Self-management for
Type 2 Diabetes Mellitus
Patients in Mexico –
Nurses’ Perception
A qualitative interview study
SUBJECT:Nursing science
AUTHOR: Montserrat Fernández Sánchez
SUPERVISOR:Anna Abelsson
Sammanfattning
Bakgrund: Diabetes Mellitus Typ 2 är en kronisk sjukdom som ger allvarliga långsiktiga skador. En av hörnstenarna för att kontrollera sjukdomen är patientens egenvård. För att genomföra behandlingen måste patienterna förstå vilken betydelse de har för sjukdomen.
Syfte: Syftet med denna studie är att beskriva Mexikaner sjuksköterskornas upplevelse om deras bidrag till kännedom om egenvård hos patienter med Diabetes Mellitus Typ 2 i Mexiko.
Metod: En kvalitativ design med semi-strukturerade intervjuer och en innehållanalys användes i denna studie.
Resultat: Deltagarna upplever att egenvård är av stor betydelse vid behandling av Diabetes Mellitus typ 2. Patienterna behöver kunskap och utbildning, och sjuksköterskorna är medvetna om att de är ansvariga för undervisningen. Däremot på grund av tidsbrist, otillräcklig personal samt överbelastning av patienter kan inte utbildning av patienter ske. Enligt deltagarna är patienternas engagemang och familjestöd faktorer som påverkar patienternas egenvård.
Slutsats: Deltagarna upplever att egenvård är viktigt för Diabetes Mellitus typ 2. Patienten och sjuksköterskorna har en viktigt roll vid egenvård. En personcentrerad omvårdnad kan hjälpa sjuksköterskor att tillgodose patienternas behov.
Nyckelord: Egenvård, Glykemisk kontroll, Kronisk Sjukdom, Personcentrerad Omvårdnad, Patientundervisning.
Summary
Background: Type 2 Diabetes Mellitus is a chronic disease that produces serious long-term complications. The self-management of the patient has become the cornerstones to control the disease. To carry out treatment, patients must understand the role they play at this.
Aim: This study aims to describe the Mexican nurses’ perception of their contribution to the knowledge of self-management in patients with T2DM in Mexico.
Method: A qualitative approach with semi-structured survey and a content analysis was used in this study.
Result: The participants perception is that self-management is of great importance in the treatment of T2DM. However, patients need education and knowledge, and the nurses are aware that they are responsible for that education. Nevertheless, the lack of time, inadequate nurse staffing and overwhelming number of patients, are causes that are not allowing them to educate the patients. According to the participants, the engagement of the patients and family support are factors affecting the patients’ self-management.
Conclusions: The participants perception is that self-management is crucial for T2DM patients and the nurses have an important role in it. The use of a Person-Center Cared approach can help the nurses meet the needs of the patients.
Keywords: Chronic Disease, Glycemic Control, Person-Centered Care, Patient Education, Self- Care
Table of Contents
SAMMANFATTNING ... SUMMARY ... TABLE OF CONTENTS ... INTRODUCTION ... 5 BACKGROUND ... 5 MEXICO ... 5HEALTHCARE SYSTEM IN MEXICO ... 5
NURSING PROGRAMS AND PROFESSION IN MEXICO ... 5
TYPE 2DIABETES MELLITUS ... 6
Type 2 Diabetes Mellitus in Mexico ... 6
Type 2 Diabetes Mellitus Complications ... 7
Self-Management in Patients with T2DM ... 7
THEORETICAL FRAMEWORK -PERSON-CENTERED CARE ... 8
PROBLEM FORMULATION ... 8 AIM ... 9 METHOD ... 9 DESIGN ... 9 PARTICIPANTS ... 9 SAMPLING ... 9 DATA COLLECTION ... 10 DATA ANALYSIS ... 11
ETHICAL CONSIDERATIONS AND APPROVALS ... 11
RESULT ... 13
THE ROLE OF THE NURSES IN SELF-MANAGEMENT ... 13
The Influence of the Nurses in the Education of the Patient ... 13
Factors that prevent Nurses from Educating Patients ... 15
ESSENTIAL ASPECTS IN SELF-MANAGEMENT ... 16
Patient’s Engagement ... 16
Family Support ... 17
DISCUSSION ... 19
METHOD DISCUSSION ... 19
RESULT DISCUSSION ... 20
The Influence of Nurses in the Education of the Patient ... 20
Factors that prevent Nurses from Educating Patients ... 21
Patients’ Engagement ... 21 Family Support ... 22 CONCLUSION ... 23 CLINICAL IMPLICATION ... 23 FURTHER RESEARCH ... 23 ACKNOWLEDGEMENT ... 24 REFERENCES ... 25 APPENDIX ... APPENDIX 1 ... APPENDIX 2 ... APPENDIX 3 ...
Introduction
Type 2 Diabetes Mellitus (T2DM) is a chronic and degenerative disease. Patients with T2DM in Mexico do not understand the disease and lack the necessary knowledge that T2DM self – management requires (Whittemore et al., 2019). The American Diabetes Association (2017) recommends the health staff to integrate in daily diabetes care, the needs, preferences, and the skills the patient has to carry out self-management to be able to reach a Patient – Centered Care (Rutten et al., 2018). According to Boström et al., (2014) the use of Patient – Centered Care with T2DM patients, develop the interaction between healthcare professionals and patients, which increases health outcomes in the patients.
Background
Mexico
The official name of the country is The United Mexican States. The country is located in North America and it borders with three countries, to the north with United States of America and to the south with Guatemala and Belize. Mexico is the third-largest country in Latin America, and it is composed of 31 states and a federal district. (Meyer et al., 2020). In 2018 the country’s total population was around 126 million people (The World Bank, 2020). The country is characterized by the great social differences, where there is extreme wealth but also poverty (Meyer et al., 2020). In 2016, an estimated showed that about 46.2% of Mexicans lived in poverty (CIA, 2020).
Healthcare System in Mexico
The Mexican health system is branched into two sectors, the public and the private. The public sector is divided into three types: social security for private companies, social security for governmental employees and health and assistance for those who do not belong to any of the groups named before (Squires & Juarez, 2012). The Institute of Mexican Social Security (known in Spanish as IMSS) is for Mexicans that work for private companies, the Institute of Social Security and Services for the State Workers (known in Spanish as ISSSTE) for Mexicans that are government employees and the rest of the population attend to Ministry of Health and Assistance (known in Spanish as SSA) or private institutions. As regards private health, several clinics are ranging from clinics with 5 beds to large hospitals, and prices are as variable as the market allows (Squires & Juárez, 2012).
Nursing Programs and Profession in Mexico
Nursing programs in Mexico occur in two diverse levels: technical (three years study) and bachelor (five years study). Some differences are depending on the type of study and whether the institution is free of charge or it has tuitions. However, the requirements for entering the program are the same. It is indispensable to have completed high school and to present an admission examination, including a general knowledge review and psychometric tests. Psychometric test is a scientific method used to measure the mental capabilities and behavioral style, to see if the personality and cognitive ability of a person are suitable to perform a role (Institute of
Psychometric Coaching, n.d.), in this case nursing role. Despite the two modalities, the work the nurses perform is the same irrespective of the nursing program, the only difference is wage.
The technical curriculum has subjects as preventive measures, health promotion, ethics, surgical procedures, women's care and care of the older adult. Combined with this, the students must complete a total of 960 practical hours in different health institutions (Secretaría de Educación Pública, n.d.).
The curriculum for bachelor’s program includes nursing fundamentals care, care in the human vital cycle and collective care. Each stage consists of practical and theoretical but also some optional courses into different areas which makes it easier for the student to get a deeper knowledge in the areas of greater interest (National Autonomous University of Mexico, 2020).
The profession of nursing in Mexico is regulated by the International Council of Nurses (ICN) Code of Ethics for Nurses (ICN, 2012). The Code of Ethics for Nurses describes the four fundamentals responsibilities that nurses have: to promote health, to prevent
illness, to restore health and to alleviate suffering. An important aspect of health promotion is health education, which means to inform the patients about the nature
of their disease and the risks related to their lifestyle. The purpose of the nurse is to provide support to the patients therefore the patients can change or modify their behavior (Whitehead, 2004). While providing care, the nurse should respect the individual rights, values, beliefs, sexual orientation, nationality, social status, or politics orientation.
Type 2 Diabetes Mellitus
T2DM is a metabolic disorder characterized by chronic hyperglycemia secondary to relative lack of insulin. Insulin is a hormone produced by the pancreas which regulates the glucose in the bloodstream. There are two factors to develop T2DM, genetics or environmental. Environmental means overweight and sedentarism (Chatterjee et al., 2017). The disease has increased rapidly around the world. Until the last few years T2DM was consider an adult disease, but cases in children have increased in recent years. T2DM is treated with loss of weight, adequate diet, physical activity and in necessary cases, medication (Inzucchi, 2017).
T2DM has a high rate of premature death and disability compared to those who do not have the disease. It is the fourth largest cause of death worldwide (American Diabetes Association, 2017). In 2017 was estimated that about 451 million people worldwide between 18 and 99 years suffer from the disease, of which between 90 - 95% suffer from T2DM (Gan et al., 2020).
Type 2 Diabetes Mellitus in Mexico
T2DM is a serious health problem that affects the Mexican population. According to World Health Organization (WHO, 2017) T2DM is the second leading cause of death in the country represented by the 14% of annual deaths. The Mexican Health System Report from the Organization of Economic Cooperation and Development (2016) reported that the prevalence of T2DM reached the 15,9% of population. The country is
a world leader in obesity and overweight. Around 70% of the adult population suffers either obesity or overweight which are risk factors to develop T2DM (Kolovos et al., 2019).
Type 2 Diabetes Mellitus Complications
Cardiovascular problems are the most common mortality and morbidity determinants in T2DM patients. The complications related to T2DM are divided into microvascular and macrovascular damages (Dimeglio et al., 2018; Schneider et al., 2018; Chatterjee et al., 2017). Macrovascular refers large blood vessel while microvascular refers to small blood vessels. The long-term complications associated with T2DM are lower limb amputation, kidney failure, stroke, coronary health disease, blindness, among others (Gan et al., 2020; Schneider et al., 2018; Forjuoh et al., 2014). However, the management of the disease and glycemic control are crucial to delay the long-term complications and reduce the harm for patients with T2DM (Wu et al., 2019).
Self-Management in Patients with T2DM
The good management of T2DM is achieved through physical activity, proper diet and monitoring of blood glucose, which is called self-management (Whittemore et al., 2019; Boström et al., 2014; Bartol, 2012). Patients are responsible to carry out the self-management required for daily diabetes care as T2DM is a chronic disease. The patients need support and motivation to be able to change their behaviors. For the patients to reach that improvement, they must be provided with the knowledge, tools, and skills necessary to carry out the daily self - management that the disease requires (Beck et al., 2017; Whittemore et al., 2019)
Self-management is consider an essential segment of effective diabetes management (Forjuoh et al., 2014). Self-management of the patient bind to regular controls with healthcare giver to follow up blood glucose levels, blood pressure, and body weight are important to reduce long-term complications (Sosa-Rubi et al., 2009). Diabetes self-management has proven to be cost-effective and harm reduction since it decreases the number of hospitalizations days and delays the long-term complications (Robbins et al., 2008; Beck et al., 2017).
In Mexico, patients lack the knowledge and understanding of the causes of the disease and how to manage it. This makes it difficult for them to take precautions, follow instructions, or do changes to improve their health. For this reason many patients do not know the benefits that dietary adjustments or physical activity has on health improvement or harm reduction (Whittemore et al., 2020). In 2013, was reported that in Mexico 28% of adult patients with T2DM follow all the self-management behaviors, 60% follow just one self-management behavior while 12% do not follow any self-management behavior (Weller et al., 2013).
Theoretical Framework - Person-Centered Care
The study’s framework is Person-Centered Care (PCC). According to Gothenburg Center for Person-centered Care (GPCC, 2017), PCC helps to establish a relationship between the patient, the relatives of the patient, and the health professionals involved in the treatment and caring of the patient. To ensure this GPCC (2017) has defined three concepts: partnership, patient narrative, and documentation.
Partnership is the collaboration between the person and the health care professionals.
This means, an understanding between the ability of the patient of living with a disease and the nurses’ knowledge of treatment. (GPCC, 2017). Patient narrative is an important key in PCC to get to know the story of the patient , their needs, their views, priorities, and goals. This help health professionals create a care plan that is right for that patient. The plan must be accepted by the patient (GPCC, 2017). Documentation means that the healthcare workers must document both the plan and the narrative of the patient. The documentation must update constantly, so the healthcare workers may document any changes in the situation of the patient, whether is medical or personal (GPCC, 2017).
Some healthcare professionals use PCC approach as it helps to reach an understanding between the patient, patient’s relatives and the health professionals involved in the treatment of the patient (Power et al., 2015). The principal goal in PCC is to prioritize general needs of the patient, not just medically and physically but emotionally, spiritually, psychologically, and socially. This involves seeing the context of patients, their family, the environment where the patients live and their place in the community (Ekman et al., 2011).
The use of PCC approach for T2DM patients is promising, especially in support for patients’ self-management. PCC helps the nurses to know the individual needs of the patients, patients’ health perception, physical limitations, emotional condition, and the family situation concerns of each patient (Power et al., 2015; Boström, 2014; Ekman et al., 2011). In that way, the nurses can be a support and motivation for the patients to cope with different challenges and lifestyle changes that the patients need to apply to achieve the goals of self-management (Broström, 2014). The use of a PCC approach facilitates for nurses the establishment of an agreement in conjunction with the patient since the plan is based on what the patient knows and needs, to set targets that the patient may be able to fulfil (Powers et al., 2015).
Problem Formulation
Mexico has a high rate of patients with T2DM. Self-management is important to delay the long-term complications and reduce the harm in patients with T2DM. Nurses have a very important role in education and providing information to patients. The increase in nurses’ understanding of the importance of self-management for T2DM patients and their contribution in it can result in better information and advices for T2DM. The intervention of nurses in patient’s self-management may benefit the health of the patients.
Aim
This study aims to describe the Mexican nurses’ perception of their contribution to the knowledge of self-management in patients with T2DM in Mexico.
Method
At the beginning of this study, two authors were involved. The two authors worked together until the method was developed. The results and discussions in this study are presented by only one of the authors.
Design
The authors used an inductive qualitative design with semi-structured interviews. An inductive approach allows the data to emerge from observation or interviews without the precedent of an established theory (Thomas, 2006). The purpose of qualitative studies is to study the experiences of a person on a specific phenomenon (Henricson & Billhult, 2012). In nursing, qualitative studies are used to broaden perspective on practice and research (Chen & Boore, 2009). In this case, this approach enabled the authors to explore the nurses' perspective more closely.
Participants
The criterion for inclusion in the study is nurses who work or had worked with T2DM patients at least five years at the hospital where the study was carried out.
The authors got access to the participants through the contact person who is a registered nurse and works in the hospital were the study took place. The participants that collaborated were eleven registered nurses who work in areas such as ophthalmology, nephrology, dialysis, wounds clinic, epidemiology, and endocrinology. Those are the areas where T2DM patients usually attend because of the common complications of the disease. The fact that the nurses in such areas are constantly in contact with T2DM patients allowed the authors to acquire more broad information. Of those eleven participants, one was a man and ten were women. The average age was 43 years (range 30 – 56 years). Among the eleven participants, three of them had a three years technical education, while the eight remaining had a five years bachelor education. They had an average of 14 years' experience (range 7 – 27 years).
Sampling
Before the authors arrived in Mexico, the authors contacted the contact person in Mexico via e-mail. The contact person is the registered nurse in the hospital where the study took place. The contact person required information about the aim of the study, the inclusion criterion, and informed consent letter in Spanish following the ethical principles (WMA, 2019) . The authors sent the requested information though did not specify the number of participants required. The contact person in Mexico, following the inclusion criterion sent by the authors, did a random sampling (Onwuegbuzie & Leech, 2007) informing several nurses who could be prospects and handed them the letter of informed consent, which finally the nurses that were interested signed on the
day of the interview. However, the authors cannot specify how many nurses received the informed consent letter, since that information was not provided by the contact person.
Data Collection
Data collection was done between the 20th and 29th of January 2020 at a hospital in the center of the country by semi-structured interviews. On the first day at the hospital the contact person arranged a meeting between the authors and the nurses that had agreed in taking part and given informed consent. The nurses were familiar with the aim of the study, but the nurses did not know the exact content, or the questions included in the interview. The authors informed verbally about the aim of the study and the inclusion criteria for the research to the nurses. The authors asked who was voluntary interested in taking part in the study. Some nurses did not want to participate while others wanted to get involved. From 15 nurses that were interested and matched the criteria, the authors selected eleven nurses based on the nurses’ availability of time . The authors considered that eleven interviews were sufficient therefore the data would not be too large and difficult to analyze (Onwuegbuzie & Leech, 2007) . The same day the authors and participants agreed on the day and the time the authors were to conduct the interviews.
An individual meeting with each participant took place. Before the interviews, the authors introduced themselves to the participant (Danielson, 2012). The author read the informed consent and clarified that the interviews were going to be recorded. The authors explained the aim of the study and let them ask any questions (WMA, 2019), and finally, they signed the letter of consent.
During the days the study took part, the authors conducted two interviews with a semi-structured guide (Appendix 1) per day. The interviews were conducted at the hospital in a separate room to avoid interruptions (Danielson, 2012) during the shift of the participants. The length of interviews varied from 15 to 40 minutes (means 27,5). Both authors were present throughout the interviews.
The interviews did not require an interpreter, as one of the authors is originally from Mexico. The mother tongue of the author and the participants is Spanish. After each interview, the interviewer would summarize the context of the interview to the co-author and both co-authors discussed the interviews. However, when the co-authors concluded the eleven interviews, a professional translator was contracted for the translation and transcription of the data in English. The translator was Mexican, this ensured that the translator understood the use of the language and the culture (Squires, 2009). The translator was professional but had no experience in health translations. To make sure that the translation and interpretation of the health terminology was correct, the author who speaks Spanish and English validated the translation (Squires, 2009) by listening and reading each interview.
The authors recorded the interviews with a digital voice program in a MacBook. The author had the guide with semi-structured question, and depending on the answer, in depth-questions were used like Could you explain what you meant by this? so the informant could extend the response or thought (Danielson, 2012). The authors
included some demographic questions in the interviews to get to know the academic training of the participants, years of experience, and age (Appendix 1).
Data Analysis
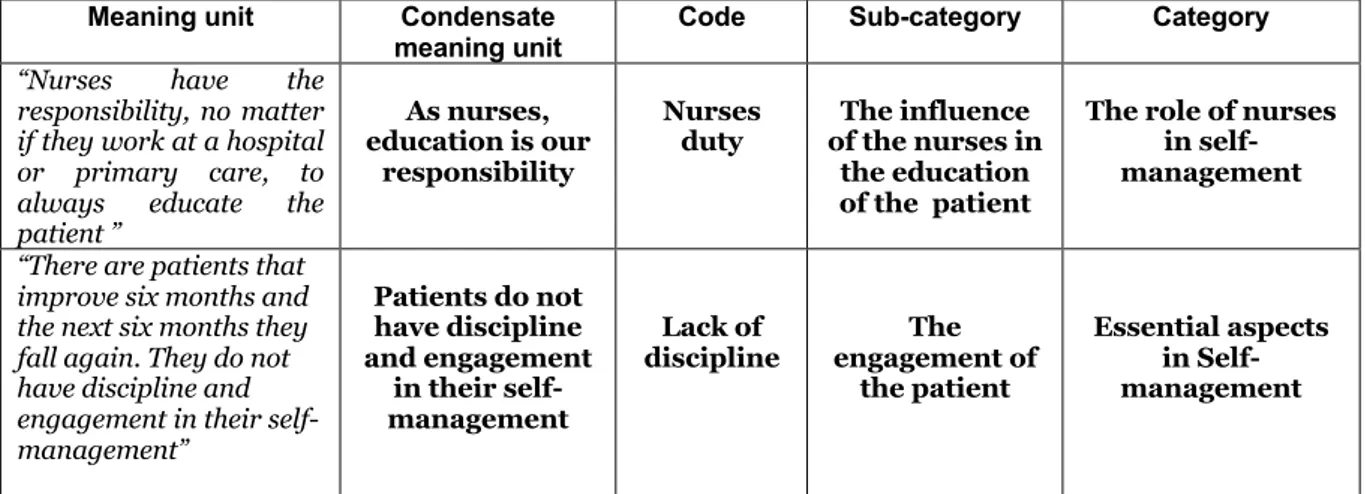
The authors used a content analysis approach (Graneheim & Lundman, 2004) to analyze the data. The authors read the interviews several times, first separately and then together to get an understanding of the text (Graneheim & Lundman, 2004). Each author read the texts and highlighted them, creating meaning units (Graneheim & Lundman, 2004). The authors discussed the highlighted text together afterwards and chose the meanings that answered the aim of the study, which turned out to be 155. The authors transferred the meaning units to a document to ease the readiness of the data.
Once having the meaning units, the authors continued with the abbreviation of the text, which provided the authors with the condensed meaning units (Graneheim & Lundman, 2004). The authors abstracted the condensed meaning units, and assigned
codes (Graneheim & Lundman, 2004).
The authors sought the similarities and differences of the codes to create categories and subcategories (Graneheim & Lundman, 2004). A total of four subcategories and two categories was generated (Table 1).
Meaning unit Condensate
meaning unit Code Sub-category Category
“Nurses have the responsibility, no matter if they work at a hospital or primary care, to always educate the patient ”
As nurses, education is our
responsibility
Nurses
duty of the nurses in The influence the education of the patient
The role of nurses in self-management
“There are patients that improve six months and the next six months they fall again. They do not have discipline and engagement in their self-management” Patients do not have discipline and engagement in their self-management Lack of
discipline engagement of The the patient
Essential aspects in Self-management
Table 1: Analyze example
Ethical Considerations and Approvals
The research in humans should follow diverse ethical principles. In qualitative research, the data is collected by interviews or observations so ethical principles such as autonomy principle, beneficence principle and justice principle (Judkins-Cohn et al., 2014; Orb et al., 2001) must be guaranteed to the participants. Autonomy
principle is the right the participants have to freely participate in a study, the right to
be informed about the study and the right to withdraw from the study at any time.
Beneficence principle focuses in principle of doing good for others and preventing
harm. Justice principle guarantees protection for the most vulnerable groups such as children, elderly or mentally ill.
The World Medical Association (WMA) developed the Declaration of Helsinki (WMA, 2019) to ensure the ethical principles for medical research involving humans including the research where human data is used. To safeguard those ethical principles the Declaration of Helsinki (WMA, 2019) has been followed in this study. The participants involvement was voluntary, the participants were informed about the aim of the study, and the right for the participants to withdraw their involvement without consequences was mentioned.
The participants signed an informed consent letter (Appendix 3).The interviews were confidential, and the authors did not save personal data following the privacy of the participant. The participants cannot be identified since the study is presented in groups not individually (WMA, 2019). Since the interviews were recorded and data transcribed to verbatim, to prevent that any person outside the study, accessed the data, all the files were saved in a computer with security password and fingerprint recognition.
However, the interviews were sent for translation with a professional translator who was not part of the study. Kjellström (2012) explains that to ensure the confidentiality of the participants, persons outside the study should not get personal information or any data that could identify the participants. When transferring the audio files to the translator, the authors transferred them one by one and no personal name was given to the files. Despite having shared the files, the translator never had personal information about the participants neither the name of the hospital or the city where the study took place to prevent the participants from being identified.
The author and supervisor carried out an ethical audit according the School of Health and Welfare in Jönköping (Appendix 2).
Result
This study aimed to describe the Mexican nurses’ perception of their contribution to the knowledge of self-management in patients with T2DM in Mexico. The data obtained from the analysis of the interviews showed the following categories and subcategories (Table 2).
Categories Sub-categories
The role of the nurses in self-management
• The influence of the nurses in the education of the patient
• Factors that prevent nurses from educating patients
Essential aspects in
Self-management • Patient’s engagement • Family support Table 2: Categories and sub-categories
The Role of the Nurses in Self-management
The perception of the participants was that self-management education for T2DM is very important. They meant that patients need knowledge about what T2DM is, how to control it and which are the long-term complications. The impression of the participants was that giving the patients the right information and knowledge provide them with the ability to carry out the proper cares of oneself. At the same time the participants insight was that the nurses need training in T2DM self-management for them to be able to transmit the information to the patients, since they were aware that the education of the patients is part of the work of nurses. However, they perceived a variety of challenges in the healthcare system that prevents them from carrying out the education of the patients.
The Influence of the Nurses in the Education of the Patient
The participants perception was that the nurses have the knowledge of what self-management for T2DM is and its importance in order to delay the long-term complications that T2DM produces. The self-management behaviors for T2DM patients that the participants mentioned are, a continuous monitoring of the blood glucose, to eat several times a day small portions, take their medications on time, physical activity at least 30 minutes a day, a healthy diet and the use of suitable footwear to prevent the occurrence of injuries on the feet .
“Self-management for patients with T2DM means how does the patient should take care of him or herself, preventing the disease from moving forward and avoiding
The participants expressed during the interviews the role that nursing has in education and prevention. They recognized that educate, inform, and teach the patients and their relatives is the responsibility of the nurses. They shared that subjects such as the education of the patient and health promotion are included in all the nursing programs as is also part of the nursing code. The nurses' perception was that the doctor diagnoses and prescribes a treatment to the patient while the nurses are in charge of educating, accompanying, supporting and caring for the patient.
“The role of the nurse is to teach and explain based on the patient’s condition which is the care he or she should have. If the patient has doubts, we should clarify them.”
P11
Nonetheless, participants mentioned that their knowledge about T2DM is delimited to what they learned during their education. What they meant was that they know and understand the pathology, but their perception was that they need a constant training in T2DM and self-management. They shared their concern, mentioning that with the problem that the disease represents in Mexico, nurses should receive specialized courses in self-management and T2DM. Thus, nurses could more effectively pass the knowledge to patients and it would generate a bigger impact.
“It is important to implement T2DM workshops for nurses, therefor nurses can train and help the patients and patients’ family”. P6
The participants perceived the need to educate the patients. The insight of the participants was that patients and their relatives lack knowledge and understanding of the disease, which results in the presence of damages in an early age. Their opinion was that the benefits of education for T2DM patients would not only be reflected in the monetary savings that it could represent for the hospital but the health of the patient. Their perception was that education for the patients would reduce the days of hospitalization and it could help delay the effects of the disease.
“Around 80% of T2DM patients do not know what glucose is, they believe it is the sugar for the coffee”. P7
Although the are no education programs implemented, the participants mentioned that when they have the opportunity, they try to provide the necessary information to T2DM patients. Their perception about those patients who have received information from the nursing staff was that the information generates impact on the patients, and it awakens an interest in their disease. They concluded that those patients who are informed and educated present a better awareness of their disease, symptoms, and care.
“I give them information and it generates and impact. I explain in depth the complications of the disease and it makes the patient more responsible and aware.”
P10
The opinion of the participants was that implementing self-management education programs for T2DM would allow nurses to carry the knowledge and education to a larger number of patients. Since the nurses could educate several patients at the same time, and invite other professionals as dieticians, endocrinologists or physiotherapists
to these talks. With the only idea of providing patients with everything they need to face life with a chronic disease.
“It is a multidisciplinary disease so it should not only be one person who follows the patients. The nutritionist and other professions also play a very important role.” P1
The participants expressed the need of support and constant education for nurses.
Factors that prevent Nurses from Educating Patients
Nevertheless, participants mentioned that even though they know it is their duty to educate and inform the patients, the circumstances they face every day such as inadequate nurse staffing, lack of time and overwhelming number of patients prevents the nurses from providing the patient with such education.
“I believe that due to lack of time. Sometimes unfortunately in our health system we miss a lot of staff, sometimes there is a lot of workload...that we forget to give the T2DM patients all the information that they need to avoid the repercussions of the
disease”. P10
At the same time, participants perceived that there is a constant rotation of nurses and doctors. And normally they do not have enough time to read the file of the patient before meeting them. They believed that it is difficult for the patient to get a proper follow up if the doctors and nurses do not have time to read the information about the health problems of the patient. Their perception was that doctors and nursing staff do not pay too much attention to the patient.
“A doctor sees you today and in 15 days it will be new doctor…because of the demand of patients they do not pay too much attention and do not follow up the
patient.” P6
Participants mentioned that they have about 20 patients per day and just 15 minutes for each patient. Their perception was that it is difficult to give the necessary information to the patients in such a short time. The lack of time makes them focus on the need of the patient at the precise time of the consultation because they do not have time for anything else.
“The long-term complications… is something that is rarely explained to the patients because we have almost 20 patients per day.” P1
The participants mentioned that around one million persons are entitled in that hospital and at least 4000 of those patients have T2DM. They perceived that they need more nursing staff to be able to give the proper attention that patients need, solve their doubts, promote the health, explain their situation, including the proper management of their medicines.
The participants believed that the lack of care and awareness of the T2DM patients about the disease is caused by variety of aspects. These aspects being the deficiency in information, follow ups and education to T2DM patients by nurses. Their impression was that it is the health system fault that the patients are missing all the knowledge they need to control their disease. Meaning that the patients do not even get an explanation about the complexity of the disease or the behavior they need to follow at home.
“Maybe it is our fault, we health workers, because we do not tell the patients the cares they have to follow at home.” P2
The perception of participants was that a multidisciplinary team would facilitate the follow-up of the patient, and help the patient have a specialized care plan. For now, the moment, the lack of time, makes the patient himself or herself seeks for information about the disease and which are the behavior they need.
Essential Aspects in Self-management
The perception of participants was that there are other important factors in self-management. These factors are independent of the education provided to the T2DM patient.
Patient’s Engagement
The perception of the participants in this study was that it is important for patients to engage with their disease and self-management. They recognized a link between patient engagement and whether they accept their T2DM or not. Their insight was that many patients do not care about their health, the effects of the disease or the proper control until they start to experience complications.
“It is until they have some complication when they change their way of thinking about the disease.” P4
The experience of the participants was that providing patients with information about T2DM and complications is important. Although their perception was that while many patients do not take the disease with the necessary seriousness, others take the information onboard, are interested in learning and follow the recommendations. The insight of the participants was that, the patients who are interested show an improvement in self-management and their health while the ones who are not usually interested worsens their health.
” Some are extremely attached to treatment, care and food while another says - I have to die for something - and they do not take it seriousness.” P11
The participants discussed how the circumstances of the patients and their intention to control their T2DM is affected by the engagement of the patient. Their perception was that the patients despite having the ability and sometimes the knowledge to take
care of themselves, they lack the interest. The opinion that participants had is that it is important that the patients have the desire to take care of themselves, because without it, still having the education and knowledge the patients will not carry out a self-management.
“They have the ability but not the desire.” P6
Moreover, the participants also mentioned their perception about how culture can influence the self-management in patients with T2DM. The insight of the participants was that the patients do not have healthy habits, as many of them drink a lot of sodas, eat fried food and they do not do physical activity. They meant that food, and healthy habits are influenced by the country’s culture.
“Mexican culture has bad habits in terms of food.” P7
During the interviews, participants commented their perception about the economic factors behind why patients with T2DM do not always look after their own self-management. This includes factors such as social status and financial resources. By this they meant that the patients sometimes do not have the financial resources to buy a glucometer or have a healthier diet, which makes it difficult for the patient to carry out a proper and adequate care to control the disease.
“They do not have the recourses to buy a glucometer” P5
The perception of the participants was that in order to carry out good self-management, the nurses need to take into account different aspects so that nurses can provide the patient with help according to the needs of the patient and possibilities. Those aspects are the economic and social situation of the patient. Which would make it easier for patients to meet their goal and follow a plan. At the same time, their impression was that through self-management education to patients, an awareness could be generated in them. The insight of the participants was that this awareness, knowledge and information could motivate the patients to do the changes that the disease required.
Family Support
The perception of the participants was that not just the physically self-cares are important, but also the emotional and psychological support for patients with T2DM. They referred that T2DM patients need psychological and emotional support for them to be able to cope living with a chronic disease. Since the disease causes many changes in their lives. They mentioned that, it is not just professional support, they also greatly benefit from family support.
“I have realized that many patients with T2DM do not accept their disease...I feel that the institutions would have to create support groups among diabetic patients and their relatives to help each other psychological based on their experiences”. P7
The perception of the participants was that family members are important when it comes to self-management in patients with T2DM. They explained that family has a huge influence on patients. The uninterested behavior from the family in the patient’s
disease influences the T2DM patient and results in them losing interest and neglecting to look after their own self-management.
“The family is a very important part of this disease, because if the support is given, the patient will succeed.” P9
Unfortunately, the experience of the participants was that not all families get involved in the care of T2DM patients and that there are shortcomings in family engagement. They considered that sometimes it is not because of lack of interest from the patient’s family, but because of lack of understanding and knowledge about the disease. According to the perception of the participants, this causes the patient to feel rejected.
“Few relatives understand the patient's condition and the patient feels that he or she does not have any help from the family.” P11
The experience of the participants in this study was that for the patients be able to manage their disease and avoid complications, the family has to work together with the patient. What they meant was that it is easier for the patient to follow recommendations such as eating healthier and exercising if the whole family commits and helps the patient. Taking into account the perception of the participants, it is difficult for the patients to implement healthy habits when there are none in their environment.
“Family does not help to follow the diet.” P2
The perception of the participants was that education programs should include the family. In this way family members may also receive the information and knowledge necessary to help the patient to carry out proper control and self-management of the disease.
Discussion
Method Discussion
According to Graneheim & Lundman (2004), the findings of a study must be reliable which is called trustworthiness. The trustworthiness of qualitative studies is based on three concepts credibility, dependability, and transferability (Graneheim & Lundman, 2004).
Credibility according Graneheim & Lundman (2004) is about asking the proper
questions to answer the aim of the study and choosing participants with different experiences. The author chose semi-structured interviews to get a deeper understanding of the perception of the nurses (Henricson & Billhult, 2012; Chen & Boore, 2009). Such information could not be obtained through surveys or closed questions, since participants would not have the opportunity to develop their ideas. To increase the credibility, the nurses in the study were of different ages and gender, with technical or bachelors’ degrees and worked in diverse areas which allowed the author to obtain a wider understanding of the perspective of the nurses in Mexico. To reach the right credibility in studies that are carried out in different languages is recommended that the interviews are carried out in the language of the participants (Squires, 2009). And when possible, without the involvement of an interpreter since interpretations, interrupt the fluid process during the data collection and important data can get lost (Squires, 2009). The interviews were sent for translation. The translator not only speaks both languages but understand the culture and context of the participants as he is Mexican, this ensures that the translation of the data is correct (Squires, 2009; Kapborg & Berterö, 202). If the authors had selected participants who could speak English, it would have reduced the number of participants and at the same time the amount of information provided by the participants would have been limited because most of the nurses did not have a good knowledge of English. An issue that the authors discussed was if the use of an interpreter instead of a translator had changed the data and results. The use of an interpreter would enable the co-author who does not speak Spanish to understand and take part in the interviews. This, perhaps, would enrich the interviews, and therefore maybe a boarder information provided by the participants. Some perceptions may have been lost, as the co-author despite being present, could not add thoughts to the interviews. The co-author despite being present in the interviews took notes based on the interviewer comments or perceptions after every interview, and this could question the trustworthiness of the study.
Dependability according to Graneheim & Lundman (2004) is about how the data is
collected and if the author chooses the right method. The data was collected through individual interviews. The authors did not have the approval from the hospital to bring a third person, in this case an interpreter. The interviews were carried out in Spanish in a separated room to avoided interruptions (Danielsson, 2012). Considering that one of the authors’ mother tongue is Spanish, the interviews were conducted in that language, which allowed for a good understanding between the author and the participants and thus obtaining the greatest possible information. The method was appropriate for the study and the author was aware of this approach although the author did not have experience interviewing participants. The length of the interviews varies from 15 to 40 minutes, this might be attributed to the inexperience of the author.
Regardless of the length’s differences in the interviews, the data produced from them was suitably for the aim of the study. In order to analyse the interviews the author used a content analysis approach. At the very first beginning, the author chose Hsieh & Shannon (2005) as a method of analysis, which is composed of three steps. Because of the inexperience analyzing texts and the few steps in that method, it was difficult for the author to understand the information. The lack of understanding of the concepts and steps would have had a repercussion on the interpretation of the data, the creation of categories and the results. That is why, finally, the author considered using Graneheim & Lundman (2004) method. This provided the author with understanding of the steps to follow to analyze the interviews, still was a challenge to create the categories and subcategories.
Transferability talks about whether the study could be replicated in another group of
people (Graneheim & Lundman, 2004). For that is necessary to describe very precisely the steps followed to produce and analysis the data, as well as the participants and questions. Based on the situation of T2DM worldwide and scientific evidence of self-management, this study could be replicable in other countries and inclusive in different chronic diseases. Nevertheless the results could vary, as this study shows the role that the patient's engagement, the culture, the social context and the family environment in the patient. Those aspects may differ in different countries.
Result Discussion
The Influence of Nurses in the Education of the Patient
The participants showed a broad knowledge of what self-management for T2DM is and the importance for patients to carry out it to prevent long-term health effects. The participants considered important to educate the patients as they recognized that self-management is one of the cornerstones for T2DM treatment. However, the perception of the participants was that it is difficult for nursing staff to educate the patients so the patients can understand the seriousness of T2DM. Which matches what Rise et al. (2013) mention, meaning that self-management is crucial to achieve a good control of T2DM.
Chrvala et al. (2016) mentions that self-management education programs help T2DM patients to get the knowledge they need to develop the skills to be able to manage their disease. In this case, the participants perception was that the patients lack the knowledge about the disease which makes it difficult for the patients to develop the necessary abilities to carry out their self-management. That kind of programs are not available in the hospital where this study took place. The participants mentioned that implementing a program like this could be useful to provide the patients with information and knowledge to develop the skills that T2DM requires.
Since patients have individual circumstances, different capacities and interests, PCC could be helpful. PCC involves the patient and the resources of the patient to develop the right care-plan for just that patient, which helps the patients to reach a proper self-management. According to Philips (2016), to reduce the harms of the disease, it is recommended to develop an individualize care to each patient. For this it is necessary to put the person in the center and let the patient takes decision about his or her care.
Factors that prevent Nurses from Educating Patients
The participants experience was that educating patients presents a challenge. The overpopulation of patients added to the inadequate nurse staffing makes it difficult for nurses to give the proper information to patients. The participants stated that it is their duty to educate patients, but at the same time they reported that doing it is difficult as they are constantly working against the clock. They explained that they usually have around 20 patients a day and the appointments have a duration of 15 minutes. This delimits the nurses to meet the needs of the patient at that moment, leaving no time to educate or inform the patient. As a result, the patients leave the hospital without understanding what T2DM is, which behaviors they should follow, how and when to take the medications and which type of follow up do they need. This has an impact in patient’s care, which in turn has an impact in the patient’s health. The participants perception was that they have a high rate of relatively young T2DM patients who attend dialysis or have gone through a bilateral amputation of lower limbs because of the lack of management of the disease. Peñarrieta- De Córdova et al. (2014) describe in their article that the overwhelming number of patients and inadequate nurse staffing causes that the patients lack the behaviors they need. In this case the insight of the participants was that the patients should receive self-management education, but the lack of time, overwhelming number of patients and inadequate nurse staffing makes the education for T2DM patients difficult.
The study shows that participants do not have the time to provide information or clarify the doubts of the patients. According to Norouzinia et al. (2015) this could rise patient’s unsatisfaction with the care they receive. Good and functional communication between participant and patient is therefore a key factor to consider when it comes to ensuring that patients feel satisfied.
If patients are not listened to, there is a risk that they will feel ignored and that will make it difficult for them to trust the nurses the next time they seek care. It is therefore important for nurses to work based on PCC (Philips, 2016). To prevent this, more nurses need to be brought in so that the workload can be reduced, and nurses can have more time with each patient.
Patients’ Engagement
Patient engagement comes down to whether a patient accepts their disease or not. The participants explained that patient’s engagement varies from patient to patient. Some patients show great interest in learning about T2DM and follow the recommendations given by the participants while others do not have that interest. The participants also told that most often, patients only become interested in their diseases once complications arise. The perception of the participants was that economic factors, as well as family support and the poor knowledge about T2DM can produce a lack of interest in the patient. According to Rodríguez (2013) there are several internal and external factors that are responsible for the lack of motivation that patients with T2DM have to carry out their self-management. Some of them can be poor understanding of T2DM and the attitude of the patients against the disease. The perception of the participants was in line with the results obtained by Rodríguez (2013).
It can be a challenge for the participants to think and act based on PCC when meeting patients who are not interested in self-management of their disease (Philips, 2016). However, it is important to try because it is part of nurses’ role to explain and give information to patients, sometimes repeatedly, in order to help them understand what is in their own best interests.
Patient engagement needs to be greater than what this study showed it to be. One way to address this and increase patient’s engagement would be education. This in order to explain to patients what T2DM is, what happens to the body and which complications can arise if the disease is not self-managed. As well as giving support to the patient and patient’s relatives to be able to maintain the life-changes the disease implies (Chrvala et al., 2016).
Family Support
The participants recognized how important the support of family members is for patients with T2DM. The participants experience was that family either help the patient to manage the disease or make it more difficult for the patient. What they mean was that when family is involved in patient’s self-management, the chances that the patient will be able to live a healthy life increase and complications can reduce. On the other hand, the lack of family support has a negative impact on the patient. Lindsay & Chandra (2012) say that in order to achieve the life-changes patients need to carry out a good self-management, the patients need support from others such as family members. Meaning that family can have a positive or negative impact in the patient’s health since they can facilitate patient’s self-management by buying the right groceries or obstruct by doing the opposite.
The study showed that the participants do not feel that the patients receive support from their family. The family does not help the patient to follow healthier behaviors because the family does not understand the disease. The patients are left feeling that their family does not understand them. A study by Avalos-Garcia et al. (2016) describes the same situation that was observed by the participants in this study – that families do not provide a high level of support to patients with T2DM.
Part of PCC is involving the family in the patient’s care. To understand the perspective of the patient and their family (Edvardsson et al., 2010). For the participants in the study, it is important to involve the family by making them be part of self-management education programs for T2DM.
Conclusion
This study aimed to describe the Mexican nurses’ perception of their contribution to the knowledge of self-management in patients with T2DM in Mexico. The participants perceive that T2DM is a big problem for the medical institutions. Patients with T2DM stands for most of the patients who use the services due to the complications. Participants attribute the situation of T2DM patients to the lack of knowledge about their disease. The study found that the participants are aware what self-management for patients with T2DM is, but they have difficulties to educate the patients in self- management. Nevertheless, the participants perception is that they do not educate the patients because of the shortage staff and overwhelming number of patients they face every day. Another important aspect that the participants mention that he engagement of the patient in self-management and the support of the relatives of the patients, play an important role in the success of the patient’s self-management.
The study shows that the participants understand how important self-management for patients with T2DM is. The opinion of the participants is that self-management education programs for T2DM patients and the relatives of the patients must be implemented at each clinic and hospital in the country. As the study shows, there are different factors that affect patient’s self-management, some of them are their economical position, family support and patient’s desire. Using a PCC approach would let the nurses understand the context of the patient in order for the nurses to support and motivate the patients for them to succeed.
Clinical Implication
The inadequate nurse staffing, the lack of time, the overwhelming number of patients and the lack of knowledge of T2DM patients, represents a challenge in the patient’s self-management. Other important factors are the engagement of the patient and the support of the family. The author considers that because of the factors mentioned, the implementation of “educational café" could be a good help for the Mexican health services. The educational café is based on the Norwegian model of health pedagogy . This will allow to educate more T2DM patients and their relatives at the same time, counteracting the lack of time or overload of T2DM patients. The core of educational café is the patient’s own capability and PPC. More specific, at educational café the T2DM patients and their relatives may meet other patients in the same situation and health professionals. The health professionals give different talks with important issues for the care and understanding of the disease. The goal is to provide T2DM patients and their relatives with the knowledge they need to live and cope with this chronic disease. Some studies show that T2DM patients that attend the educational café, experience a better well – being. Educational café shall be viewed as a complement to the traditional medical care (Altis, 2019).
Further Research
Implementing “educational café” in some hospitals could be a matter of study. A study with two groups of patients, one attending the educational café and another that does not to follow the improvement in self-management between the patients. Although, it might be suggested to make a quantitative study to measure if the education influences the results HbA1c of the T2DM patients or not.
Acknowledgement
This study has not been possible without the financial scholarship Minor Field Studies (MFS) from the Swedish International Development Cooperation Agency (SIDA). Special thanks to every person involved in this study. Above all, thank to the contact person in Mexico for her support to be able to carry out this study and to all the nurses who took part in it by sharing their experiences.
References
Altis, L. (2019). Att arbeta personcentrerad i form av lärcafé.
https://samverkan.regionsormland.se/siteassets/utbildning-och-forskning/att-arbeta-personcentrerat-med-bilagor.pdf
American Diabetes Association (2017). Older adults. Diabetes Care, 40, 99 – 104. http://doi.org/10.2337/dc17-S014
Avalos - Garcia, M., López - Ramón, C., Morales - García, M., Priego - Álvarez, R., Garrido - Pérez, S. & Cargil – Foster, N. (2016). Quality in diabetes mellitus control in primary care units in Mexico. A study of the perspectives of the patient’s family. Atención primaria, 9(1), 21 – 27. https://doi.org/10.1016/j.aprim.2016.02.012
Bartol, T. (2012). Improving the treatment experience for patients with Type 2 diabetes: Role of the nurse practitioner. Journal of the American Academy of
Nurses Practitioner, 24, 270 – 276. DOI: 10.1111/j.1745-7599.2012.00722.x
Beck, J., Greenwood, D., Blaton, L., Bollinger, S., Butcher, K., Condon, J., Cypress, M., Faulkner, P., Fischl, A., Francis, T., Kolb, L., Lavin-Tompkins, J., MacLeod, J., Maryniuk, M., Mensing, C., Orzeck, E., Pope, D., Pulizzi, J., Reed, A.,...Wang, J. (2017). 2017 National standards for diabetes self-management education and support. Diabetes care, 40, 1409 – 1419. https://doi.or.g/10.2337/dci17-0025 Broström, E., Isaksson, U., Lundman, B., Lehuluante, A. & Hörnsten, Å. (2014).
Patient- centred care in type 2 diabetes – an altered professional role for diabetes specialist nurses. Scandinavian Journal of Caring Sciences, 28(4), 675 – 682. https://doi.org/10.1111/scs.12092
CIA (2020). North America –Mexico. https://www.cia.gov/library/publications/the-world-factbook/geos/mx.html
Chatterjee, S., Khunti, K. & Davies, M. (2017). Type 2 Diabetes. The lancet, 389, 2239– 2251. http://dx.doi.org/10.1016/S0140-6736(17)30058-2
Chen, H & Boore, J. (2009). Translation and back-translation in qualitative nursing research: methodological review. Journal of clinical nursing, 19, 234 – 239. http://doi.org/10.1111/j.1365-2702.2009.02896.x
Chrvala, C., Sherr, D. & Lipman, R. (2016). Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic control. Patient education and counseling, 99(6), 926 – 943. https://doi.org/10.1016/j.pec.2015.11.003
Danielson, E. (2012). Kvalitativ forskningsintervju. M. Henricson (Red.).
Vetenskaplig teori o metod- från idé till examination inom omvårdnad (s. 163
DiMeglio, L., Evans-Molina., C & Oram, R. (2018). Type 1 Diabetes. The lancet,
391(10138), 2449 – 2462 https://doi.org/10.1016/S0140-6736(18)31320-5
Edvardsson, D., Fetherstonhaugh, D. & Nay, R. (2010). Promoting a continuation of self and normality: person-centred care as described by people with dementia, their family members and aged care staff. Journal of clinical nursing, 19(17-18), 2611 – 2618. https://doi.org/10.1111/j.1365-2702.2009.03143.x
Ekman, I., Swedberg, K., Taft, C., Lindseth, A., Norberg, A., Brink, E., Carlsson, E., Dahlin-Ivanoff, S., Johansson, I-L., Kjellgren, K., Lindén, E., Öhlén, J., Olsson, L-E., Rosén, H., Rydmark, M. & Sunnerhagen, K. (2011). Person-Centered Care – Ready for Prime Time. European Journal of Cardiovascular Nursing, 10(4), 248 – 251. https://doi.org/10.1016/j.ejcnurse.2011.06.008
Gan, Q., Wang, J., Hu, J., Guanhua, L., Xiong, H., Peng, C., Zheng, S. & Huang, Q. (2020). The role of diosgenin in diabetes and diabetic complications. Journal
of steroid biochemistry and molecular biology, 198.
https://doi.org/10.1016/j.jsbmb.2019.105575
Gothenburg Center for Person-Centered Care (2017). Person-centered care. https://gpcc.gu.se/english/about-gpcc/person---centred-care
Graneheim, U.H. & Lundman, B. (2003). Qualitative content analysis in nursing research: concepts, procedures, and measures to achieve trustworthiness.
Nurse education today, 24, 105 – 112.
http://doi.org/10.1016/j.nedt.2003.10.001
Henricson, M. & Billhult, A. (2012). Kvalitativ design. M. Henricson (Red.),
Vetenskaplig teori och metod, från idé till examination inom omvårdnad
(s.129 – 137). Studentlitteratur.
Hsieh, H-F. & Shannon, S. (2004). Three approaches to qualitative content analysis.
Qualitative health research, 15(9), 1277 – 1288.
http://doi.org/10.1177/1049732305276687
Institute of psychometric coaching (n.d.). What are psychometric tests?
https://www.psychometricinstitute.com.au/psychometric-guide/introduction_to_psychometric_tests.html
ICN Code of Ethics for Nurses. International Council of Nurses.
https://www.icn.ch/sites/default/files/inline-files/2012_ICN_Codeofethicsfornurses_%20eng.pdf
Inzucchi, S. (2017). Is it time to change the type 2 diabetes paradigm? No! Metformin should remain the foundation therapy for type 2 diabetes. Diabetes care, 40(8), 1128 – 1132. https://doi.org/10.2337/dc16-2372
Judkins-Cohn, T., Kielwasser-Withrow, K., Owen, M. & Ward, J. (2014). Ethical Principles of Informed Consent: Exploring Nurses’ Dual Role of Care Provider and Researcher. The journal of continuing Education in Nursing, 45(1), 35 – 42. doi:10.3928/00220124-20131223-03
Kapborg, I. & Berterö, C. (2002) Using an interpreter in qualitative interviews: does it threaten validity? Nursing Inquiry, 9(1), 52 – 56. doi:10.1046/j.1440-1800.2002.00127.x
Kjellström, S. (2012). Forskningsetik. Henricson, M. (Red.). Vetenskaplig teori och
metod, från idé till examination inom omvårdnad (s.69 - 92).
Studentlitteratur.
Kolovos, S., Jimenez-Moreno, A., Pinedo-Villanueva, R., Cassidy, S. & Zavala, G. Association of sleep, screen time and physical activity with overweight and obesity in Mexico. Eat weight disorder, 2019. https://doi.org/10.1007/s40519-019-00841-2
Lindsay, M. & Chandra, O. (2012). Family support, medication adherence, and glycemic control among adults with type 2 diabetes. Diabetes care, 35(6), 1239 – 1245. https://doi.org/10.2337/dc11-2103
Meyer, M., Willey, G., Parkes, H., Palerm, A., Griffin, E., Cline, H. & Bernstein, M.
(2020). Mexico. Encyclopedia Britannica.
https://www.britannica.com/place/Mexico/Drainage
National Autonomous University of Mexico (2020). National school of nursing and
obstetrics. Bachelor's in nursing.
http://www.eneo.unam.mx/english/pdf/Bachelor%20in%20Nursing.pdf Norouzinia, R., Aghabarari, M., Shiri, M., Karimi, M. & Samami, E. (2015)
Communication barriers perceived by nurses and patients. Global Journal of
health science, 8(6), 65-74. http://dx.doi.org/10.5539/gjhs.v8n6p65
Onwuegbuzie, A. & Leech, N. (2007). A call for Qualitative Power Analyses. Quality &
Quantity, 41(1), 105 – 121. DOI:10.1007/s11135-005-1098-1
Orb, A., Eisenhauer, L. & Wynaden, D. (2001). Ethics in Qualitative Research. Journal
of Nursing Scholarship, 33(1), 93 – 96
Organization of Economic Cooperation and Development (2016), OECD Reviews of
Health Systems: Mexico 2016. Paris, France: OECD Publishing
https://www.oecd.org/health/health-systems/OECD-Reviews-of-Health-Systems-Mexico-2016-Assessment-and-recommendations-English.pdf
Peñarrieta-De Córdova, M., Castañeda-Hidalgo, H., Acevedo-Porras, G., Rangel-Torres, S., González-Salinas, F. & Garza-Hernández, R. (2014). Role and working conditions of hospital nurse managers: A binational study from Peru and Mexico. Journal of hospital administration, 3(3), 91-99 https://doi.org/10.5430/jha.v3n3p91
Philips, A. (2016). Optimizing the person-centred management of type 2 diabetes.
British journal of nursing, 25(10), 535 – 538.