Contents lists available atScienceDirect
Sexual & Reproductive Healthcare
journal homepage:www.elsevier.com/locate/srhcMidwives
’ counselling of women at specialised fear of childbirth clinics: A
qualitative study
Ann-Charlotte Wulcan
a,⁎, Christina Nilsson
b,caNorthern Älvsborg County Hospital, NU-Hospital Group Trollhättan/Uddevalla, Västra Götaland Regional Council, 461 73 Trollhättan, Sweden bFaculty of Caring Science, Work Life and Social Welfare, University of Borås, Allegatan 1, 501 90 Borås, Sweden
cInstitute of Health and Care Sciences, The Sahlgrenska Academy at the University of Gothenburg, Box 100, 405 30 Gothenburg, Sweden
A R T I C L E I N F O Keywords: Fear of childbirth Midwifery Experiences Content analysis Treatment Counselling A B S T R A C T
Objective: Fear of childbirth is a well-known problem affecting women’s wellbeing and health. The prevalence of intense fear varies across countries from 4.8 to 14.8%. During the past 25 years in Sweden women with intense fear of childbirth have been offered counselling at specialised clinics staffed by midwives. Although the coun-selling demonstrates positive results, the training, education, supervision and organisation differ between clinics. It is still unclear which approaches and practices are the most beneficial. The aim was to explore and describe the counselling of women with intense fear of childbirth from the viewpoint of midwives who provide counselling in specialised fear of childbirth clinics in one region of Sweden.
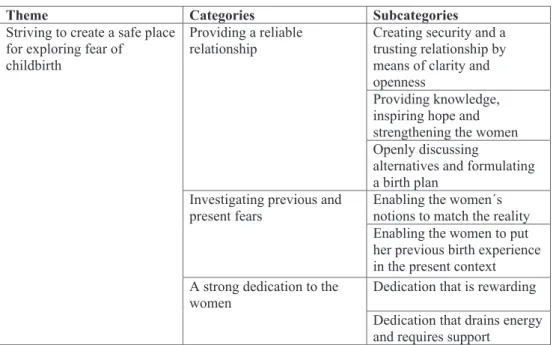
Methods: A qualitative study of 13 midwives using focus group interviews and inductive content analysis. Results: The midwives’ counselling of women with intense fear of childbirth is described as ‘striving to create a safe place for exploring fear of childbirth’, comprising the following categories: Providing a reliable relationship; Investigating previous and present fears; and A strong dedication to the women.
Conclusion: Although there are no guidelines for the counselling the midwives described similar frameworks. Some approaches were general, while others were specific and related to the individual woman’s parity. The midwives achieved professional and personal development through counselling experiences. Thefindings add to the existing literature on counselling and can be used to inform the development of midwife-led interventions for women with intense fear of childbirth and previous traumatic births, as well as for the formal education of midwives.
Introduction
Fear of childbirth (FOC) affects women’s wellbeing and health[1] and is an important reason for the increasing number of requests for and rates of caesarean section (CS) in Europe, Australia and the United States[2,3]. There are inconsistencies in the tools used for measuring FOC, reflecting the problems in defining women’s FOC [4]. When measured in the same way, the prevalence of intense FOC varies from 4.8% in Australia[5]to 6.3% in Belgium and 14.8% in Sweden[6]. Intense FOC is usually described as a fear that influences women’s daily life[7,8]. Fear occurring before a woman’s first childbirth is described as primary FOC[9], while secondary FOC is often related to previous birth experiences[9–12]. According to a recent systematic review, the strongest predictor of FOC is a previous negative or traumatic birth experience and operative birth[13]. A study from Sweden[1]found
that women with intense FOC had a higher rate of sick leave and made more health care visits during pregnancy and the postpartum period than those with low levels of FOC. They also stayed longer in the labour ward and had more complicated childbirths, including higher rates of planned CS[1].
The number of randomised controlled trials (RCT) conducted on different prenatal FOC interventions[14,15]is limited. However, some interventions have demonstrated positive effects on women’s FOC[15], including one study from Finland on individual cognitive-behavioural therapy (CBT) led by an obstetrician[16]and one study from Australia on telephone counselling provided by midwives who had training in psychoeducation[17]. The Australian study also indicated other ben-efits for women, such as a reduction in overall CS rates and a preference for vaginal birth in their next pregnancy[18]. Other examples of in-terventions showing a positive effect on women’s fear[15]are prenatal
https://doi.org/10.1016/j.srhc.2018.12.001
Received 10 April 2018; Received in revised form 26 November 2018; Accepted 2 December 2018
Abbreviations: CBT, cognitive behavioural therapy; FOC, fear of childbirth; FOC clinic, specialised fear of childbirth clinic where midwives provide counselling for women with intense fear of childbirth; CS, caesarean section; RCT, randomised controlled trial
⁎Corresponding author.
E-mail addresses:ann-charlotte.wulcan@vgregion.se(A.-C. Wulcan),christina.nilsson@hb.se(C. Nilsson).
1877-5756/ © 2018 Published by Elsevier B.V.
childbirth education[19], an education course at the hospital[20]and prenatal yoga [21]. Moreover, a specific counselling model for post-partum women who experienced a traumatic birth[22]has also shown promising results[23]. Available studies seem to indicate that different forms of counselling reduce FOC and although consensus on the best treatment for women has not yet been achieved, the studies are not contradictory.
As all maternity care in Sweden is state funded (except for home birth), almost all pregnant women avail of it. Traditionally, midwives in Sweden have an independent role and are responsible for care during pregnancy and labour. If complications occur, obstetricians take over the responsibility, although midwives still play an active part in the care. For the past 25 years, FOC clinics have been introduced at most hospital labour wards in Sweden [24]. These FOC clinics provide counselling by midwives and obstetricians for women with intense FOC [24,25], including women who request a CS without medical reasons. Women in Sweden are not entitled to have a planned CS without medical reasons, which does not include intense or phobic FOC[26]. Before obstetricians make thefinal decision about CS they must fulfil the following requirement; the woman has been offered and/or re-ceived supportive counselling and information about the short and long-term consequences of CS [26]. Studies have demonstrated that women are generally satisfied with the counselling received and about half withdrew their request for CS afterwards[24,25,27,28]. Women also describe the counselling as increasing their confidence in giving birth through the support from the midwife and that receiving in-formation and knowledge made them feel safer, which had a positive impact on their birth experience [29]. Midwives at antenatal clinics considered the FOC clinics valuable resources when caring for women with FOC [30]. Midwives at labour wards experienced the care of women with FOC as demanding[31]and expressed a desire for more knowledge of the condition [30]. In a national survey, Larsson et al. [32]found that FOC clinics provided various forms of care and were organised in different ways. The education and supervision of staff also differed. Although midwives working at FOC clinics have gained much experience over the years, their counselling has not yet been explored and described in qualitative studies, particularly in terms of useful methods, strategies, challenges and content.
In summary, most women suffering from intense FOC in Sweden are referred to FOC clinics. Women are generally satisfied with the coun-selling provided, resulting in many withdrawing their request for CS. However, studies demonstrate that the training, supervision and orga-nisation of midwife counsellors vary between FOC clinics. In addition, research is limited on the content of the counselling and the factors leading to positive changes. It is still unclear which approaches and practices are the most beneficial. Studies exploring the counselling provided by midwives can add to the knowledge of how to approach and support women with intense FOC. It is time to gather information from experienced midwife counsellors before they retire by asking them to describe their counselling sessions, challenges and which compo-nents they consider important. Therefore, the aim of this study was to explore and describe the counselling of women with intense FOC from the viewpoint of midwives who provide counselling in FOC clinics in one region of Sweden.
Method
In this qualitative study, focus group interviews were used to collect data[33], which were analysed by means of an inductive approach to qualitative content analysis [34], a method considered appropriate when little is known about the research subject[35]. Content analysis has a long history in both quantitative and qualitative research and has been developed as a qualitative method for analysing textual data in health research[36].
Setting and participants
The interviews were conducted in a region of southern Sweden. Following our request, the managers of four FOC clinics chose partici-pants with long experience as midwives who provided counselling and worked at a labour ward. The midwives’ work experience ranged from 8 to 41 years. Their experience in the area of counselling averaged 8 years, ranging from 6 months to 20 years. The midwives generally worked at FOC clinics for 23.5 h a month, ranging from 8 to 64 h a month. They usually counselled women with intense FOC on two or three occasions and the women’s partners were welcome to attend. About two thirds of the women sought counselling due to fear after previous negative childbirth experiences. Moreover, the midwives had different levels of special education in counselling, most commonly some training in CBT and motivational interviewing. All participants took part in regular group supervision.
Data collection
Data were collected by means of four focus group interviews, each with two tofive participants, during May and June 2015. The region has four hospitals (including one university hospital], which together handle approximately 18,800 births annually [37]and all have FOC clinics. Midwives from all four hospitals were represented, but not in each focus group interview. Thefirst three interviews took place at a conference room in a neutral location with participants from three of the hospitals. Due to a busy work schedule, thefinal interview only involved participants from the fourth hospital, who were interviewed at their work place.
During thefirst three interviews, an observer (a midwife with focus group experience) was responsible for the audio recording and asked follow-up questions when necessary. In a presentation before the in-terview, the roles of the interviewer and the observer were explained and information about the study was provided. The interviews were audio recorded and lasted between 83 and 113 min. Three research questions were posed during all interviews: (1)‘Can you please describe a typical counselling session?’ (follow-up questions concerned structure and content); (2)‘What do you think are the most effective components of counselling?’ (follow-up questions concerned requirements for change to occur); and (3) ‘Can you please describe emotional en-counters with women?’ (follow-up questions concerned what was easy/ difficult).
Data analysis
Data were analysed using the content analysis method described by Elo and Kyngäs[34], which permits an inductive approach in which categories are directly suggested by the data without the use of theory. The interviews were transcribed verbatim and then analysed through a process of identifying the units of analysis, open coding, creating ca-tegories and abstracting[34].
The data analysis started with a thorough reading of the transcribed interview text as a whole. Next, labels and headings describing each unit of analysis (portions of the interview texts that answered any of the three research questions) were written in the margins. These headings were then entered into coding sheets, compared and grouped together based on their similarities. Content that belonged together was grouped and re-grouped until no further merging under a higher-order heading (abstraction) was possible. Eventually, a main category and three ca-tegories based on subcaca-tegories were identified from the data. Ethical considerations
The study was carried out in accordance with the Code of Ethics set out in the Declaration of Helsinki. Permission to carry out the study was obtained from the heads of the obstetrics and gyneacology departments
at the participating hospitals. Ethical approval was granted by the Regional Ethical Review Board, Gothenburg (2015-03-19, No. 148-15). Permission to conduct and audio-record the interviews was received in writing (consent form) from each participant. The participants were also guaranteed, both verbally and in writing, that all information would be treated confidentially and that they could withdraw from the study at any time without the need to give a reason.
Results
Several midwives stated that it was difficult to describe a typical counselling session. Nevertheless, a common framework emerged from their descriptions. The following theme, categories and subcategories were identified.
The midwives’ counselling of women with intense FOC at FOC clinics was described in the theme ‘Striving to create a safe place for exploring fear of childbirth’. This meant that despite the sometimes challenging circumstances, the midwives were dedicated in their at-tempt to achieve a mutual dialogue and a trusting relationship in an atmosphere where the women felt safe and free to examine previous and present fears together with them.
The following categories; Providing a reliable relationship, Investigating previous and present fears and A strong dedication to the women are described with their respective subcategories and illustrated by quotations (seeFig. 1).
Providing a reliable relationship
The midwives tried to provide a reliable relationship by means of the strategies described in the subcategories below.
Creating security and a trusting relationship by means of clarity and openness
The midwives clarified the framework early in the first session, in-cluding confidentiality, documentation in the medical record and the time frame (one hour). The most common strategy during this session was to encourage the women to speak freely about their fears. The midwives experienced that most women had no problem opening up during the sessions, but a few found it difficult. The midwives sum-marised what the women had said, which prevented misunderstandings
and created consensus. The midwives emphasised that it was necessary to listen respectfully. Many women expressed that it felt good to talk to someone who was non-judgemental and not directly involved. The midwives confirmed the women’s experience by saying: “I hear you and I can see that this is hard for you”. It was vital to have sufficient time and focus on each woman's story.
“The main thing is that on some level they feel: ‘I can trust you as a midwife’.”
Several midwives described observing visual changes in the wo-men’s bodies during counselling, for example a woman who was tense and worried when she arrived went home relaxed. The midwives hoped that once the women felt that they could communicate with and trust the midwife, they would be willing to transfer this trust to the midwives at the labour ward. If the women had not received appropriate care at the previous birth, the midwives confirmed this and apologised, which might serve as a form of atonement for the women.
“She had been rejected on the phone, she had been so lonely, so vul-nerable. (…) She came anyway when she felt that she needed help, but the staff had no time for her, (…) someone just quickly checked on her from time to time. And when I said:‘I’m so sorry, you really didn’t get what you needed, that was really bad care’, it was exactly what she needed. (…) She had felt guilty that she couldn’t keep herself together and manage at home until a bed was available.”
The midwives also mentioned difficulties in building a trusting re-lationship. This was most clearly articulated in relation to women with a strong desire for a CS as well as those who expressed their fear by anger. The midwives avoided entering into a verbal battle as it might be difficult to find the appropriate words to diffuse the situation.
“So it doesn’t turn into a fight, because when you have a fight in your room, it will never work. Somehow we mustfind a way to connect to this woman.”
The midwives had different views about their part in the decision-making process regarding the mode of birth. Some considered that the fact that women had no right to choose a CS made it vital to ensure that each woman understood and accepted this situation. Others thought that they helped the women to take a decision by providing information about the benefits and disadvantages but at the same time tried not to put pressure on them. Even if their own view was that a vaginal birth
would be best for mother and child, they also acknowledged that a CS was a better alternative for some women and arranged appointments with obstetricians to discuss CS when necessary.
“I have had some who were approved for a CS and they were so happy and so present in that situation, expressing that they had had a lovely experience. (…) I am just as happy about those who have given birth in that way.”
Other difficulties involved women who avoided talking about their fear or partners who took over and spoke on their behalf.
“(…) he leaned back and put his arms like this and said ‘Now you listen to me…’ and when that happens I get so terribly provoked that I have to breathe really hard and try to talk in a calm manner. It was exactly the same type of man who said:‘But honestly, isn’t giving birth vaginally very out of date?’.”
Providing knowledge, inspiring hope and strengthening the women The midwives became more active in the subsequent phases of the counselling session. Providing individualised information was con-sidered a powerful component. They emphasised that they conveyed knowledge based on facts and felt that their work at the labour ward made them appear trustworthy. The midwives stressed that it was es-sential for the women to believe that they could give birth vaginally. For parous women who felt that they had failed to give birth normally because they had required a vacuum extraction or emergency CS, the midwives tried to change that notion by explaining that a previous birth led to physical advantages when giving birth again and by providing information about the success rate of vaginal birth after a previous CS. They assured the women that the next birth would be different.
“I say: ‘You are in great condition and will receive help’ and so many listen to what I say (…) we must be able to help them regain hope.” The midwives considered the staff shortage within labour wards as one reason for FOC. The women’s fear of not having all the help and support they needed was shared by the midwives, which represented a dilemma, as they knew how difficult the situation could be at the labour ward. Nevertheless, they had to build trust and help the women over-come their fear.
“If only I could really promise her that we will take care of her and be there for her all the time. But I can’t. I believe that is one huge reason why women are afraid.”
Openly discussing alternatives and formulating a birth plan
During the last counselling session, the women and the midwives discussed alternatives and formulated a birth plan, which consisted of a short background and what the women needed and wished for during the birth. Some things were general, such as the provision of informa-tion, while others were more specific, such as the need for an early epidural. The midwives considered the birth plan important for the women, as documenting what had been agreed made them feel safe and reduced their anxiety.
“For them to read it actually works very well. It’s like a summary of all our sessions, it’s the conclusion. I want the patient to agree with what I have written.”
The midwives wanted to have a follow-up meeting or telephone call after the birth to talk about the women’s birth experiences, but they had limited time for this. Even at this stage the midwives made efforts to strengthen the women’s belief in themselves and their ability.
Investigating previous and present fears
The most common way of working with both nulliparous and parous women was counselling sessions in combination with visits to the la-bour ward. However, the content of the counselling differed in ac-cordance with the women’s parity, which is described in the following two subcategories.
Enabling the women’s notions to match the reality
The midwives stated that it was more difficult to counsel women who were expecting their first baby. Nulliparous women were en-couraged to relate what they had heard from others, both “horror births” and “perfect ones”. The counselling enabled them to pinpoint their fears and compare them with the reality. Some women who were unable to express their fears were advised to consult a psychologist. The midwives provided information about the birthing process and helped the women to develop realistic thoughts about giving birth. Several women were perceived as putting a great deal of pressure on themselves to manage the birth and not embarrass themselves.
Some women had frightening visions about the labour ward looking like a slaughterhouse. Visiting a labour room was beneficial because they could see that their fearful visions did not match the reality. Moreover, meeting a kind and welcoming midwife during the visit could make a huge difference.
Enabling the women to put their previous birth experience in the present context
The most common reasons for parous women to require counselling were previous prolonged births and negative experiences of encounters with staff, e.g., not being listened to or seen as an object. Other reasons were being shocked by their own reactions or behaviours or frightened by adverse events (e.g., vacuum extraction, the baby being unwell) during a previous birth. The midwives considered that both external and internal factors influenced how the women experienced the childbirth. What was objectively deemed an“easy” birth could be ex-perienced as the worst thing that had ever happened.
Although the women were afraid, many wanted help to dare give birth again. The fear mostly concerned having the same experience as on the previous occasion. The midwives said that for a substantial change to occur in parous women, they needed to understand what had happened and why. The midwives described the following stages: al-lowing the women to describe the previous birth in their own words, reading through the medical record of the previous birth together, normalising the situation, strengthening the women and eventually using their previous birth experience to plan the next birth.
Thefirst session was devoted to the previous birth experience. The midwives believed it had a healing effect for the women to put their thoughts and feelings into words and have them confirmed. It often elicited strong emotional reactions and many women cried. Some had never spoken about their previous birth experience before.
“One woman said after her first appointment: ‘I was totally spent after our last meeting, I couldn’t go to work, I went to bed, it was so ex-hausting’.”
Reading the medical record from the previous birth together was seen as extremely beneficial. The midwife suggested possible explana-tions and corrected misunderstandings, while again confirming the women's experience. The expectant mothers obtained answers and felt relieved afterwards.
The midwives tried to alter the women’s negative feelings about the previous childbirth, partly by strengthening their self-confidence and partly by normalising the situation. Many women felt they had failed and some felt so bad for a long time afterwards that they even ex-perienced difficulty attaching to their baby. Women with traumatic
childbirth experiences were encouraged to visit the labour ward before giving birth again to understand and accept what had happened. Some recalled how difficult it had been and started to cry, while others rea-lised that it was not as distressing as they had imagined. The writing of a birth plan was vital for the women.
A strong dedication to the women
The midwives were very dedicated to the women. It seemed as if they invested emotionally in them and often thought about ‘their’ women. The midwives revealed positive and negative experiences from their counselling work, both professionally and in their relationship with the women and in their collaboration with other midwives and obstetricians at the labour ward, which are described in the following two subcategories.
Dedication that is rewarding
The midwives emphasised how the work at the labour ward and the FOC clinic cross fertilised each other and made them more skilled. The counselling helped them to understand the importance of communica-tion and informacommunica-tion. They learned how words could be perceived and became aware of how the couple read the staff at the labour ward and therefore took care when informing them.
The midwives expressed satisfaction at seeing the women grow mentally, both during counselling and in the birthing room. It was described as fantastic when women with a previous traumatic birth experience had a positive experience and felt healed and whole again. The midwives also received positive feedback from the women.
“You want it to be good for the other person and then you get so much in return. It’s some kind of magnificent feeling, a win-win-situation really.” A reason for the midwives working at the FOC clinic was the close encounters. One midwife said:“It’s very exciting, you never know at the first counselling session what the journey will be like”. They learned about people, how they thought, experienced things and handled their lives. It gave them so much in return and broadened their horizons. Counselling was also seen as a way of developing oneself. One midwife said that it had taught her thefinishing touches of midwifery.
“This is a part of some kind of process I think, if you look at how you were as a new midwife or nurse. Then you wanted to have the technical skills, to be good at inserting a needle (…). That no longer makes me feel proud, instead the most important thing in midwifery is these personal encounters with women and their partners.”
The midwives also described boundaries to their dedication. A principle was not to attend to women during labour who they had encountered in counselling. The midwives did not want to feel per-sonally responsible for them during the birth. Instead, they wished to strengthen the women by building their trust in all staff at the labour ward. Another reason was that the counselling midwife would have to be there for the women afterwards and remain objective, which could be difficult if responsible during the birth.
The midwives considered that an important part of their work was to convey the knowledge they had obtained from the women to their colleagues at the labour ward in order to support them when en-countering women who are afraid of giving birth naturally. In addition, they wanted the organisation to make better use of their unique knowledge, for example by developing the care based on the women’s narratives.
Dedication that drains energy and requires support
The midwives described several energy-draining events at the la-bour ward. Their counselling experience made them more prone to arguing with the doctor in charge in an effort to obtain authorisation for
a CS for women with a prolonged labour. It could also make them more concerned when there was a shortage of staff, as the midwives knew the negative effects of leaving women on their own for too long. Additionally, talking to colleagues who had deviated from a woman’s birth plan, or who considered the time spent on counselling, which they called“luxury care”, as unfair to the other women in the labour ward, also drained their energy.
“We [become] some kind of advocate for these women and sometimes you have to stand up to a doctor and some strict colleagues. That is an emotionally energy-draining part of it.”
Some midwives described feeling isolated. Discussions with collea-gues were an important form of support, although they did not have much time for them. Most midwives worked alone on their counselling days and there were no regional meetings, despite their expressed wish for an opportunity to exchange experiences and develop their work. Group supervision was seen as highly beneficial and one midwife stated that“a good supervisor is worth her/his weight in gold”. Supervision helped the midwives to handle difficult cases as well as constituting an educational component that enabled them to better understand and meet the various needs of women with FOC.
Discussion
The aim of this qualitative study was to explore and describe the counselling of women with intense fear of childbirth from the view-point of midwives who provide counselling in fear of childbirth clinics in one region of Sweden. The midwives revealed that they strived to create a safe place for women to explore and discuss their fears. This striving can be related to midwives’ efforts during labour and birth to create a sanctuary-like environment where birthing women can feel safe and secure[38]. Such efforts can be a way to compensate for the previous experiences of many women who suffer from secondary FOC due to feeling unsafe during an earlier birth and experiencing the staff as uncaring [39]. Instead, maternity care providers should critically evaluate their care and attempt to identify iatrogenic factors that cause FOC in women during labour and birth[11,40,41], which also is in line with the wish from the midwives in our study to develop the maternity care based on the women’s birth experiences.
The category Providing a reliable relationship revealed the general characteristics of counselling, in particular how the structure and pro-fessional relationship between the midwife and the woman can enable emotional processing. Presenting a framework early in thefirst session is a way of demonstrating that one is a confident and responsible leader, which enables the other to relax and reflect[42]. The midwives de-scribed that when some women were initially tense or aggressive, they tried to create a calm atmosphere by means of body language. This is in line with the low arousal approach described by McDonnell[43], which is intended to help professionals create a caring environment that re-duces stress and challenging behaviour by being aware of how non-verbal cues can promote de-escalating behaviour[43]. An important part of recovery from suffering is the hope that the future will be better [44]. Although the midwives were aware of the necessity of inspiring hope in parous women that their next birth would be a better experi-ence, they were nevertheless surprised at how strongly their words and experience instilled hope in them and influenced them positively. The midwives functioned as an other-oriented hope until the women dared to sense it themselves[44].
The category Investigating previous and present fears revealed that the characteristics of the counselling content were adapted to the woman’s parity. The FOC clinics in our study accounted for 16.5% of all births in Sweden in 2015[45]. A national survey of midwife-led counselling at 43 of the 45 FOC clinics in Sweden [32] found similar counselling strategies to those described by the midwives in our study, for instance reviewing medical records together with the women, strengthening their belief in themselves and their ability to give birth, visiting the
labour ward and writing a birth plan. The midwives in our study also gave a detailed description of how and when they used such strategies. The counselling content and strategies employed by the midwives are similar to the telephone counselling provided by midwives in Australia [17,18]. In addition to the above-mentioned strategies, the key ele-ments of the counselling include emphasis on the relationship between the woman and the midwife, support to examine the origin of the women’s fear, reconcile any impact from a previous birth experience, providing information about birth options and developing strategies to facilitate a positive birth experience, irrespective of the ultimate mode of birth. These types of conversation with women suffering from FOC are described as“building childbirth resilience”[22,23,46]and have been tested in two RCTs with positive results[15,17]. Ourfindings add to the existing literature on counselling women with FOC and/or women with previous negative and traumatic births. However, FOC is a complex phenomenon [13], making it difficult to determine which strategies are most effective for each individual woman. Studies show that although FOC counselling improved women’s emotional well-being and reduced their demand for planned CS, no clear effects on women’s fear have yet been verified[24,27,29,47].
Anotherfinding worth highlighting was the experienced midwives’ counselling strategies despite differences in their formal education on FOC and its treatment. For example, the participants described the es-sence of humanistic psychology when emphasising acceptance, em-pathy and congruence as the pillars of professional relationships[48]. Additionally, the midwives mentioned common CBT strategies, such as posing questions that made the women reflect and exposing them to frightening situations (e.g., visiting the labour ward) to diminish their fear[49].
The category A strong dedication to the women revealed how re-warding the midwives found the counselling, although some aspects of it could drain their energy. It can be assumed that their dedication is noted by the women and may help the latter to build trust and hope in the midwife. The midwives described how the counselling motivated them to continue working at the FOC clinics, gaining experience and achieving professional and personal knowledge and growth, despite the sometimes demanding work situation. Moreover, energy-draining cir-cumstances were when the midwives were confronted with conflicts between different belief systems [50] and different ideologies per-taining to their care for women[51]; should they be“with the woman” or“with the institution”? The midwives described a more woman fo-cused approach in the counselling sessions where they let the individual woman’s needs guide the care. This was in contrast to their work at the labour ward, where the demands from obstetricians and other collea-gues required a more institutional approach and forced them to adhere to the general rules and guidelines of the institution in a workplace culture that hindered them from being“with the woman”[51,52]. Our results indicate a lack of woman focused models to guide midwife counselling and care for women with FOC not only during counselling but also during labour and birth. One survey of Swedish midwives[53] found that as many as one third reported some kind of burnout related to stressful work environments characterised by staff shortages and thus not related to the care of the women[53]. Regular meetings with col-leagues provide midwife counsellors with an opportunity to both share their knowledge and receive support, which together with supervision are important contributors to midwives’ workplace resilience[54,55]. Furthermore, new midwife counsellors should benefit from the ex-perience of their longer serving colleagues and not have to make the same mistakes as the latter did in their early days of their professional career. We hope that thefindings of our study can be used as compo-nents in a future educational programme for midwives who provide counselling.
Method discussion
To the authors’ knowledge, the present study is the first to explore
and describe the counselling of women with intense FOC from the viewpoint of midwives in FOC clinics in one region of Sweden. Qualitative research questions were appropriate, as both FOC and midwives’ care of women with such fear are complex issues. The three research questions were asked in the same order in all four focus group interviews. The participants were more than willing to reflect and communicate their knowledge. Thanks to the richness of the collected data, the sample size was sufficient to achieve saturation[56].
The interviewer worked at an obstetrics and gyneacology depart-ment in the region and had supervised some of the participating mid-wives. She also knew women with FOC through her profession as a psychologist, which made her familiar with FOC counselling. However, in her role as interviewer she attempted to be objective and keep an open mind in order to allow new knowledge to emerge. Previously unreported differences in midwives’ prerequisites, collaboration and thoughts about their counselling role were described. The interviewer encouraged everyone in the focus groups to be active. She also tried to make all participants feel respected for their work, especially when differences arose.
To ensure the study’s trustworthiness and validity we tried to de-scribe the whole research process in a transparent way[56,57]. The trustworthiness of a study is about the extent of the researchers’ con-fidence in their data[56]. Among other things, this concerns whether the participants’ views and experiences have been described authenti-cally with clarity and integrity[57]. As already mentioned, the same three research questions were posed by the interviewer in identical order in all four focus group interviews, while remaining open to the research topic and showing respect for the participants’ integrity. The midwives willingly reflected on and communicated their experiences and views. The entire data analysis process was conducted in ac-cordance with the method by Elo and Kyngäs[34]. The present authors were both involved in this process, participating in critical and re-flective discussions on the content and tentative categories. The theme and the categories were described with the intention of capturing the midwives' descriptions of their counselling as clearly as possible. Moreover, when interpreting qualitative researchfindings, the studied context should be considered in relation to transferability to other contexts[34]. To facilitate transferability we attempted to carefully describe the context of the study.
The strength of the present study was the midwives’ thorough de-scriptions of how they counselled women suffering from intense FOC, their own emotional reactions as well as their thoughts about what was beneficial. The limitations include the interviewer’s previous super-vision of some of the participating midwives. A few midwives might have felt observed and therefore not free to share their thoughts. On the other hand, this situation may have affected them in a positive way and created a sense of familiarity, resulting in rich, varied data. However, no differences in the data related to these potential circumstances were found. Another limitation was the use of data from only one region; however, the region in question includes nearly 20% of all women who gave birth in Sweden in 2015[37].
Conclusion
Although there are no guidelines for midwives who counsel women with FOC, the midwives in our study described similar counselling approaches and strategies. Some were general, while others were spe-cifically related to the individual woman’s parity. The findings add to existing literature on counselling for women with FOC and previous negative and traumatic births. The midwives achieved professional and personal development through their counselling experiences. However, they also described conflicts related to different ideologies of care, in-dicating a lack of woman focused care models to guide them when caring for women with FOC. The result can be used to inform the de-velopment of midwife-led interventions for women with FOC as well as in the formal education of midwives.
Recommendations for future research
Recommendations for future research are to explore more deeply how FOC counselling affects midwives. In addition, researchers should develop and test interventions based on midwife-led counselling for women with FOC. Finally, research is needed on how formal, evidence-based education of midwives enhances their knowledge, strategies, approaches and well-being as well as the impact of such education on women with intense FOC.
Declaration of interest None.
Acknowledgements
This study was funded by the Department of Research and Development NU-Hospital Group, Sweden and the Fyrbodal Research and Development Council Region Västra Götaland, Sweden. The fun-ders had no involvement in study design, collection, analysis and in-terpretation of data, in the writing of the report, and in the decision to submit the article for publication. We thank the midwives who so generously shared their knowledge.
Appendix A. Supplementary material
Supplementary data to this article can be found online athttps:// doi.org/10.1016/j.srhc.2018.12.001.
References
[1] Nieminen K, Wijma K, Johansson S, Kinberger EK, Ryding E-L, Andersson G, et al. Severe fear of childbirth indicates high perinatal costs for Swedish women giving birth to theirfirst child. Acta Obstet Gynecol Scand 2017;96(4):438–46. [2] OECD. Health at a Glance 2017: OECD Indicators. Paris; 2017.
[3] D’Alton ME, Hehir MP. Cesarean delivery rates: revisiting a 3-decades-old dogma. JAMA 2015;314(21):2238–40.
[4] Richens Y, Lavender DT, Smith DM. Fear of birth in clinical practice: a structured review of current measurement tools. Sexual Reprod Healthcare 2018;16:98–112. [5] Toohill J, Fenwick J, Gamble J, Creedy DK. Prevalence of childbirth fear in an
Australian sample of pregnant women. BMC Pregnancy Childbirth 2014;14(1):275. [6] Nilsson C, Hessman E, Sjöblom H, Dencker A, Jangsten E, Mollberg M, et al.
Definitions, measurements and prevalence of fear of childbirth: a systematic review. BMC Pregnancy and Childbirth 2018;18(1):28.
[7] Areskog B, Uddenberg N, Kjessler B. Fear of childbirth in late pregnancy. Gynecol Obstet Invest 1981;12(5):262–6.
[8] Nilsson C, Lundgren I. Women's lived experience of fear of childbirth. Midwifery 2009;25(2):e1–9.
[9] Hofberg K, Ward MR. Fear of pregnancy and childbirth. Postgrad Med J 2003;79(935):505–10. quiz 508–10.
[10] Størksen HT, Garthus-Niegel S, Vangen S, Eberhard-Gran M. The impact of previous birth experiences on maternal fear of childbirth. Acta Obstet Gynecol Scand 2013;92(3):318–24.
[11] Lukasse M, Schei B, Ryding EL. Prevalence and associated factors of fear of child-birth in six European countries. Sex Reprod Healthc 2014;5:99–106.
[12] Ayers S, Bond R, Bertullies S, Wijma K. The aetiology of post-traumatic stress fol-lowing childbirth: a meta-analysis and theoretical framework. Psychol Med 2016;46(6):1121–34.
[13] Dencker A, Nilsson C, Begley C, Jangsten E, Mollberg M, Patel H, et al. Causes and outcomes in studies of fear of childbirth: a systematic review. Women Birth 2018. [in press].
[14] Nieminen K, Andersson G, Wijma B, Ryding EL, Wijma K. Treatment of nulliparous women with severe fear of childbirth via the Internet: a feasibility study. J Psychosom Obstet Gynaecol 2016;37(2):37–43.
[15] Stoll K, Swift Emma M, Fairbrother N, Nethery E, Janssen P. A systematic review of nonpharmacological prenatal interventions for pregnancy-specific anxiety and fear of childbirth. Birth 2017;45(1):7–18.
[16] Saisto T, Salmela-Aro K, Nurmi JE, Könönen T, Halmesmäki E. A randomized controlled trial of intervention in fear of childbirth. Obstet Gynecol 2001;98(5):820–6.
[17] Toohill J, Fenwick J, Gamble J, Creedy DK, Buist A, Turkstra E, et al. A randomized controlled trial of a psycho-education intervention by midwives in reducing childbirth fear in pregnant women. Birth 2014;41(4):384–94.
[18] Fenwick J, Toohill J, Gamble J, Creedy DK, Buist A, Turkstra E, et al. Effects of a midwife psycho-education intervention to reduce childbirth fear on women’s birth outcomes and postpartum psychological wellbeing. BMC Pregnancy Childbirth 2015;15(1):284.
[19] Serçekuş P, Başkale H. Effects of antenatal education on fear of childbirth, maternal self-efficacy and parental attachment. Midwifery 2016;34:166–72.
[20] Haapio S, Kaunonen M, Arffman M, Åstedt-Kurki P. Effects of extended childbirth education by midwives on the childbirth fear offirst-time mothers: an RCT. Scand J Caring Sci 2016;31(2):293–301.
[21] Newham JJ, Wittkowski A, Hurley J, Aplin JD, Westwood M. Effects of antenatal yoga on maternal anxiety and depression: a randomized controlled trial. Depression Anxiety 2014;31(8):631–40.
[22] Gamble J, Creedy DK. A counselling model for postpartum women after distressing birth experiences. Midwifery 2009;25(2):e21–30.
[23] Gamble J, Toohill J, Creedy DK, Fenwick J. Types of conversations with women and families fearful of birth: building childbirth resilience. Women Birth 2015;28:S15. [24] Larsson B, Karlström A, Rubertsson C, Hildingsson I. The effects of counseling on
fear of childbirth. Acta Obstet Gynecol Scand 2015;94(6):629–36.
[25] Ryding EL, Persson A, Onell C, Kvist L. An evaluation of midwives' counseling of pregnant women in fear of childbirth. Acta Obstet Gynecol Scand 2003;82(1):10–7. [26] Socialstyrelsen (National Board of Health and Welfare). Indikation för kejsarsnitt på
moderns önskan [Indication for CS on the mothers’ request]; 2011. Report no.: 2011:09.
[27] Hildingsson I, Nilsson C, Karlström A, Lundgren I. A longitudinal survey of child-birth-related fear and associated factors. J Obstet Gynecol Neonatal Nursing: Clin Scholarship Care Women Childbearing Families Newborns 2011;40(5):532–43. [28] Mohlander M, Ryding EL. Samtal kan hjälpa kvinnor med förlossningsrädsla
[Counselling can help women with fear of childbirth]. Läkartidningen (J Physicians) 2013;110(12):618–20.
[29] Larsson B, Hildingsson I, Ternström E, Rubertsson C, Karlström A. Women’s ex-perience of midwife-led counselling and its influence on childbirth fear: a qualita-tive study. Women Birth 2018.
[30] Salomonsson B, Alehagen S, Wijma K. Swedish midwives’ views on severe fear of childbirth. Sexual Healthcare 2011;2(4):153–9.
[31] Salomonsson B, Wijma K, Alehagen S. Swedish midwives’ perceptions of fear of childbirth. Midwifery 2010;26(3):327–37.
[32] Larsson B, Karlström A, Rubertsson C, Hildingsson I. Counseling for childbirth fear– a national survey. Sexual Reprod Healthcare 2016;8:82–7.
[33] Barbour R. Focus groups. In: Bourgeault I, Dingwall R, de Vries R, editors. The SAGE handbook of qualitative methods in health research. London: SAGE; 2010. p. 327–52.
[34] Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs 2008;62(1):107–15.
[35] Estabrooks C, Field P, Morse J. Aggregating qualitativefindings: an approach to theory development. Qual Health Res 1994;4:503–11.
[36] Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res 2005;15(9):1277–88.
[37] Västra Götalandsregionen. Förlossningsvården i Västra Götalandsregionen 2002–2013 [Maternity care services in Västra Götalandsregionen 2002–2013]; 2015.
[38] Fahy K, Parratt J, Foureur M, Hastie C. Birth territory: a theory for midwifery practice. In: Bryar R, Sinclair M, editors. Theory for midwifery practice. Great Britain: Palgrave Macmillan; 2011.
[39] Nilsson C. The delivery room: Is it a safe place? A hermeneutic analysis of women's negative birth experiences. Sexual Reprod Healthcare 2014;5(4):199–204. [40] Liljeroth P. Rädsla inför förlossningen: ett uppenbart kliniskt problem?
Konstruktionen av förlossningsrädsla som medicinsk kategori [Fear before Delivery – An Obvious Clinical Problem? The Construction of Fear of Childbirth as a Medical Category].Åbo: Åbo Akademi; 2009.
[41] Nilsson C, Bondas T, Lundgren I. Previous birth experience in women with intense fear of childbirth. J Obstet Gynecol Neonatal Nursing: Clin Scholarship Care Women Childbearing Families Newborns 2010;39(3):298–309.
[42] Bentzen M, Hart S. Through windows of opportunity: a neuroaffective approach to child psychotherapy. London: Karnac Books; 2015.
[43] McDonnel AA. Managing aggressive behavior in care settings: understanding and applying low arousal approaches. Chichester (West Sussex): Wiley-Blackwell; 2010. [44] Howell A, Larsen D. Understanding other-oriented hope: an integral concept within
hope studies. Cham: Springer; 2015.
[45] Socialstyrelsen (National Board of Health and Welfare). Graviditeter, förlossningar och nyfödda barn– Medicinska födelseregistret [Pregnancies, deliveries and new-born infants– The Swedish Medical Birth Register]; 2015.
[46] Fenwick J, Gamble J, Creedy DK, Buist A, Turkstra E, Sneddon A, et al. Study protocol for reducing childbirth fear: a midwife-led psycho-education intervention. BMC Pregnancy Childbirth 2013;13.
[47] Larsson B, Karlström A, Rubertsson C, Ternström E, Ekdahl J, Segebladh B, et al. Birth preference in women undergoing treatment for childbirth fear: a randomised controlled trial. Women Birth 2017;30(6):460–7.
[48] Kirschenbaum H. Carl Rogers life and work: an assessment on the 100th anniversary of his birth. J Counseling Dev 2004;82(1):116–24.
[49] Willis F. Beck’s cognitive therapy: distinctive features. London: Routledge; 2009. [50] Blaaka G, Schauer Eri T. Doing midwifery between different belief systems.
Midwifery 2008;24(3):344–52.
[51] Hunter B. Conflicting ideologies as a source of emotion work in midwifery. Midwifery 2004;20(3):261–72.
[52] Davis DL, Homer CSE. Birthplace as the midwife's work place: How does place of birth impact on midwives? Women Birth 2016;29(5):407–15.
[53] Hildingsson I, Westlund K, Wiklund I. Burnout in Swedish midwives. Sexual Reprod Healthcare 2013;4(3):87–91.
[54] Hunter B, Warren L. Midwives׳ experiences of workplace resilience. Midwifery 2014;30(8):926–34.
[55] Catling CJ, Reid F, Hunter B. Australian midwives’ experiences of their workplace culture. Women Birth 2017;30(2):137–45.
[56] Polit DF. Nursing research: Generating and assessing evidence for nursing practice. 9th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2012. [57] Whittemore R, Chase SK, Mandle CL. Validity in qualitative research. Qual Health