CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports78(2021)411–416ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
j o ur na l h o m e p a g e :w w w . c a s e r e p o r t s . c o m
First
bilateral
non-invasive
follicular
thyroid
neoplasm
with
papillary-like
nuclear
features
(NIFTP)
co-occurring
with
bilateral
papillary
thyroid
microcarcinoma.
Case
report
and
literature
review
Mohamed
S.
Al
Hassan
a,
Walid
El
Ansari
b,c,d,∗,
Abdallah
Elshafeey
e,
Mahir
Petkar
f,
Abdelrahman
Abdelaal
aaDepartmentofGeneralSurgery,HamadGeneralHospital,Doha,Qatar bDepartmentofSurgery,HamadGeneralHospital,Doha,Qatar cCollegeofMedicine,QatarUniversity,Doha,Qatar
dSchoolofHealthandEducation,UniversityofSkövde,Skövde,Sweden eWeillCornellMedicine–Qatar,Doha,Qatar
fDepartmentofLaboratoryMedicine&Pathology,HamadGeneralHospital,Doha,Qatar
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received28November2020 Accepted30November2020 Availableonline2December2020 Keywords:
NIFTP Casereport Thyroidnodule Management
Papillarythyroidmicrocarcinoma Bilateral
a
b
s
t
r
a
c
t
INTRODUCTION:Non-invasivefollicularthyroidneoplasmwithpapillary-likefeatures(NIFTP)isarecently characterizedlesionwithverylowmalignantpotential.Thishasallowedforlessaggressivemanagement ofthistumorsubtype.Papillarythyroidcarcinoma(PTC)hasmalignantpotentialandrequiresdifferent considerationsinmanagement.
PRESENTATIONOFCASE:A33-year-oldwomanpresentedtoourThyroidSurgeryClinicwithaleftneck swellingslowlyenlargingover4years,andrecentright-sidedneckpain.Neckultrasoundandfineneedle aspirationforcytologyfoundbilateralthyroidnodules,labelledas‘follicularlesionofundetermined significance’(FLUS).Finalpathologyreportaftertotalthyroidectomyidentifiedfourdistincttumors: bilateralNIFTPlesionsandbilateralpapillarymicrocarcinomas.
DISCUSSION:ManagementofNIFTPcomprisespartialortotalthyroidectomywithoutfurther interven-tion.ManagementofPTCisthesamebutwiththepossibleadditionofradioactive ablationdueto theincreasedmalignantpotential.ThisisthefirstreportofbilateralNIFTPlesionsandbilateral pap-illarymicrocarcinomasco-occurringtogetherinthesamepatient,somanagementwaschallenging.The decisionwasmadetogivethepatientlowdoseradioactiveiodineablationandcontinuemonitoring. Ultrasoundoftheneckfollowup6monthslatershowednoresidualthyroidtissueorlocalrecurrence. CONCLUSION:Althoughrare,NIFTPcanco-occurwithPTC.BilateralNIFTPwithbilateralPTCisextremely rare.Surgeonsandpathologistsneedtobeawareofthisrareentitythatcanco-occurinboththyroid lobes.Totalthyroidectomyisthedefinitivetreatment.Post-surgerysurveillanceisimportantandfollow upneedstobewatchfulforanyrecurrenceormetastasis.
©2020TheAuthor(s).PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Thyroid canceris anincreasingly important due tothe dra-maticincreaseindiagnosedcasesduringthelast30years[1].Even thoughthe5-yearsurvivalrateis97.8%[1],thyroidcancerhas significantimpact,whereintheUSAalone,$1.6billionhasbeen spentonthemanagementofthyroidcancerduring1985–2014[2]. Extensiveeffortshavebeenmadetoappropriatelyclassifythyroid tumorsbasedontheirpotentialformalignancyinorderto man-agebenignlesionslessaggressively.In2017,theWHOreleaseda
∗ Correspondingauthorat:DepartmentofSurgery,HamadGeneralHospital,Doha, Qatar.
E-mailaddress:welansari9@gmail.com(W.ElAnsari).
newclassificationforthyroidtumorstofurtherclassifypreviously misunderstoodlesions[3].
Mostwelldifferentiatedthyroidtumorscanbeclassifiedinto thebroadfollicularandpapillarycategoriesbasedonthe histo-logicalcharacteristics.Folliculartumors(10–15%prevalenceofall thyroidcancers)comprisefollicularcellslinedbycuboidal epithe-liumandarefurthercharacterizedbasedontheirinvasivebehavior [4,5].Folliculartumorsthatdonotinvadethecapsulearefollicular adenomas,andthosethatshowevidenceofinvasionarefollicular carcinomas[4].Papillarythyroidcancer(PTC,themostcommon typeofthyroidtumors)isanepithelialtypetumor,carriesthebest prognosis,andisdifferentiatedfromthefollicularsubtypebyits uniquenuclearfeatures[5].
A very unique and recently characterized thyroid lesion is thenon-invasivefollicular thyroidneoplasmwithpapillary-like
https://doi.org/10.1016/j.ijscr.2020.11.159
2210-2612/©2020TheAuthor(s).PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
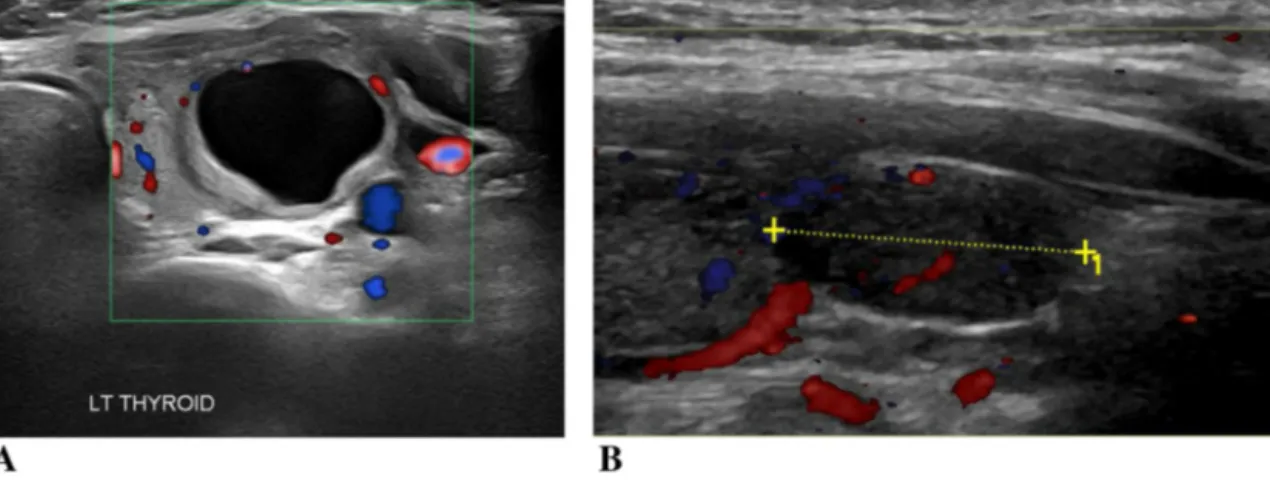
Fig.1. USoftheleftthyroidnodule.
features(NIFTP).Thistypehasdistincthistopathologicaland clin-icalcharacteristics.Formerlyknownasnoninvasiveencapsulated follicularvariantofpapillarythyroidcarcinoma,NIFTPbehaves dif-ferentlyfromtheclassicPTC.Mostimportantly,NIFTPhasavery indolentcourseandrarelyexhibitsmalignantpotential[6],making itimportanttodistinguishfromothermoremalignanttumors.A studyof108patientsshowedthatNIFTPexhibitednorecurrence 1–10yearsaftersimplelobectomy[7].DiagnosisofNIFTPismade aftercompleteresectionandconfirmationofcriteriasuchasthefull encapsulationofthetumor,nuclearfeatureofPTC,follicularpattern ofgrowthwithnopsammomabodies,nocapsularorvascular inva-sion,andnoevidenceofnecrosis[7].Moleculartestingisamajor partofthediagnosisduetotheuniquegeneticmakeupofNIFTP thatincludesmarkerslikeanactivatingmutationinoneoftheRAS genes(NRASmostcommon,36–67%),PAX8-PARGrearrangement (4–22%),andTHADAfusions(22%)[8]
Wepresentapatientwithaleftsidedneckswellingthat,after totalthyroidectomy,wasfoundtohavebilateralNIFTPsinaddition tobilateralpapillarythyroidmicrocarcinoma.Tothebestofour knowledge,thisisthefirstcasereportofthisnature.Wereport thiscaseinlinewiththeupdatedconsensus-basedsurgicalcase report(SCARE)guidelines[9].
2. Casepresentation
A33-year-oldEgyptianfemalepatientpresentedatourThyroid SurgeryOutpatientClinicatHamadGeneralHospitalinDoha,Qatar witha4-yearhistoryofleftneckswelling.Shealsocomplainedof arecentfeelingofsomediscomfortandneckpainontherightside, butnochangeofvoice.Herpastmedical,socialandfamilyhistory wereunremarkable.Shehadnohistoryofchronicmedical condi-tionsandheronlysurgicalhistorywasalowersegmentcesarian sectionafewmonthsbeforehercurrentindexpresentation.She didnotsmoke,neverconsumedalcoholandwasnotonlong-term medications.Therewasnofamilyhistoryofthyroidcancer,and nopasthistoryofneckirradiation.Physicalexaminationrevealed aleftthyroidlobeenlargement,about3×3cm,thatmovedwith swallowing.Therightthyroidlobewasnotpalpable.Therestof thephysicalexaminationwasunremarkable.
BloodworkuponpresentationshowednormalTSHandfreeT3 andT4.Intialultrasound(US)ofthethyroidglandatasecondary hospitalshowedenlargementoftheleftlobe(5.3×2.2×3.5cm),as wellasacomplexnodule(4.2×1.8×2.2cm)thatoccupiedmostof theleftlobe,containingacystwithathickirregularwallandclear contents withperipheralvascularityandnointernalvascularity. Bothsubmandibularandparotidglandswereunremarkable,and therewasnocervicallymphadenopathy.
Fig.2. LeftlobeNIFTPwithwellcircumscribedandthincapsule.HandEx2.
ShewasreferredtoourThyroidSurgeryOutpatientClinicat thetertiaryhospitalforUSguidedfine-needleaspirationfor cytol-ogy(FNAC)(Fig.1).WeundertookFNACbiopsyofthis leftlobe nodule.DuringtheFNACprocedure,theUSshowedanothersolid noduleintherightlobethatwasalsoaspirated.Theaspiratefrom bothnodulesshowedhighcellularitycomprisedoffollicularcells arrangedin analteredarchitectural background,suggestingthe histopathologicdiagnosisofthetwonodulesas‘follicularlesionof undeterminedsignificance’(FLUS).Thecasewasdiscussedatour thyroidmulti-disciplinarymeeting(MDT)andthedecisionwasto undertaketotalthyroidectomy.Thesurgerywasundertakenbyan experiencedthyroidsurgeonandwasuneventful.
The thyroidectomy specimen weighed 23 gm. The right lobemeasured4×1.5×1.5cm, whereas theleftlobemeasured 5×2.5×2.5cm.Therewasawelldemarcatednoduleintheright lobemeasuring1.3cminmaximumdimensionandasimilar,but larger,thinlyencapsulatednodule,measuring3cminmaximum dimension,intheleftlobe.Microscopically,bothnodulesdisplayed featuresofNIFTP.Theneoplasmshadafolliculararchitecturewith lesionalcellsexhibitingnuclearclearingandprominentgrooves. HBME1immunostainwasstrongly anddiffusely positive, while stainingforBRafV600Ewasnegative.Inaddition,thereweretwo separatefociofpapillarymicrocarcinoma,locatedintherightand leftlobes,measuring0.8cmand0.3cmrespectively, demonstrat-ingtypicalnuclearcharacteristics(nuclear clearing,overlapping andgrooves)withareasofpapillarymorphology.Background lym-phocytic thyroiditisand adenomatoidnodules were also noted (Figs.2–6).
CASE
REPORT
–
OPEN
ACCESS
M.S.AlHassanetal. InternationalJournalofSurgeryCaseReports78(2021)411–416
Fig.3.RightlobeNIFTPwithcharacteristicwellcircumscribedarchitecture.Hand Ex2.
Fig.4.Papillarymicrocarcinomawithtumorcellsshowingtypicalnuclearfeatures includingoverlapping,clearingandgrooves.HandEx20.
Fig.5.NIFTPdemonstratingstrongHBME1staining.
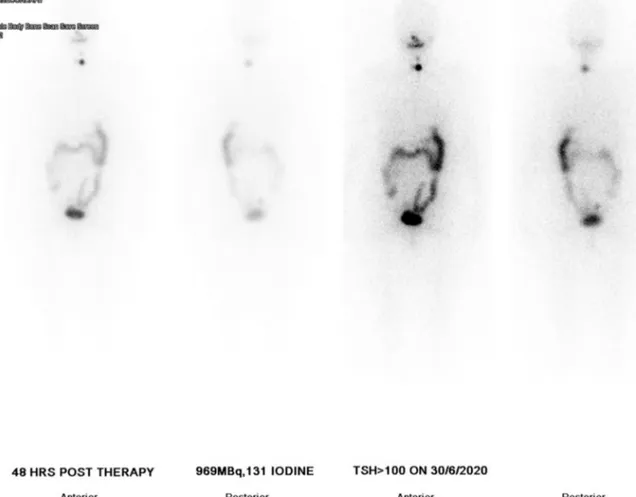
Twoweeksafterthesurgery,non-stimulatedthyroglobulin(TG) was <0.1ng/mL, and TGantibodies waspositive (133.5 IU/mL). Hence,MDT recommendedlow-doseradioactiveiodinetherapy (oralintakeof869MBqofradioactiveI-131capsule),followedby wholebodyscanwhichshowedasmallamountofactivityinthe thyroid bed.Therewasnoevidenceofdistantabnormaluptake (Fig.7). Threemonthslater, theblood test showed TGlevel of 0.1ng/mL,andtheTGantibodiesexhibitedadropfrom133IU/mL
Fig.6. NegativeBrafV600EimmunostainintheNIFTP.
to36.9IU/mL.Thepatientwasputonsuppressivelevothyroxine therapy,andscheduledforfollowupevery6monthsbyUSofthe neck,andthyroglobulintumormarkers.Themostrecentfollowup US6monthslatershowednodefiniteresidualthyroidtissueor localrecurrence.
3. Discussion
Tothebestof ourknowledge,this is thefirstreportedcase ofbilateralNIFTPswithsimultaneousbilateralpapillarythyroid microcarcinoma.Hence,wewereunabletofindothersimilar pub-lishedcaseswithwhichwecandirectlycompareourfindingswith. Weprovidealiteraturereviewofthe4publishedcasereportsof NIFTP.DespitethataremanycasesofNIFTPreportedinliterature aspartofbiggertrialsorsystematicreviewoftrials,wereportthese 4casesalongwithours,duetotheuniquefeaturesofeachofthem. Oneofthecasesoccurredina10-year-oldchild,twocaseshad spin-dlecellmetaplasiawithinthelesion,andlastly,oneofthelesions occurredwithinaHurthlecelladenoma(Table1).
Todate,therehavebeen1430reportedcasesofunilateralNIFTP [7],buttothebestofourknowledge,noreportsofbilateralNIFTP.In addition,noneofthese1430reportedcaseshadassociated micro-carcinoma,and none had bilateralassociated microcarcinomas. Hencethecurrentcaseisveryuniqueandpresentssomechallenges inthemanagementthathavenotbeendescribedbefore.
NIFTPhasbeenrecentlycharacterizedasathyroidtumorthat exhibitsanindolentbehavior.Such characterizationallows clin-iciansto approach NIFTP in a less aggressive way than before, limitingtheneedforextensivetherapyandunnecessarysideeffects associated with aggressive measures [6]. A recent review that examined11NIFTPstudieswithlargepatientpopulationsobserved nodeathsduetoNIFTPandonly1caseofpulmonarymetastasis[7]. Giventhemortalityandmetastaticevidencethatthisreview pro-vided,theparadigmformanagementofNIFTPshiftedconsiderably andnowcentersaroundsimplelobectomyfortheNIFTPinsteadof addingradioactiveiodineaswell[6].
Intermsofpresentation,ourreviewoftheliterature(Table1) shows that mostNIFTP casespresented asymptomatically with eitherafullyenlargedthyroidorenlargementofasinglelobe.We areinagreement,ourpatientpresentedwithleftthyroid enlarge-mentwhichcanbeconsideredaclassicalpresentationofthyroid nodules.However,thetablealsoshowsthatonepatienthadan unusualpresentation[10],withupperextremitynumbnesswhich isnotnormallyasymptomofthyroidnodulesunlesstheyinvolve theparathyroidglandand influencecalciumhomeostasis. How-ever,ourpatientalsocomplainedofrecentrightsidedneckpain.
T
–
OPEN
A
CCESS
International Journal of Surgery Case Reports 78 (2021) 411–416Abdou[12]Egypt2020 10 F UnilateralRt Enlarged thyroid observedby mother TwoNIFTP lesionsonR side
N Euthyroid Twosuspicious
nodulesonRt side Sheetsof follicular epithelialcells Total thyroidectomy No 12m,noRor Mt
Pigac[16]Croatia2018 42 F b Slightly
enlarged tenderthyroid NIFTPlesion withina Hurthlecell adenoma
N Euthyroid Enlargedboth
lobes, hypoechoic structureinRt lobe
Hurthlecells Rt
hemithy-roidectomy switchedto total thyroidectomy
No N
AlRasheed[10]USA2017 76 F a Upper
extremity numbness. Multinodular goiter NIFTPwith spindlecell metaplasia N Euthyroid Multinodular goiter, Dominant noduleinRt upperpole.No microcalcifica-tions Follicularand Hurthlecells Total thyroidectomy No 2mnoRorMt
Arnoux[11]Switzerland2017 37 F UnilateralL Largenodulein
Lthyroid enlargingsince 2005 NIFTPwith focalspindle cellmetaplasia N Euthyroid Isoechogenic noduleinL thyroidlobe FNA12years earliershowed benignfindings L lobo-isthmectomy No N
Duetospacelimitations,onlythefirstauthoriscited;aPatienthadmultiplenodulesthroughoutthethyroid,butthecasereportonlycommentedontheNIFTPlesion;bOnultrasoundtwolesionswerefound,oneontheright andoneontheleftbutthecasereportdidnotcommentontheleft-sidedlesion;FNAC:FineNeedleAspirationforCytology;G:Gender;L:Left;Mt:metastasis;m:months;N:no;NIFTP:non-invasivefollicularthyroidneoplasm withpapillary-likefeatures;R:recurrence;Rt:Right;TFT:ThyroidFunctionTests.
CASE
REPORT
–
OPEN
ACCESS
M.S.AlHassanetal. InternationalJournalofSurgeryCaseReports78(2021)411–416
Fig.7.Postlow-doseradioactiveiodinetherapywholebodyscanshowingsmallamountofactivityinthethyroidbed.
Asregardstothyroidinvolvement,Table1depictssome varia-tionintermsoftheextentoftheinvolvementofthethyroid.While onecasehadmultinodularenlargementofthegland[10],others [11,12]presentedwithenlargementofonlyonehalfofthegland. Givensuchanextentofvariation,thereseemstobenofixedsetof physicalexaminationfindingsorpresentationthatcanprovidean indicationtothesurgicalteamastonatureofthelesions.
In terms of investigations, thyroid function tests (TFTs) are required todeterminetheactivityofthethyroidgland.Table1 showsthatinallthecasesreviewed,thepatientswereeuthyroid indicatingthatthenoduleswerenotactive[10–12,16].Wearein agreement, ourpatientwaseuthyroid,althoughthepatienthad deliveredaroundonemonthbeforethefirstsetofTFTswhichcould causeunexpectedendocrinefluctuations.Suchfluctuationshave beenshowntooccurinaround5%ofwomenfollowingdelivery [13].
Asfor imaging,Table1 depictsthat theUSfindings differed considerablybetweencasesthatourreviewidentified.The pub-lished caseswereviewedexhibitedvariableechogenicityonUS scan. Suchhypoechoic,hyperechoicorisoechogenicUS findings [11,14,16]aresupportedbyothers whodescribedNIFTPlesions aswell-circumscribedwithwidelyvariableechogenicity[14].In addition,initialUSonlyshowedtheleftsidedcomplexcystic nod-ule;onlyonUSguidedFNAwasthesecondnoduleontheright sideidentifiedandaspirated.USfindingsareoperatordependent, andtherecouldbesomelimitationsofUSwhenemployedforthe assessmentofthyroidnodules,wherenodulesthataretoosmall mightnotbeidentifiedwithgreataccuracy.HenceUSfindingsof thethyroidshouldbeinterpretedwithcautionbecauseitdoesnot haveperfectsensitivity[15].
AsfortheUSguidedFNAC,Table1showsthatallthecasesthat ourreviewidentifiedexhibitedfollicularcellsinabackgroundof colloidorbenigncells.SomeofthestudiesalsofoundHurthlecells [10,16].Inourcase,FNACofbothrightandleftnodulesshowedan abundanceoffollicularcellsinanalteredarchitecturesuggesting FLUS.AlimitationofFNACisthatitdoesnotprovideinformation regardinginvasionofthecapsulewhichisessentialinthediagnosis ofNIFTP[6].
Intermsofmanagement,basedonourcombinedUSandFNAC results,afterMDTmeeting,thedecisionwastoundertaketotal thy-roidectomy.Thiswasundertakenbyanexperiencedsurgeon.The finalhistopathologicexaminationfoundthatthetwomasses iden-tifiedonimagingwerebothNIFTP,andalsoreportedtwoadditional smallmassesofpapillarymicrocarcinomas.
Such presence of four separate tumors presented a huge dilemmatotheteamastothebestwayforwardwiththispatient’s management.Ontheonehand,NIFTPisestablishedasarelatively benignlesionwithalmostnochanceofrecurrenceafterresection. Table1showsthatalltheNIFTPcasesthatourreviewidentified weremanagedbysimpleresectionoftheinvolvedthyroidgland andsubsequentfollowup.Ontheotherhand,contrarytoallthe othercasesinTable1,ourpatienthadtwoNIFTPsandtwo papil-larymicrocarcinomas.Inaddition,thepatienthadelevatedtumor markerthyroglobulinsuggestingsomemalignantpotential, prob-ablyof the papillarymicrocarcinomas.The decision, after MDT meeting,wastogivethepatientlowdoseradioactiveiodine abla-tion,bothasadiagnosticmeasure(toidentifyanyresidualthyroid tissue)andalsotherapeutic.
In terms of recurrence and metastasis, US follow up of our patientat6monthsshowednoevidenceofeither.Thepatient, how-ever,remainsbeingmonitoredevery6monthsinordertoassess
notexcludetheco-occurrenceofotherpapillarymicrocarcinomas lesions. Conflictsofinterest Nothingtodeclare. Sourcesoffunding Nothingtodeclare. Ethicalapproval
ApprovedbyMedicalResearchCenter,HamadMedical Corpo-rationreferencenumber(MRC-04-20-1090).
Consent
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereportandaccompanyingimages.Acopy ofthewrittenconsentisavailableforreviewbytheEditor-in-Chief ofthisjournalonrequest.
Authorcontribution
Mohamed S. Al Hassan: Conceptualization, Data curation,
Investigation,Writing -review &editing. WalidElAnsari: Con-ceptualization,Datacuration,Investigation,Methodology,Project administration,Writing-originaldraft,Writing-review&editing.
Abdallah Elshafeey: Data curation,Investigation, Methodology,
Writing-originaldraft,Writing-review&editing.MahirPetkar:
Laboratorydata,Writing-review&editing.Abdelrahman
Abde-laal:Datacuration,Writing-review&editing.
Allauthorscriticallyreviewed,revisedandcontributedtothe finalarticle.Allauthorsreadandapprovedthefinalmanuscript.
Registrationofresearchstudies
researchregistry6272 available at: https://www. researchregistry.com/browse-the-registry#home/
registrationdetails/5fba4ae0d3b0b1001e41b262/.
[1]Q.T.Nguyen,E.J.Lee,M.G.Huang,Y.I.Park,A.Khullar,R.A.Plodkowski, Diagnosisandtreatmentofpatientswiththyroidcancer,Am.HealthDrug Benefits8(2015)30–40.
[2]C.C.Lubitz,C.Y.Kong,P.M.McMahon,G.H.Daniels,Y.Chen,K.P. Economopoulos,G.S.Gazelle,M.C.Weinstein,Annualfinancialimpactof well-differentiatedthyroidcancercareintheUnitedStates,Cancer120 (2014)1345–1352.
[3]D.Sanita`,E.Al,WHOClassificationofTumoursofEndocrineOrgans, InternationalAgencyforResearchOnCancerPP-Lyon,2017.
[4]D.Ashorobi,P.P.Lopez,FollicularThyroidCancer,StatPearlsPublishing, TreasureIsland(FL),2020[Updated2020Aug26].StatPearls[Internet]. January.
[5]F.Limaiem,A.Rehman,T.Mazzoni,PapillaryThyroidCarcinoma,StatPearls Publishing,TreasureIsland(FL),2020[Updated2020Oct16].StatPearls [Internet].January.
[6]Y.E.Nikiforov,R.R.Seethala,G.Tallini,Z.W.Baloch,F.Basolo,L.D.R.Thompson, J.A.Barletta,B.M.Wenig,A.AlGhuzlan,K.Kakudo,T.J.Giordano,V.A.Alves,E. Khanafshar,S.L.Asa,A.K.El-Naggar,W.E.Gooding,S.P.Hodak,R.V.Lloyd,G. Maytal,O.Mete,M.N.Nikiforova,V.Nosé,M.Papotti,D.N.Poller,P.M.Sadow, A.S.Tischler,R.M.Tuttle,K.B.Wall,V.A.LiVolsi,G.W.Randolph,R.A.Ghossein, Nomenclaturerevisionforencapsulatedfollicularvariantofpapillarythyroid carcinoma,JAMAOncol.2(2016)1023.
[7]P.W.Rosario,G.F.Mourão,Noninvasivefollicularthyroidneoplasmwith papillary-likenuclearfeatures(NIFTP):areviewforclinicians, Endocrine-RelatedCancer26(2019)R259–R266.
[8]M.Pusztaszeri,M.Bongiovanni,Theimpactofnon-invasivefollicularthyroid neoplasmwithpapillary-likenuclearfeatures(NIFTP)onthediagnosisof thyroidnodules,GlandSurg.8(2019)S86–S97.
[9]R.A.Agha,T.Franchi,C.Sohrabi,G.Mathew,A.Kerwan,SCAREGroup,The SCARE2020guideline:updatingconsensusSurgicalCAseREport(SCARE) guidelines,Int.J.Surg.(2020),http://dx.doi.org/10.1016/j.ijsu.2020.10.034, S1743-9191(20)30771-8.Epubaheadofprint.
[10]M.R.HaroonAlRasheed,A.Acosta,G.Tarjan,Encapsulatedfollicularvariant ofpapillarythyroidcarcinoma/noninvasivefollicularthyroidneoplasmwith papillary-likenuclearfeatureswithSpindleCellMetaplasia:casereportand reviewofliterature,Pathol.-Res.Pract.213(2017)416–421.
[11]G.Arnoux,M.Pusztaszeri,“Noninvasivefollicularthyroidneoplasmwith papillary-likenuclearfeatures”withfocalspindlecellmetaplasia,Int.J.Surg. Pathol.26(2017)261–265.
[12]A.G.Abdou,H.Aiad,N.Asaad,CaseReport:multifocalnon-invasivefollicular thyroidneoplasmwithpapillary-likenuclearfeaturespresentinginafemale child,F1000Research9(2020)645.
[13]A.Smith,J.Eccles-Smith,M.D’Emden,K.Lust,Thyroiddisordersinpregnancy andpostpartum,Aust.Prescr.40(2017)214–219.
[14]K.Zajkowska,J.Kopczy ´nski,S.Gó ´zd ´z,A.Kowalska,Noninvasivefollicular thyroidneoplasmwithpapillary-likenuclearfeatures:aproblematicentity, Endocr.Connect.9(2020)R47–R58.
[15]K.RahimDurr-e-Sabih,Thyroidnoduleimaging,statusandlimitations,Asia Ocean.J.Nucl.Med.Biol.3(2015)50–57.
[16]B.Pigac,S.Masic,Z.Hutinec,V.Masic,Rareoccurrenceofincidentalfindingof noninvasivefollicularthyroidneoplasmwithpapillary-likenuclearfeatures inhurthlecelladenoma,Med.Arch.72(2018)367.
[17]S.Dideban,A.Abdollahi,A.Meysamie,S.Sedghi,M.Shahriari,Thyroid papillarymicrocarcinoma:etiology,clinicalmanifestations,diagnosis, follow-up,histopathologyandprognosis,Iran.J.Pathol.11(2016)1–19.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.