing N, Tiyce M, Holdsworth L, Nuske E, (2013) All in the family: Help-seeking by significant others of problem gamblers. International journal of mental health
addiction, 11, 396-408.
Håkansson A, Mårdhed E, Zaar M, (20167) Who seeks treatment when medicine opens the door to pathological gambling patients – psychiatric comorbidity and heavy predominance of online gambling. Frontiers in psychiatry, 8, 1-6.
23
Kim H, Hodgins D, Bellringer M, Abbott M, (2016) Gender differences among helpline callers: Prospective study of gambling and psychosocial outcomes.
Journal of gambling studies, 32, 605-623.
Koob G, Le Moal M, (1997) Drug abuse: Hedonic homeostatic dysregulation. Science, 278, 52-58.
Ledgerwood D, Arfken C, Wiedemann A, Bates K, Holmes D, Jones L, (2013) Who goes to treatment? Predictors of treatment initiation among gambling help-line callers. The American journal on addiction, 22, 33-38.
Ledgerwood D, Steinberg M, Wu R, Potenza M, (2005) Self-reported gambling-related suicidality among gambling helpline callers. Psychology of addictive
behaviors, 19(2), 175-183.
Ledgerwood D, Wiedemann A, Moore J, Arfken C, (2012) Clinical characteristics and treatment readiness of male and female problem gamblers calling a state gambling helpline. Addiction research and theory, 20(2), 162-171.
Leshner A, (1997) Addiction is a brain disease, and it matters. Science, 278, 45-47.
Lewis M, (2015) The biology of desire: why addiction is not a disease. UK, Hachette.
Lorains F, Cowlishaw S, Thomas S, (2011) Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction, 106, 490-498.
Malmö University Ethical review of ethically sensitive student projects > https://www.mah.se/etikprovning< 2018-05-31
May-Chahal C, Humphreys L, Clifton A, Francis B, Reith G, (2017) Gambling harm and crime careers. Journal of gambling studies, 33, 65-84.
Meyer G, Stadler M A, (1999) Criminal behaviour associated with pathological gambling. Journal of gambling studies, 15(1), 29.43.
Muelleman R, DenOtter T, Wadman M, Tran P, Anderson J, (2002) Problem gambling in the partner of the emergency department patient as a risk factor for intimate partner violence. The journal of emergency medicine, 23(3), 307-312. Nutt D, (2013) Addiction: lifestyle choice or medical diagnosis? Journal of evaluation in clinical practice ISSN, 19, 493-496.
Orford, J. (2001) Addiction as excessive appetite. Addiction, 96, 15-31. Pallant J, (2010) SPSS survival manual. McGraw-Hill education. UK
Petry N, Blanco C, Stinchfield R, Volberg R, (2012) An empirical evaluation of proposed changes for gambling diagnosis in the DSM-5. Addiction, 108, 575-581.
24
Potenza M, Steinberg M, McLaughlin S, Wu R, Rounsaville B, O’Malley S, (2001) Gender-related differences in the characteristics of problem gamblers using a gambling helpline. The American journal of psychiatry, 158(9), 1500-1505.
Potenza M, Steinberg M, Wu R, Rounsaville B, O’Malley S, (2006)
Characteristics of older adult problem gamblers calling a helpline. Journal of
gambling studies, 22, 241-254.
Public Health Agency of Sweden (2016) Gambling and gambling problems in
Sweden 2008 – 2010. Swedish Longitudinal Gambling Study, Swelogs Findings from wave one and wave two.
>https://www.folkhalsomyndigheten.se/contentassets/fe1d3ba6e62a40158a8188b b3b83b9c5/gambling-gambling-problems-sweden-2008-2010-16013.pdf< (2018-05-18).
Pulford J, Bellringer M, Abbott M, Clarke D, Hodgins D, Williams J, (2009a) Reasons for seeking help for a gambling problem: The experiences of gamblers who have sought specialist assistance and the perceptions of those who have not.
Journal of gambling studies, 25, 19-32.
Pulford J, Bellringer M, Abbott M, Clarke D, Hodgins D, Williams J, (2009b) Barriers to help-seeking for a gambling problem: The experiences of gamblers who have sought specialist assistance and the perceptions of those who have not.
Journal of gambling studies, 25, 33-48.
Rennert L, Denis C, Peer K, Lynch K, Gelernter J, Kranzler H, (2014) DSM-5 gambling disorder: Prevalence and characteristics in a substance use disorder sample. Exp clin psychopharmacol. 22(1), 50-56.
Roberts A, Landon J, Sharman S, Hakes J, Suomi A, Cowlishaw S, (2018) Gambling and physical intimate partner violence: Results from the national epidemiologic survey on alcohol and related conditions (NESARC). The American journal on addictions, 27, 7-14.
Rodda S, Hing N, Lubman D, (2014) Improved outcomes following contact with a gambling helpline: the impact of gender on barriers and facilitators.
International gambling studies, 14(2), 318-329.
Satel S, Lilienfeld S, (2017) If addiction is not best conceptualized a brain disease, then what kind of disease is it? Neuroethics, 10(1), 19-24.
Sinclair H, Pretorius A, Stein D, (2014) A counselling line for problem and pathological gambling in south Africa: Preliminary data analysis. Journal of
behavioral addiction, 3(3), 199-202.
Stödlinjen (2016) Stödlinjen för spelare och anhöriga - Årsrapport 2016.
25
Suurvali H, Cordingley J, Hodgins D, Cunningham J, (2009) Barriers to seeking help for gambling problems: A review of the empirical literature. Journal of
gambling studies, 25, 407-424.
Svensson J, Romild U, (2011) Incidence of internet gambling in Sweden: results from the Swedish longitudinal gambling study. International gambling studies,
11(3), 357-375.
The Data Protection Act, 1998:204 >http://www.riksdagen.se/sv/dokument- lagar/dokument/svensk-forfattningssamling/personuppgiftslag-1998204_sfs-1998-204< 2018-05-30
The Ethical Review Act, 2003:460 >http://www.riksdagen.se/sv/dokument- lagar/dokument/svensk-forfattningssamling/lag-2003460-om-etikprovning-av-forskning-som_sfs-2003-460< 2018-05-30
The Health and Medical Services Act, 2017:30
>https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/halso--och-sjukvardslag_sfs-2017-30< 2018-05-18
The Social Services Act, 2001:453 > https://www.riksdagen.se/sv/dokument- lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453< 2018-05-18
Valdivia-Salas S, Blanchard K, Lombas A, Wulfert E, (2014) Treatment-seeking precipitators in problem gambling: Analysis of data from a gambling helpline.
Psychology of addictive behaviors, 28(1), 300-306.
Wardell J, Quilty L, Hendershot C, Bagby M, (2015) Motivational pathways from reward sensitivity and punishment sensitivity to gambling frequency and
gambling-related problems. Psychology of addictive behaviors, 29(4), 1022-1030.
Williams R, Royston J, Hagen B, (2005) Gambling and problem gambling within forensic populations: A review of the literature. Criminal justice and behavior, 32(6), 665-689.
Williams R, West B, Simpson R, (2007) Prevention of problem gambling: A comprehensive review of the evidence. Report prepared for the Ontario problem gambling research centre. Guelph, Ontario, Canada.
26
APPENDICES
Appendix 1
The data was received in an excel-file. The first step was therefore converting the file to an SPSS-file. Each variable then needed to be given values for SPSS to be able to make computations. The data set contained 22,285 calls. After deliberation with researchers at KI, the calls during 2008 (only one month) were excluded because it was a trial period for the helpline data base. The remaining 22,260 calls contained 102 variables with various degrees of response rates. Some variables were binary like gender and others were descriptive containing up to 306 different nominal values.
There were three variables where counsellors had given a short description of the call as a primary categorisation of either calls related to 1) gambling for money, 2) not gambling for money, and 3) other problems. Gambling for money contained 306 different descriptions that were categorised by the author as either support, information or other. ‘Not gambling for money’ contained 202 different
descriptions that were categorised by the author as misdials, prank calls or other. ‘Other problems’ contained 91 different problems that were not primarily
gambling for money (e.g. shopping, computer games, sex, and stocks) but was the main focus of the call and was therefore dichotomized as ‘other problem’ yes/no. These three variables had an overlap of 812 cases (callers). After examining those cases and categorising them as either a gambling related call or not, a second exclusion was made leaving 13,574 calls that were in some way gambling related.
The data set contained multiple variables pertaining to gamblers and relatives. In the data set, these were sorted left to right beginning with gamblers. This
‘gamblers-block’ and ‘relatives-block’ had an overlap which needed to be distinguished. Creating response rate variables for specific gambler and relative aspects (see appendix 2), adding them separately yielding two variables showing how many cases have responded to 1,2,3…19 variables. This was then
dichotomized to yield one ‘gambler calling’ variable (1 for any respond) and one ‘relative calling’ variable (-1 for any respond). Summing the two variables yielded a single variable with -1, 0, and 1 where ‘0’ was an overlap (i.e. cases with
information in both relative-block and gambler-block). After deliberation with researchers at KI and examining the overlap by hand it was decided that the 510 cases were most likely relatives calling and talking about a gambler whereby the counsellors input data in both blocks. Another 274 cases that only had 1 or 2 variables in relative’s demographics were inspected and no overlap with gambler-block was found and those cases could therefore also be added to ‘relatives calling’. This process yielded 6110 (45%) gamblers calling, 4706 (34.7%) relatives calling and 2758 (20.3%) other or missing values.
27 Appendix 2
Creating ‘Gambler calling’ using response rate (0/1):
Variables added together to yield ‘Gambler calling’: gender, age, living situation, occupation, primary problem game, GPLM10 how often, GPLM time spent, GPLM bets, problem onset, economic problems x4 (own assessment, debt, other consequences, crime), health problems x3 (own assessment physical, own
assessment psychological, other consequences), social problems x2 (relationships and work/studies).
Creating ‘Relative calling’ using response rate (0/1):
- Sum relative’s gender, relative’s age, player’s gender, and player’s age yielding a variable with variance 1 to 4. Recoded 3 and 4 as 1, 1 and 2 as missing.
- Sum ‘player phase’ and ‘how did you get to know’, recoded as 1 for any response.
- Sum relative’s psychosocial problems using economic problems x3 (own assessment, problems like, and consequences), health problems x3 (own physical assessment, own psychological assessment, and other
consequences), social problems x2 (relationships and work/studies). Recode into ‘at least one EHS’ 1 for yes.
- Sum the three steps above and then further recode into ‘relative calling’ -1 for yes.
Psychosocial problems recoding
Financial: Respondents assessed their own economy as bad and out of control, bad but under control, and good. This was dichotomized to good (0) and bad (1). Gambling related debt ranged from 0 to over 1 million kronor in 11 unequally distant brackets and a 12th option of ‘player does not know’. This was recoded into whether there was a gambling debt (1) or not (0), ‘player does not know’ was excluded. Other consequences were things like gambled away company, cancelled dentist’s appointment, payment remarks and more. This variable was recoded ‘any other financial consequences’ 1 for yes. Together these 3 variables were summed to create a variable ranging 0-3. This was then also dichotomized into ‘any financial problems’ 0 for no, 1 for yes.
Health: Callers assessed their physical and psychological health as good, bad, or neither good nor bad. Both of these 2 variables were dichotomized into good/neither good nor bad (0) or bad (1). Sleep was dichotomized from ‘no effect, sleep issues du to gambling, and sleep issues due to stress/anxiety’ to any sleep issues (0) no, (1) yes. Other health consequences contained information about suicidality and alcohol/drug abuse and was recoded to ‘any other health consequences’ 1 for yes. Together these 4 variables were summed to create a variable ranging 0-4. This was then also dichotomized into ‘any health problems’ 0 for no, 1 for yes.
Social: Relationships were dichotomized as ‘has had an effect’ (1) and ‘no effect’ (0). Current residential problems ranged from ‘no problem’ to ‘homeless’, and was dichotomized as ‘has not had an effect’ (0) and ‘has had an effect’ (1). Work/Study
28
contained no effect, neglecting, sick leave, risk losing employment/lost employment and was dichotomized as no effect (0) has affected work/study (1). Together these 3 variables were summed to create a variable ranging 0-3. This was then also dichotomized into ‘any social problems’ 0 for no, 1 for yes.
Financial: For relatives calling, their own economic assessment was dichotomized as good or bad, ‘problems like’ was the same as the gamblers’ ‘other consequences’ and was recoded as (1) yes, there has been consequences. The third variable contained data on loans, paid with savings and have had money or things stolen. Having had money or things stolen was extracted to form a variable of its own and the rest was dichotomized as (0) no consequences and (1) yes, there has been financial consequences. Same dichotomization as gamblers.
Health: Relatives calling assessed their physical and psychological health as good, bad, or neither good nor bad. Both of these 2 variables were dichotomized into good/neither good nor bad (0) or bad (1). Sleep was dichotomized from ‘no effect, sleep issues du to gambling, and sleep issues due to stress/anxiety’ to any sleep issues (0) no, (1) yes. Other health consequences contained data on physical and psychological abuse as well as alcohol/drug abuse. The physical and psychological abuse was extracted to create a crime victimization variable and the substance abuse was dichotomized as 1 for yes.
Social: 3 social variables for relatives were processed like for gamblers explained above.
29 Appendix 3
Malmö universitet / Fakulteten för Hälsa och samhälle
Etikrådet
Adm sekreterare Ewa Sortberg Bassmann
Utlåtande
2018-02-16 HS2018 löp nr 17
Projekt:
Projekt: Problemspelare och anhöriga som kontaktar Stödlinjen – En utforskning av karakteristik från klusteranalys över tid
Student: Erik Rosenberg
Handledare: Claes Andersson
Föredragande: Camilla Nordgren
Etikrådets utlåtande:
Projektet syftar till att utforska mönster vad gäller karakteristik och spelrelaterade problem över tid för spelare och anhöriga som kontaktar Stödlinjen. Material, bestående av dokumentation av handläggare vid Stödlinjen, är helt anonymiserat och går ej att koppla till någon individ.
Etikrådet har inget att invända mot genomförandet av detta projekt i enlighet med ansökan.
För Etikrådet vid Fakulteten för hälsa och samhälle, Malmö universitet Camilla Nordgren