Caries experience and risk
assessment in 6-year-olds and
14-year-olds living in
Malmö, Sweden
Author:
Turki Almujaweb
Supervisors:
Gunilla Klingberg
Karin Ridell
Master Thesis in Odontology (30 ECTS)
Malmö University
International Master Program
Faculty of Odontology
3
ABSTRACT
Aim: to study if children with caries in primary teeth at age 6 had more caries in permanent
teeth at age 14 compared to children who were caries-free at age 6. Besides that, if children who were judged as having high caries risk at age 14 had higher DMFT than children with low caries risk in the same age, and if children with high caries risk at age 14 had higher dmft at age 6 than children with low/moderate risk at age 14. Method: Dental records from 2655 15-year-olds were reviewed by two investigators. Information was collected on background information (age, gender, medical status), dmft value and risk assessment at age 6, DMFT value and risk assessment at age 14. Results: Individuals with higher dmft values at age 6 had higher DMFT values at age 14 years. Individuals who were judged as low/moderate risk individuals at age 14 showed less caries experience than individuals who were judged as high/ very high risk individuals. The individuals who were judged as low/moderate risk individuals at age 14 showed less caries experience at age 6 and report less dmft value than individuals who were judged as high/ very high risk individuals. Conclusion: Individuals with higher caries experience at young age had higher DMFT values and were judged as high caries risk individuals at age 14. Therefore, dmft value at young age can be used as a predictor for future carious experience in adolescence.
4
Table of contents
Abstract……….3
Introduction ………..5
Epidemiology of dental caries……….5
Dental caries impacts ………...5
Dental caries as a multifactorial disease. ………6
Microbiology of dental caries. ………7
Demineralization and remineralization.………...8
How to diagnose carious lesions ……….8
Caries progression ………...9
Caries risk assessment ………...10
Aim...………...11
Problems... ………...11
Hypothesis....………...11
Material and Methods.…..………...12
Ethical consideration..………...12
Results....………...13
Discussion….………..16
Conclusion…..………...18
5
INTRODUCTION
Dental caries remains the most common oral disease worldwide and it is documented that dental caries can effect oral and general health (1-3). In 2010, untreated caries in permanent teeth considered as the most common health condition in the world and untreated caries in deciduous teeth was the 10th most common condition (4). Dental caries is a multifactorial disease leading to a localized destruction of the enamel and dentin. Acids metabolized by cariogenic bacteria from carbohydrates (mainly sucrose) will initiate tooth structure destruction (5).
Epidemiology of dental caries
Dental caries is affecting around 60–90 % of schoolchildren and adults in industrial countries. It is the most common oral disease in many Asian and Latin American countries, while it appears to be less common and less severe in African countries (6). However, it has been suggested that dental caries incidence will increase in the future in many developing countries of Africa, because of growing consumption of sugars and inadequate exposure to fluorides in those countries. Besides that, the problem is the limited and difficult access to oral health services in most developing countries (6). A systematic review reported that untreated caries in permanent teeth in 2010 affected 2.4 billion people worldwide or 35 % of world
population. The prevalence in deciduous untreated teeth was affecting 621 million children worldwide or 9 % of world population (4).
According to Swedish National Board of Health and Welfares’ (Socialstyrelsen)
epidemiological national survey from 2015, only manifest caries lesion were measured not the initial caries, reported the percentage of caries free in Swedish preschool children at age 3 years and 6 years old to be 96 % and 75 % respectively. Also, the survey presented the percentage of the Swedish adolescents in 12-year-olds and 19-year-olds. In these age groups 67 % and 37 % are caries free (7).
The survey also presented data from Region Skåne of 3-year-olds group and 6-year-olds group (each group approximately 13.000 children). The survey found that the percentage of caries free in 3-year-olds and 6-year-olds was 94 % and 73 % respectively. The corresponding data for 12-year-olds and 19-year-olds were 67 % and 37 % respectively (7).
Dental caries in permanent teeth can be reported in the form of the DMFT or DMFS values (D = decayed, M = missing due to caries, F = filled due to caries). T means teeth, while S means tooth surfaces. The primary teeth analyzed through the same manner by using small letters dmft, dmfs or dt. The regional office of WHO for oral health in Europe proposed goals by 2015, which are: 80 % or more caries free for 6-year-olds age, 12-year-olds shall have no more than DMFT = 1.5 of at least 1.0 shall be FT value, and 18 years olds to be without missing teeth due to caries (8).
Dental caries impacts
Dental caries is a major problem and have impact on both oral and general health, as oral health is an integrated part of general health. Dental caries may affect the individual’s quality of life in many aspects (see Box.1). It can lead to pain and discomfort because of infections and abscesses formation, which may result to limitation in oral function such as influencing on chewing and eating ability, and may be reduce the appetite and food intake (9,10). It is reported that dental caries has an impact on social life and may effect on the daily activities
6 and disturbed individual’s sleeping (9,11). A Norwegian study published 1999 found that there is a positive relation with high DMFT, high dental anxiety and missed dental
appointments among 169 subjects (12). A cross sectional survey in 417 schoolchildren aged 6 to 8 years found a relation between the higher values of untreated caries with poorer growth in Saudi schoolchildren (13).
Besides that, carious lesions may effect children with compromised health conditions like cardiac diseases, cancer, hemophilia, those receiving radiation therapy, and immuno-compromised by disease and/or therapy. The risk and potential sequelae of poor oral health and caries are greater with medically compromised children. The dental infections and dental treatments of carious lesion may lead to life threatening complications (14).
Dental caries as a multifactorial disease
Dental caries is a multifactorial disease leading to a local destruction of the enamel and dentin. The destruction is started by acids metabolized by cariogenic bacteria from
carbohydrate, mainly sucrose. Then, the minerals are lost from enamel surface due to acidic attack generated by bacteria and if this process continues the cavity will occur (5,15). Rothman et al. 2008 developed a model to understand the dental caries as a multifactorial disease caused by interaction between the biofilm, sugary diet and host factors. They
suggested that if any factor is reduced the caries susceptibility is decreased (16). In addition, Fisher-Owens and colleagues published a model for the dental caries as multifactorial disease (Fig.1.), describing the roles for the child, the family and the community beyond the classical biological infectious disease model (17).
In 2001, Burt and Pai reported in their systematic review a clear relationship between sugar intake and caries in modern life. The authors suggested that the patient with high risk of caries should be motivated to change his/her dietary habits to less sugar intake (18). Sundin and
Box 1.The impact of the dental caries on both oral and general health (presented and rephrased from Pediatric Dentistry – A clinical approach, 3rd edition 2017) :
Physical
Pain and discomfort.
Risk of pain during invasive dental treatment. Risk of development disturbance of permanent teeth. Risk of occlusal development disturbance.
Growth retardation due to appetite loss and reduced food intake. Sleep problems.
Special problems in medically compromised children due to disease and/or therapy.
Psychological and emotional
Dental fear and anxiety.
Being teased by others and/or lower self-estimation due aesthetic, speech problems.
Behavioral
Behavior management problems.
Lack of regular attendance to dental care and missed dental appointments.
Social
Disturbance of daily activities and habits.
7 coworkers found that frequency of consumption of sweets was an important caries related factor in Swedish 15-18 year old teenagers. Both the amount of sugar and the frequency of sugar intake are strong factors related to caries development. In addition, oral hygiene, socioeconomic status, and fluoride exposure all influence the sugar caries relationship (19).
Fig.1. A multifactorial model of dental caries depicting possible factors. From Fisher-Owens et al. (2007) (17).
Microbiology of dental caries
More than 700 different types of microorganism have been detected in the mouth (20). Teeth provide the only non-shedding surface within the body to which the resident microflora can normally attach. Teeth are always covered by an acellular proteinaceous film called pellicle, which are salivary glycoproteins, phosphoproteins and lipids. The acquired pellicle is formed on the tooth enamel surface (with start in pits and perikymatal grooves) immediately upon teeth brushing or professional cleaning within minutes. Adherent bacteria contain a
recognition system on their surface, which enable bacteria to attach to receptors within the acquired pellicle on the tooth surface (21).
The initial colonizers constitute a highly selected part of the oral microflora, mainly
streptococcal sanguinis, streptococcal oralis, streptococcal mitis, actinomyces ssp, and gram negative bacteria. Mutans streptococcus comprise only 2 % or less of the initial streptococcal population irrespective of the caries activity of the individual (21). The bacteria create an environment that is more attractive to secondary invaders, secondary colonizers attach to the
8 established pioneer species via adhesion receptor inter action. Dental biofilm develop bacteria producing polysaccharides from metabolism of sucrose and form biofilm matrix (21).
Characteristic features of dental biofilm bacteria are the ability to transport sugar and convert it to acid, the ability to tolerate acidic condition and maintain sugar metabolism; acidogenic and aciduric, and the ability to produce extracellular (EPS) and intracellular polysaccharides (IPS). EPS include glucans and fructans contribute to biofilm matrix and IPS are glycogen like storage compound converted to acid when free sugar are not available (21).
A major change to the habitat such as frequent carbohydrate intake can disrupt the ecology of the dental biofilm by the selection of acidogentic and aciduric species. These acidogenic (acid-producing) oral plaque bacteria produce weak acids, which are a product of
carbohydrate metabolism (lactic, formic, acetic and propionic acids). These acids result in a decrease in PH below the critical value (5.0-5.5) leading to increase the solubility of calcium hydroxyapatite in the enamel and demineralization occurs. In (low PH) environment, mineral (calcium and phosphate) continues diffusing out of the tooth and the enamel become more porous, leading eventually to carious lesion. Microflora on the tooth surface changes with caries lesion development from dominance of non mutans streptococci and actinomyces to dominance of mutans streptococcus and other non mutans including lactobacilli (21-24).
Demineralization and remineralization
Demineralization and remineralization are processes of exchange of ions between the tooth minerals and the oral environment. During demineralization, ions and minerals are exchanged between saliva and enamel through the biofilm. Dental caries activity is determined by the dynamic balance between pathological factors that lead to demineralization and protective factors that lead to remineralization (fig.2), (25).
Fig 2. Schematic diagram of the balance between pathological factors and protective factors in the dental caries process. From Featherstone (1999) (25).
How to diagnose carious lesions?
It has been reported that visual-tactile examination and radiographic examination together are the most reliable diagnostic method for dental caries. Visual-tactile examination is simple,
9 cheap and more reliable than either method used separately. Visual and tactile refers to using a mouth mirror and probe for tooth examination. For optimal visual examination, it is
recommended to have good lighting and the examined teeth must be cleaned prior to the examination and kept dry by using cotton rolls or compressed air blasts (26).
The radiographs should be of good quality and taken on individual indications to avoid unnecessary exposure to radiation (for example, high caries risk may require radiographs taken every year but at low caries risk may needs radiographic examination every 2-3 years). Also value of early diagnosis and cost of dental radiography in term of time, radiation and resources should be considered (9,26).
Two studies using visual-tactile and radiographic examination have found that the sensitivity (correctly identifies surfaces damaged by caries) of the combined method are 49 and 65 %, and specificity (correctly identifies sound surfaces) 87 and 73 %, respectively (27,28). The ICDAS (International Caries Detection and Assessment System) is a diagnostic detecting system to assess and grade the caries lesion severity. Seven codes (0 – 6) are ranged from sound to extensive distinct cavity with visible dentin. These criteria used as visual
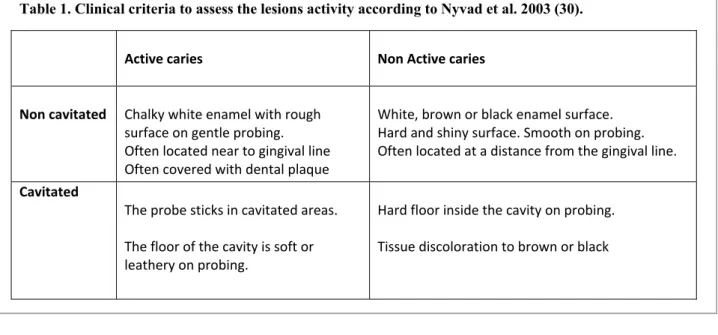
examination for pit, fissures and smooth surfaces. Besides that, detection of severity of the proximal carious lesions are done from the bitewing radiographic examinations (9). However, the assessment of lesion activity is also important. It has been suggested six grades (modified to four grades) as criteria for active and non active lesions (29). The criteria is presented in Table 2. This criteria is used in a clinical trial to study the effect of daily supervised brushing with fluoride toothpaste was carried out among 273 12-year-old children. The researchers found that the active non cavitated lesions had higher risk to be cavitated lesions than non active non cavitated lesions (9,30).
Table 1. Clinical criteria to assess the lesions activity according to Nyvad et al. 2003 (30). Active caries Non Active caries Non cavitated Chalky white enamel with rough surface on gentle probing. Often located near to gingival line Often covered with dental plaque White, brown or black enamel surface. Hard and shiny surface. Smooth on probing. Often located at a distance from the gingival line. Cavitated The probe sticks in cavitated areas. The floor of the cavity is soft or leathery on probing. Hard floor inside the cavity on probing. Tissue discoloration to brown or black
Caries progression
Progression of dental caries in permanent teeth in low prevalence populations from enamel dentin border to outer half of dentin is usually slow (31-33). The caries progression from the inner half of the enamel to the outer half of dentin on mesial surface of the first permanent molar was almost four time faster in the younger group (6-12 years) than in the older group (12-22 years) (34). A Swedish radiographic study analyzed 918 occlusal lesions in children
10 aged 14 and 15 years old. Of unrestored occlusal outer dentine caries 8.8 % are progressed to deep dentine caries during one year. Besides that, of 629 proximal outer dentine lesions, only 33 lesions have progressed to deep dentine caries during one year. 42 % were restored and 53 % have not progressed. (35).
The caries progression can be effected by many factors. Tooth surface type is one of these factors. Mejàre and coworkers showed that the distal surface of maxillary second premolar and mesial surface of mandibular second molar had faster progression (2.1 and 2.8
respectively) compared to the median progression period of 3 years. However, posteruptive age, caries experience and iatrogenic damage on neighboring surfaces are factors may effect dental caries progression rate (9,36).
A study analyzed bitewing radiographs from over 700 children and found that over 40 % of the carious lesions in permanent teeth were not progressed during a period of four years. Also, the authors found that the newly erupted first permanent molars had faster carious progression rate, it took between 19- 28 months to reach the dentin. Besides that, the study analyzed caries progression in primary teeth, the researchers found that the average was 12 months for a lesion to progress through the outer half of the enamel layer, and on average 10-12 months for a lesion to progress through the inner half of the enamel layer (31).
Caries risk assessment
The best prediction risk factor of dental caries in the future is previous caries experience (26). Caries risk assessment should be included as a part of the dental examination. It is used to help health care providers to identify individuals with increased risk of the disease and could also be help to understand the factors associated with caries development. The specific information gained from a systematic assessment of caries risk guides the dental team in the decision making process to establish treatment and preventive procedures for children with oral disease and for those considered to be at risk (37,38). This procedure should performed at any child's first dental visit and then regularly throughout life, and especially when the
individual involved with social or medical problems (39). Risk is defined as the probability that some harmful event will occur and caries risk assessment is the clinical procedure to predict the probability of future caries development (40).
Different models to assess risk are available. Risk factors commonly used for caries risk assessment are previous caries experience, general diseases, dietary intake of sugar amount and frequency, plaque index, streptococcus mutans test, fluoride exposure, saliva test, buffer capacity, socioeconomic level, and oral hygiene (9,26). The Swedish Public Dental Service developed a risk assessment system used to assess the children, adolescents and adults. The risk assessment for the children depends on the caries, periodontal health and general status of the individual. On other hand, the risk assessment of the adults depends on the caries,
periodontal health, general and technical risks.
One of these models is the Cariogram, which is an interactive computer programs for caries risk assessment. Several causal risk factors of importance for the caries process analyzed together and the chance to avoid tooth decay calculated. The Cariogram was evaluated in a prospective clinical trail in schoolchildren with 2 years follow up by Hänsel Petersson and coworker in 2002. The probability was higher to identify low risk patients (specificity) than those with higher risk (sensitivity). One advantage is that it can be used as an educational tool for children and parents to facilitate the understanding and discussion with them (41).
Recently, another risk assessment program is used called R2 (beslutsstöd R2). This system is assessing caries risk, risk of periodontal diseases, and general and technical risk (38).
11 A systematic review published in 2014 concluded that the accuracy of multivariate models are superior over the single models for pre-school children than for schoolchildren/adolescents caries prediction (42). Several studies on both toddlers and preschool children found that the presence of mutans streptococci and/ or lactobacilli in saliva as sole predictor for caries development among children have low accuracy (26). The dentist can use the posteruptive age as caries predictor since the risk of lesions developing is high after eruption period (9).
Concerning caries lesion risk on occlusal surfaces, the first molars are at greatest risk during the first year and the second molars during the first 2–3 years after eruption. On the other hand, the proximal surfaces are at greatest risk during the first 3–4 years after eruption (9,26). It has been reported that the most susceptible tooth to dental caries in the young permanent dentition is the first permanent molar. The researchers found that more than 60 % of all restored surfaces at the age of 21 were performed in first permanent molar (36). Mesial and distal surfaces of first molar and distal surface of 2nd premolar are the most caries susceptible surfaces between 13-27 years old subjects (43).
A cross-sectional study analyzed 286 children aged between 24 to 72 months. The authors found that the posterior primary teeth had a higher risk for caries than the anterior teeth, the interproximal sites with closed contact points were at greater caries developing risk than those with open contact points (44). Several studies in the primary teeth in North American children found more carious lesions in molars than in anterior teeth (45,46).
AIM
The aim of this paper was to study if
children with caries at age 6 (dmft) have more caries in permanent teeth at age 14 (DMFT), compared to children who are caries- free at age 6.
children who are judged as having high caries risk at age 14 had higher DMFT than children with low risk at the same age.
children who are judged as having high caries risk at age of 14 have higher dmft at age 6 than children with low/moderate caries risk at age 14.
PROBLEMS
Do children with caries at age 6 (dmft) have more caries in permanent teeth at age14 (DMFT), compared to children who are caries free at age 6?
Do children who are judged as having high caries risk at age 14 have higher DMFT compared to children with low caries risk at the same age?
Children with high caries risk at age 14, did they have higher dmft at age 6 than children with low/moderate caries risk at age 14?
HYPOTHESIS
Children with caries in primary teeth at age 6 have more caries in permanent teeth at age 14. Children judged as having high caries risk at age 14 have more caries at age 14 and age 6.
12
MATERIALS AND METHODS
In 2005, the year of collecting the material for the study, The Swedish Public Dental Service offered all children and adolescents between 0-19 years of age free dental care. At that time, the city of Malmö, Sweden, had 19 Public Dental Service clinics (35). This study is part of a previous study in which the prevalence of caries in children born in 1990 and residing in the city of Malmö in 2005 was studied (35).
For this study 2655 individual were eligible. The individuals were all born in 1990 and included in the Public Dental Service in the city of Malmö in 2005.The data was retrieved from dental records. The dental records were reviewed and analyzed by the author and another international master student in pediatric dentistry (here called investigator).The investigators collected about half of the data each. The individuals’ identity was not exposed to the investigators, all individuals were identified by code numbers and a separate code list was performed.
A protocol was performed and tested. Adjustments were made before starting collecting data. The following data was collected from the dental records:
- Background information including age, gender, and medical status/condition. Medical status/condition was categorized into individuals with no medical problem and individuals with medical problem (chronic disease). Chronic disease was defined according to Westbom et al. 1987 as any medical condition that may interfere with normal life and/or needs a treatment for at least three months (53).
- Caries experience expressed as dmft and DMFT: dmft = number of decayed, missing due to caries and filled teeth in the primary dentition, DMFT = number of Decayed, Missing due to caries, and Filled Teeth in the permanent dentition. Teeth were only considered to fulfill the criteria for `missing` and `filled` if caries had been the reason for this diagnosis. For missing primary teeth normal exfoliation was not considered nor extractions due to trauma. The reason for a missing tooth was verified by the notes. dmft was collected at age 6 and DMFT form age 14. If data was not found at age 6, information was collected from age 7, 8 or 9. In the same way, if data was not found at age 14, information was collected from age 15 or 16. - Risk assessment based on a risk assessment program for children and adolescents used by the Public Dental Service in Region Skåne at that time. The individuals were categorized to group 1 (low caries risk), group 2 (moderate caries risk), group 3 and 4 (high and very high caries risk) (Table 2). The data was collected by using a protocol.
The investigators were calibrated and inter- and intra-examination reliability was calculated. All data were transferred to software SPSS version 22 (IBM SPSS Statistics 22 IBM, New York, US) for processing the data.
Statistics
The consistency of the variables was measured using the weighted kappa-statistics (47). Differences between mean values were evaluated using Mann-Whitney or Kruskal-Wallis test. To access the difference within the groups at age 6 and 14, Mann-Whitney test was used. The level of significance was set to 0.05. The inter-examiner agreement for the variable dmft at age 6 had a weighted kappa value of 0.71 (CI 0.52-0.90) and for DMFT at age 14 0.72 (CI 0.52-0.93). The intra-examiner agreements had weighted kappa values for the dmft at age 6 of
13 0.87 (CI 0.76-1.0) and 0.66 (CI 0.39-0.94) and for DMFT at age 14 0.77 (CI 0.52-1.0) and 0.66 (CI 0.37-0.94).
Table 2. Guidelines for risk assessment in children and adolescents developed by the Swedish Public Dental Services in Region Skåne. Individuals are categorized based on caries risk, periodontal risk and general risk. The highest score obtained decides the final classification of risk group.
ETHICAL CONSIDERATION
Maintaining the confidentiality of the children´s rights and data is obligatory in all research phases. The data of present study is gathered from a previous study (35) that has been approved by Regional Ethics Committee of Lund University, Sweden (Dnr 76/2005).Using children’s personal and medical data in any study is controversial issue from an ethical aspect. Since, they cannot give their agreement or sign any informed consent from a legal point of
Risk group 1 Low risk Risk group 2 Moderate risk Risk group 3 High risk Risk group 4 Very high risk
Caries/Perio No caries progression last 2 years Within 2 years: Caries progression in the enamel 1-2 new manifest caries lesions Gingivitis Within 2 years: Several new and/or progression of earlier initial caries lesions 2-3 new manifest caries lesions Generalized gingivitis Within 2 years: Extensive caries progression
3 or more manifest caries lesions
Extensive need of restorative care at earlier treatment period
Periodontal pockets › 5 mm
Marginal bone loss
General No disease/ disability/ medication/ unfavorable habits Slightly treatment affecting disease/ disability/ medication/ habits Moderate treatment affecting disease/ disability/ medication/ habits/ dental anxiety/ behavior management problems
Severe treatment affecting disease/ disability/ medication/ habits/ dental anxiety/ behavior
14 view. Also, they are not able to understand the full consequences of the research, possible risks and suggested benefits and aspects of integrity. The parents or caregivers are responsible to do this procedure. However, the studies on humans should require competent individuals able to give their consent.
On the other hand, limits the researches on a group of individuals and excluding another group will be problematic, because it will affect researchers’ abilities to explore and reach many facts from their researches that might improve the health and living conditions for excluded groups. This controversial issue is mentioned and expressed in declarations of the rights and formulations of the laws and proclaimed by UNICEF, and approved in the United Nations Convention on the Rights of the Child from 1989 (48). The convention confirmed all needs and rights of the child. Also, announced principles to ensure human rights and legal safeguards for children. The child is defined as any individual under the age of 18 years. This means that not every child has the maturity and development to participate in the same way children’s age, maturity, physical, and psychological status must be considered before participating this age group in any research. It is important that the researchers should be aware about all the benefits and risks of involving children in their researches.
The participation of the child should base on informed consent from each child’s legal guardian (parents or caregivers). The Swedish Ethical Review Act states that the children at age of 15 or older should give consent to participate by themselves (49). Even if the legal guardian (parent or caregiver) gives consent to the child’s participation, the research should not perform until the child understands the objectives and objects of participation.
RESULTS
Table 3. Study population characteristics.
*dmft/DMFT = no. of caries lesions, missed teeth due to caries and filled primary/permanent teeth. Missing data is reported.
The study population consisted of 2655 individuals (47.9 % males and 52.1 % females) from 19 public dental service clinics. Number of individuals varied between the clinics, and the clinics were represented 1.5- 8 % (n = 40 – 207) of all individuals. The number of the individuals, their medical condition, dmft and DMFT value are presented in Table 3. Ninety-four percent of the individuals were marked as healthy or having seasonal or non-seasonal allergies. Six percent of the individuals had medical problems such as congenital heart
Individuals N (%)
Medical status (missing =10)
Healthy and allergies Medical problems N (%) N (%) dmft age 6 (missing=304) mean (SD) DMFT age 14 (missing= 22) mean (SD) Female 1272 (52.1) 1189 (93.5 %) 78 (6.1 %) 2.0 (3.1) 2.1 (2.5) Male 1383 (47.9) 1289 (93.2 %) 89 (6.4 %) 2.4 (3.3) 2.0 (2.5) Total 2655 (100) 2478 (93.3 %) 167 (6.2 %) 2.2 (3.2) 2.0 (2.5)
15 diseases, diabetes, asthma or syndromes. Data on medical status was missing in 10
individuals.
The mean dmft at age 6 differed between females and males (2.0 and 2.4) respectively. The difference was statistically significant (p=0.014). At age 14 there was no difference between the sexes. A total of 304 (11.5 %) individuals were excluded from dmft evaluation and 22 (0.8 %) individuals from DMFT evaluation due to missing information in the dental records. The distribution of dmft values, at age 6 is presented in Figure 3. Out of 2351 individuals 52 % (n = 1221) were caries-free in primary teeth, 22 % (n = 522) had a dmft value of 1-3 and 26 % (n = 608) had a dmft value ≥ 4. Almost 4 % (n = 91) reported dmft values ≥ 10.
The distribution of DMFT values at age 14 are presented in Figure 4. Out of 2633 individuals 38 % (n = 991) were caries-free in permanent teeth. Forty percent (n = 1064) had a DMFT value of 1-3, and 22 % (n = 600) had a DMFT value ≥ 4. Almost 1 % (n = 38 ) reported DMFT values ≥ 10.
Table 4 shows the number of the individuals reported as having dmft value=0, 1-3 and ≥4 at age 6 years and compare it with the mean DMFT value at age 14. Individuals with low dmft value at age 6 also had low DMFT values at age 14. Meanwhile, the individuals with higher caries experience at age 6 had higher DMFT value at age of 14 years compared to these with lower dmft at age 6. The difference were statistically significant (P=0.000). Data at age 6 and/or age 14 is missing in 320 individuals.
Table 4. Relationship between dmft age 6 (grouping 0; 1-3; ≥ 4) and mean DMFT age 14.
p=0.000 (Kruskal –Wallis test)
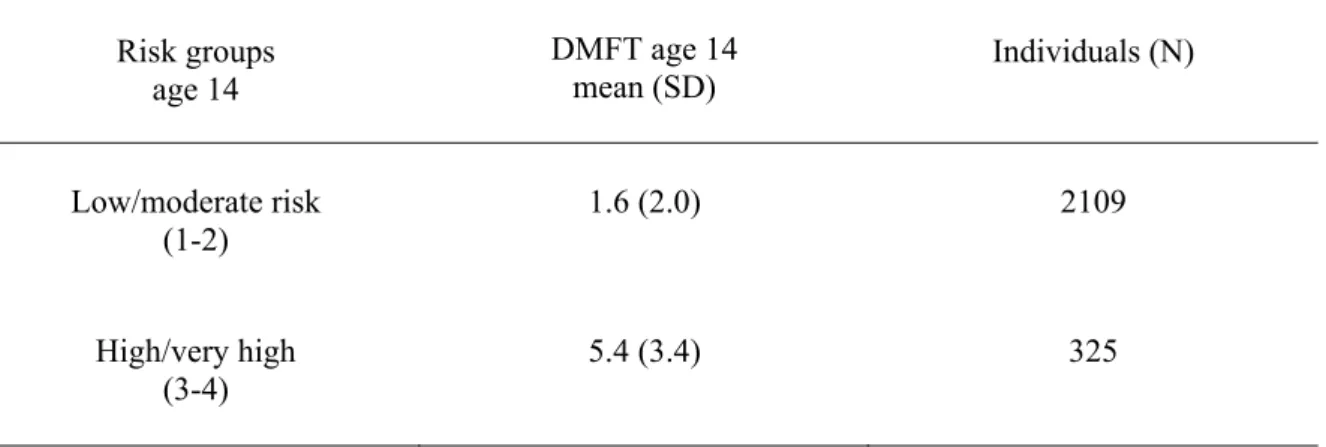
The relation between risk groups at age 14 and mean DMFT values at the same age are shown in Table 5. The individuals who were judged as low/moderate risk individuals at age 14 showed less caries experience (DMFT mean = 1.6) than individuals who were judged as high/very high risk individuals (DMFT mean = 5.4). The differences were statistically significant (P=0.000).
The relation between risk groups at age 14 and mean dmft values at age 6 is shown in Table 6. The individuals who were judged as low/moderate risk individuals at age 14 showed less caries experience (dmft mean value = 1.9) at age 6 and report less dmft value than individuals who were judged as high/very high risk individuals (dmft mean = 4.8). The results were
dmft age 6 DMFT age 14
mean (SD) Individuals (N)
0 1.0 (1.5) 1211
1-3 2.0 (2.1) 520
16 statistically significant (P=0.000). Risk group assessment at age 6 was missing in 994
individuals of the sample papulation and missing at age of 14 years in 222 individuals.
Fig 3. Distribution of dmft values at age 6.
17 Table 5. The table shows the relationship between individuals’ risk groups, DMFT mean values at age 14 and total number of individuals in each risk group.
p= 0.000 (Mann-Whitney test).
Table.6.The table shows the relationship between individuals risk groups at age of 14, dmft mean values at age 6 and the total individuals number of each risk group.
p=0.000 (Mann-Whitney test).
DISCUSSION
This study has shown that individuals with high caries experience at age 6 have more caries experience at age 14 and are judged as having higher caries risk at that age. Several studies have shown that past caries experience is related to future dental caries (50-52). Motohashi M. et al. 2006 in a prospective cohort study found that the dmft score is a useful tool to predict future caries lesions in permanent teeth (52).
Furthermore, the results are compatible to the results of a systematic review published by The Swedish Council on Technology Assessment in Health Care in 2007. They found that the previous caries experience is the single best prediction factor of future caries (26). A systematic review published 2014 suggested that the caries experience had moderate/good accuracy in pre-school children and limited accuracy in schoolchildren and teenagers, however, the caries experience was the most accurate single predictor in all age groups (42).
Risk groups age 14 DMFT age 14 mean (SD) Individuals (N) Low/moderate risk (1-2) 1.6 (2.0) 2109 High/very high (3-4) 5.4 (3.4) 325 Risk groups age of 14 dmft age 6 mean (SD) Individuals (N) Low/moderate risk (1-2) 1.9 (3.0) 1885 High/very high (3-4) 4.8 (4.1) 266
18 The results of this study and previous studies suggests that previous caries experience can be used as a predictor for future caries status in older ages.
According to Westbom et al. 1987 (53), the definition of the chronic illness is any medical condition that may interfere with normal life and/or needs a treatment for at least three
months. In this study, it was difficult to estimate the medical status in dental records for some of the individuals. Therefore, the results shall be taken with some caution. Nevertheless, the results showed that 6 % of the study population had medical problems. Westbom et al. 1987 found that 8.4 % of the 15 years old Swedish children had a chronic condition (53). This finding is almost similar to the results in this study. The number of individuals with medical conditions may can reflect the Swedish population and not affect the results in this study. The purpose of this study was to analyze the relationship between caries experience and individuals’ different risk groups (an assessment tool predetermined by dental team). The caries experience was calculated by dmft values at age 6 and DMFT values at age 14. Three hundreds and four individuals (11.5%) have no information about their caries experience at age 6 and in the age-group 14 information was missing in 22 individuals (0.8%). This must be considered as a low amount of missing data and therefore the caries data must be considered as valid.
The most frequent missing item from the dental records was risk group assessment at age 6 in which reviewed records showed missing risk group assessment in around 37 % of the
population. The exact cause of this issue is unknown, however, risk assessment is an important procedure to give the adequate preventive procedures to the patient (37-39). Nevertheless, the large sample size (2655 individuals) is a strength in this study.
As in any study with retrospective design, missing data and using unclear terms in dental records caused major challenges during data collection process. The results depends mainly on the accuracy of information reported in the dental records.
Hypotheses and study questions can be used in a prospective study design, which is superior to a retrospective study design (54). In this study the individuals could have been examined at age 6 and then followed to the age of 14 prospectively. Furthermore, more questions could have been added to the study. The prospective design for the same number of individuals that was used in the study would have taken longer time, been more expensive, and may have needed more human power. Nonetheless, a retrospective study design is considered to be an inexpensive and quick method to analyze existing data. Taken in consideration that this study is a retrospective study, the questions (problems) were answered and the hypotheses were verified.
The risk assessment data were collected from the dental records depended on a classification that was used by Public Dental Service (Folktandvården) in Region Skåne – Sweden.
Individuals were categorized into different risk groups according to the assessment of caries, periodontal health, as well as medical and physical status of each individual. Accordingly, dentists assigned the individuals to Group 1 (low risk), Group 2 (moderate risk), 3 and 4 (high risk and very high risk) after complete dental examination. In this study, the caries
experiences of the individuals compared to the risk assessment that previously mentioned.
The caries risk assessment is also an essential procedure to evaluate the patient’s caries risk factors and guide the dentist in the decision making process to establish prevention, treatment procedures and recall intervals (37-39). Today, a risk assessment program called Beslutsstöd
19 R2 used in Public Dental Service in Region Skåne. This program is not only judging caries risk but also risk for periodontal diseases, general and technical risk. Which is different from the risk assessment that used in this study.
The individuals’ dental records were collected from all 19 dental clinics in Malmö- Sweden in 2005. Each of these dental clinics are represented in the sample. All individuals born in 1990 were included. The sample could represent caries experience status at age of 6 and age of 14 in Malmö city at that time, because the sample consists of all 14 year olds at the Public dental service at that time. However, if the results can reflect the caries experience in other parts in Sweden is unsure because of the high percent of inhabitants with immigrant background in Malmö. At 2006, 27 % of Malmö city population were born abroad (55). In 2015, the authorities announced that individuals born abroad represented 22.5 % of the Malmö population (56). Studies have shown that children with immigrant background have poorer oral health and higher DMFT values compared to other groups (57-59).
According to Swedish National Board of Health and Welfares’ (Socialstyrelsen)
epidemiological national survey 2005, the percentage of caries free children living in Sweden for 6 and 12-year-olds groups were 73 % and 58 % respectively. Data from Skåne was not available at that time. The results from this study showed 52 % caries free children aged 6 and 38 % adolescent aged 14 which shows that the studied population had more caries experience that presented in national data. (60).
In 2015, the percentage of caries free children living in the Skåne region (Malmö city is part of Skåne region) were 73 % for 6-year-olds and 67 % for the 12-year olds. (7). Although the data were collected from a population born in 1990 in this retrospective study it may reflect the current caries experience in children and adolescents in Malmö since prevention programs and treatment protocols at these different periods probably are almost the same. However, caries prevalence is also depending on other factors such as the population´s knowledge and attitudes (59,61,62).
Moderate to very good agreement was found in the inter-examiner and intra-examiner agreement depending on the variables. This shows that the data was correctly collected and gives a strength to the study results (47).
CONCLUSION
Based on this study’s results, individuals with higher caries experience at a young age are associated with higher DMFT values in the future as well as judgement as high caries risk individuals. Therefore, dmft value at young age can be used as a predictor for future carious experience in adolescence.
20 1. Evans CA, Kleinman DV. The Surgeon General’s report on America’s oral health:
Opportunities for the dental profession. J Am Dent Assoc. 2000;131:1721-1728. 2. US Dept. of Health and Human Services. Oral health in America: A Report of the
Surgeon General. NIH Publication 00-4713. National Institute of Dental and Craniofacial Research, National Institutes of Health;2000:7.
3. Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: child and parent perspectives. Pediatr Dent 2003;25:431-440.
4. Kassebaum NJ, Bernabe E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res 2015;9:650-658.
5. West NX, Joiner A. Enamel mineral loss. J Dent 2014;42 Suppl 1:2-11.
6. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ 2005;83:661-669. 7. Socialstyrelsen: Karies hos barn och ungdomar, Epidemiologiska uppgifter för år
2017. Available at: www.socialstyrelsen.se/publikationer2017/2017-11-6. Accessed
20171120.
8. World Health Organization. Health 21: the health policy framework for the WHO European region. European health for all series No. 6. Copenhagen: S Regional Office for Europe, 1999.
9. Koch G, Poulsen S, Espelid I, Haubek D. Pediatric Dentistry – A clinical approach. Chichester,UK. Wiley-Blackwell. 3rd edition, 2017:75-160.
10. Alsumait A, ElSalhy M, Raine K, Cor K, Gokiert R, Al-Mutawa S, et al. Impact of dental health on children's oral health-related quality of life: a cross-sectional study. Health Qual Life Outcomes 2015;13:98.
11. Low W, Tan S, Schwartz S. The effect of severe caries on the quality of life in young children. Pediatr Dent 1999;21:325-326.
12. Skaret E, Raadal M, Berg E, Kvale G. Dental anxiety and dental avoidance among 12 to 18 year olds in Norway. Eur J Oral Sci 1999; 107: 422-28.
13. Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Tsakos G. Dental caries and growth in school-age children. Pediatrics 2014;133:616-23.
14. Foster H, Fitzgerald J. Dental disease in children with chronic illness. Arch Dis Child 2005;90:703-708.
15. Featherstone JD. The continuum of dental caries--evidence for a dynamic disease process. J Dent Res 2004;83:39-42.
16. Rothman KJ, Greenland S, Lash TL. Modern epidemiology. Philadelphia, PA: Lippincott- Raven, 2008.
17. Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA, Soobader MJ, Bramlett MD, et al. Influences on children's oral health: a conceptual model. Pediatrics 2007;120:510-520.
18. Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dent Educ 2001 ;65:1017-1023.
21 19. Sundin B, Granath L, Birkhed D. Variation of posterior approximal caries incidence
with consumption of sweets with regard to other caries-related factors in 15-18-year-olds. Community Dent Oral Epidemiol 1992;20:76-80.
20. Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol 2005;43:5721-5732.
21. Fejerskov O, Kidd E. Dental caries: the disease and its clinical management- 2nd edition. Blackwell Munksgaard: Copenhagen, 2003:163- 87.
22. Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res 2011;90:294-303.
23. Sheiham A. Dietary effects on dental diseases. Public Health Nutr 2001;4:569-591. 24. Struzycka I. The oral microbiome in dental caries. Pol J Microbiol 2014;63:127-135. 25. Featherstone JD. Prevention and reversal of dental caries: role of low level fluoride.
Community Dent Oral Epidemiol 1999;27:31-40.
26. Caries – Diagnosis, Risk Assessment and non-Invasive Treatment, A Systematic Review, The Swedish Council on Technology Assessment in Health Care 2007. 27. Lussi A. Comparison of different methods for the diagnosis of fissure caries without
cavitation. Caries Res 1993;27:409-16.
28. Cayley AS, Holt RD. The influence of audit on the diagnosis of occlusal caries. Caries Res 1997;31:97-102.
29. Nyvad B, Machiulskiene V, Baelum V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 1999;33:252-260.
30. Nyvad B, Machiulskiene V, Baelum V. Construct and predictive validity of clinical caries diagnostic criteria assessing lesion activity. J Dent Res 2003;82:117-122. 31. Shwartz M, Grondahl HG, Pliskin JS, Boffa J. A longitudinal analysis from bite-wing
radiographs of the rate of progression of approximal carious lesions through human dental enamel. Arch Oral Biol 1984;29:529-536.
32. Lervik T, Haugejorden O, Aas C. Progression of posterior approximal carious lesions in Norwegian teenagers from 1982 to 1986. Acta Odontol Scand 1990;48:223-227. 33. Mejare I, Kallest lC, Stenlund H. Incidence and progression of approximal caries from
11 to 22 years of age in Sweden: A prospective radiographic study. Caries Res 1999;33:93-100.
34. Mejare I, Stenlund H. Caries rates for the mesial surface of the first permanent molar and the distal surface of the second primary molar from 6 to 12 years of age in Sweden. Caries Res 2000;34:454-4.
35. Ridell K, Olsson H, Mejare I. Unrestored dentin caries and deep dentin restorations in Swedish adolescents. Caries Res 2008;42:164-170.
36. Mejare I, Kallestal C, Stenlund H, Johansson H. Caries development from 11 to 22 years of age: a prospective radiographic study. Prevalence and distribution. Caries Res 1998;32:10-16.
37. Ramos-Gomez FJ, Crystal YO, Ng MW, Crall JJ, Featherstone JD. Pediatric dental care: prevention and management protocols based on caries risk assessment. J Calif Dent Assoc 2010;38:746-761.
22 38. Hänsel Petersson G. Kariologisk riskbedömning.
http://www.internetodontologi.se/dyn_main.asp?page=316. Accessed 20171120. 39. Twetman S, Fontana M, Featherstone JD. Risk assessment - can we achieve
consensus? Community Dent Oral Epidemiol 2013;41:64-70.
40. Malmö university web site. Caries risk assessment. https://www.mah.se/fakulteter-
och-omraden/Odontologiska-fakulteten/Avdelning-och-kansli/Cariologi/Cariology/Caries-risk-assessment/. Accessed 20171015.
41. Hänsel Petersson G, Twetman S, Bratthall D. Evaluation of a computer program for caries risk assessment in schoolchildren. Caries Res 2002;36:327-340.
42. Mejare I, Axelsson S, Dahlén G, Espelid I, Norlund A. Caries risk assessment. A systematic review. Acta Odontol Scand 2014;72: 81–91.
43. Mejare I, Stenlund H, Zelezny-Holmlund C. Caries incidence and lesion progression from adolescence to young adulthood: a prospective 15-year cohort study in Sweden. Caries Res 2004;38:130-141.
44. Allison PJ, Schwartz S. Interproximal contact points and proximal caries in posterior primary teeth. Pediatr Dent 2003;25:334-340.
45. Margolis MQ, Hunt RJ, Vann WF,Jr, Stewart PW. Distribution of primary tooth caries in first-grade children from two nonfluoridated US communities. Pediatr Dent
1994;16:200-205.
46. Trubman A, Silberman SL, Meydrech EF. Dental caries assessment of Mississippi Head Start children. J Public Health Dent 1989;49:167-169.
47. Pallant J. SPSS Survival Manual. Berkshire, England. Open University press. Third edition 2007.
48. United Nations Convention on the Rights of the Child from 1989.
http://www.ohchr.org/EN/ProfessionalInterest/Pages/CRC.aspx. Accessed 20171110. 49. The Swedish Ethical Review Act.
https://www.epn.se/media/2348/the_ethical_review_act.pdf. Accessed 20171112. 50. Seppa L, Hausen H, Pollanen L, Helasharju K, Karkkainen S. Past caries recordings
made in Public Dental Clinics as predictors of caries prevalence in early adolescence. Community Dent Oral Epidemiol 1989;17:277-281.
51. Klein H, Bimstein E, Chosack A. Caries prevalence of the primary dentition at age seven. an indicator for future caries prevalence in the permanent dentition. Pediatr Dent 1981;3:184-185.
52. Motohashi M, Yamada H, Genkai F, Kato H, Imai T, Sato S, et al. Employing dmft score as a risk predictor for caries development in the permanent teeth in Japanese primary school girls. J Oral Sci 2006;48:233-237.
53. Westbom L, Kornfalt R. Chronic illness among children in a total population. An
epidemiological study in a Swedish primary health care district. Scand J SocMed 1987;15:87-97.
54. Hess DR. Retrospective studies and chart reviews. Respir Care 2004;49:1171-1174. 55. Statistics Sweden, 2006. In Swedish: Statistiska Centralbyrån, Befolkningsstatistik.
23 56. Statistics Sweden, 2016. In Swedish: Statistiska Centralbyrån, Befolkningsstatistik.
https://www.scb.se/sv_/Hitta-statistik/Artiklar/Finland-och-Irak-de-tva-vanligaste-fodelselanderna-bland-utrikes-fodda/#. Accessed 20170913.
57. Ridell K, Matsson L, Mejare I. Background factors associated with endodontic treatment due to caries in young permanent teeth. Acta Odontol Scand 2007;65:219-223.
58. Jacobsson B, Wendt LK, Johansson I. Dental caries and caries associated factors in Swedish 15-year-olds in relation to immigrant background. Swed Dent J 2005;29:71-79.
59. Svensson I, Gustafsson J, Uleskog E, Mathisson C, Mollai N, Kahlmeter A, et al. Oral condition and background factors in Somali immigrant children newly arrived in Sweden. Swed Dent J 2016;40:153-164.
60. Socialstyrelsen: Karies hos barn och ungdomar, En lägesrapport för år 2008.
61. Astrom AN, Jakobsen R. The effect of parental dental health behavior on that of their adolescent offspring. Acta Odontol Scand 1996 ;54:235-241.
62. Mattila ML, Rautava P, Ojanlatva A, Paunio P, Hyssala L, Helenius H, et al. Will the role of family influence dental caries among seven-year-old children? Acta Odontol Scand 2005;63:73-84.