Hälsa och samhälle
NURSES’ DAILY WORK
AT DORDRECHT PROVINCIALLY AIDED
HOSPITAL, SOUTH AFRICA - A FIELD STUDY
LOTTA FRITZON
Examensarbete i omvårdnad Malmö högskola Nivå 61-90 p Hälsa och samhälle Sjuksköterskeprogrammet 205 06 Malmö Juni 2009
NURSES’ DAILY WORK
AT DORDRECHT PROVINCIALLY AIDED
HOSPITAL, SOUTH AFRICA - A FIELD STUDY
LOTTA FRITZON
Fritzon, L. Nurses’ Daily Work at Dordrecht Provincially Aided Hospital, South Africa – a field study. Degree project, 15 Credit Points. Nursing Programme, Malmö University: Health and Society, Department of nursing, 2009.
Background: South Africa has about 50 million people, the world highest number
of HIV-positive and has a BNP at 6170 USD. The nurses are registered as a nurse after four years studies and there are approximately 2 nurses per 1000 citizens, compared to Sweden’s 10/1000. Dordrecht Provincially Aided Hospital is a district hospital, offering services as emergency, medical, surgery, maternity, paediatrics, antiretroviral treatment and serves about 15 000 people.
Aim: The aim of this study is to explore and describe nurses’ daily work at DPAH. Method: The study is accomplished as an ethnographic study, with participant
observations, informal conversations and a questionnaire. It is performed as a field study at the hospital for eight weeks. Eight nurses have been participating in the study.
Results: The analysis of the gathered data resulted in a general description of the
daily work, but also in 5 categories describing the daily work. These categories were patients relations, staff relations, responsibility, nursing and HIV.
Conclusions: The strength of this study has been the ability to provide an over all
picture of the daily work which has not been done before.
Keywords: daily work, ethnography, HIV, nurses, relations, responsibility, South
SJUKSKÖTERSKORS
DAGLIGA ARBETE
PÅ DORDERCHT PROVINCIALLY AIDED
HOSPITAL, SYDAFRIKA - EN FÄLTSTUDIE
LOTTA FRITZON
Fritzon, L. Sjuksköterskors Dagliga Arbete på Dordercht Provincially Aided Hospital, Sydafrika - En fältstudie. Examensarbete i omvårdnad 15
högskolepoäng. Malmö högskola: Hälsa och Samhälle, Utbildningsområde
omvårdnad, 2009.
Bakgrund: Sydafrika har ca 50 miljoner invånare, världens högsta antal
HIV-positiva och har en BNP per capita på 6170 USD. Sjuksköterskorna blir
legitimerade efter 4 års utbildning och där finns ungefär 2 sjuksköterskor per 1000 invånare, jämfört med Sveriges 10/1000. Dordrecht Provincially Aided Hospital är ett distriktssjukhus och erbjuder akutsjukvård, medicinsk- och kirurgisk vård, obstetrik, pediatrik, antiretroviral behandling och har ett upptagningsområde på ca 15 000 människor.
Syfte: Syftet med studien är att undersöka och beskriva sjuksköterskornas dagliga
arbete på Dordrecht Provincially Aided Hospital.
Metod: Studien är genomförd med etnografisk ansats, med deltagande
observationer, informella samtal och med ett frågeformulär. Den är gjord som en fältstudie på sjukhuset under åtta veckor. Åtta sjuksköterskor har deltagit i studien.
Resultat: Analysen av det insamlade materialet resulterade i en allmän
beskrivning av det dagliga arbetet, men även i fem kategorier som skildrar dagliga arbetet. Kategorierna var patient relationer, personal relationer, ansvar,
omvårdnad och HIV.
Slutsatser: Styrkan i studien har varit förmågan att tillhandahålla en helhetsbild av
det dagliga arbetet som inte tidigare gjorts.
Nyckelord: ansvar, dagligt arbete, etnografi, HIV, relationer, sjuksköterskor,
TABLE OF CONTENTS
ACKNOWLEDGMENTS 5
INTRODUCTION 5
BACKGROUND 6
South Africa 6
Eastern Cape and Dordrecht 6 South Africa Health System 6
Table 1 6
Nurses in South Africa 7 Health among South Africans 8 Earlier research 9
PURPOSE 10
Definitions and abbreviations 10
METHOD 10
Ethnography 10
Research method 10 Observations and field notes 11 Informal conversations 11 Self-reporting 12 Trustworthiness 12 The researchers role 13
Sampling 13 Data gathering 13 Data analysis 14 Ethics 15 Considerations 16 Permission 16 Participating information and consent 16 Confidentiality 16 RESULTS 17 An ordinary day 18 Patient relations 20 Impersonal 20 Personal 21 Patient responsibility 21 Staff relations 22 Nursing assistant 22 Between nurses 22 Superior relations 23 Doctor relations 23 Responsibility 23 Independency 23 Reliability 24 Nurses experience of responsibility 25
Nursing 25 HIV 25 DISCUSSION 26 Method 26 Trustworthiness 28 Ethics 29 Results 30 An ordinary day 30 Patient relations 30 Staff relations 31 Responsibility 31 Nursing 31 HIV 31 CONCLUSIONS 32 Future value 33 REFERENCES 34 APPENDIX 37
ACKNOWLEDGMENT
A great thanks to all the nurses at Dordrecht Provincially Aided Hospital, you made this study possible. And thanks for receiving me with such kindness. Thanks to the rest of the people working at the hospital for your hospitality and
helpfulness. I will also thank Mrs Botha for letting me come to your hospital, and for you kindness, and to Ann-Mari Campbell for your great help back in Sweden.
INTRODUCTION
South Africa, a country in between. You can get one of the best heart
transplantations in the world, but you can also be stuck with the clinic that only has a doctor one hour a week. If you have money, anything can happen, if you don’t, the worst can happen. My first contact with this amazing country were in 2001, when I came there as a student. We got to travel around, and to meet all kinds of people. I fell in love. The decision to become a nurse came to me, as I felt after years in South Africa that I couldn’t do more, I needed to have an education, to be able to help. Cause helping is what my whole spirit told me I must do.
I didn’t have much knowledge about the health system in South Africa, nor the nurses there. I only knew the people, who are also patients, and they touch me, I was going to come back, as a nurse, to make a difference.
When the opportunity to make a field study abroad was revealed to me, I put all my energy into it, to make it happen. This was my opportunity to get to know something, to see the other side of the coin, to see what the nurses were doing. To see what I was supposed to do.
South Africa 2009, we all know they had elections, we all know ANC won. Jacob Zuma, some of us heard about but did someone care? What is the value of a study like this, in a foreign country, far away? What is the value for me, as a Swedish nurse? Personally, the value is obvious, I need to know, I want to know and one day I will work there. But also, the knowledge about other nurses around the world can motivate me in my work, can show me what an important work we are doing, and can make a connection, a connection needed in the world today where we allow ourselves to explore and use other countries. If there is a connection, there are also respect and understanding, there is also a concern, and that is what will make the difference, for them. People caring. The nurses in South Africa are the same as we. They do the same job, they treat the same patients. There is no difference. If I can with this study, make one person get an interest about South Africa and the issues there, my personal purpose is fulfilled. If I can get nurses to start exchanges, to educate each other, to work in each others countries not only my purpose is fulfilled, but also the purpose and goal for the International Council of Nursing: to bring nursing together worldwide (ICN), is fulfilled. And
BACKGROUND
To get a picture of nurses’ situation in South Africa a short description of the health system, nurses’ condition and the health status of the people in South Africa will be described as well as some land facts to fully understand the situation. Also some earlier research connected to the subject will be presented.
South Africa
South Africa is about three times as big as Sweden. There are almost 50 millions inhabitants and the median age is 24 years (compare Sweden’s 41 yrs). The main religion is Christianity in different shapes but there are also Muslims, Hindus and Jews. The biggest language among the 13 officials language is Zulu, Xhosa and Afrikaans. South Africa is a republic with a new president, Jacob Zuma, since April 2009. He is the president of African National Congress, ANC, who has been in power since 1994, when South Africa had their first multi-racial elections. There is an unemployment rate at 21 % (CIA, 2009) and a BNP at 6170 US Dollars per capita (compare Sweden’s 55 620 USD). This makes South Africa one of the richest countries in Africa, but as a consequence from the previous
apartheid system the rift between classes is still big (landguiden).
Eastern Cape and Dordrecht
South Africa consists of eight provinces. Dordrecht Provincially Aided Hospital (DPAH) where this study is conducted, it situated in the Eastern Cape. In Eastern Cape there are approximately 7 millions inhabitants with a majority (83.4%) of isiXhosa people (Ecdc).
Eastern Cape is divided in eight districts with its own district and local
municipalities. Dordrecht, which is a small farming village, is situated in the Chris Hani district, in the heart of the province. This is the second largest district and has a population of 822 000 people. Most of the population is rural or semi-rural. The local municipalities in Chris Hani district have been grouped into six health districts where DPAH is situated in the Emalahleni district (EC, 2009).
South Africa Health System
The health system in South Africa starts at the Department of Health which is responsible for the legislation and standards concerning health care, national health goals and assuring the access to cost-effective health care. There is also a big private sector which is constantly growing (SA, 2008b) which is today serving about seven million people having medical aid schemes (Burger, 2006/07). The provinces have their own provincial health policies and should provide health service of good quality. There are 68 region hospitals in the whole country. In each province there are different health districts which have district hospitals, in total 281 in South Africa. The districts have their local service area with primary health care (PHC) clinics of which there are 3000 in South Africa (SA, 2008b). The services provided by the PHC clinics are disease prevention, maternity care, child healthcare including screening, health promotion, youth health services, counselling services, taking care of chronic diseases and diseases of older persons, rehabilitation, accident and emergency services, family planning, and oral health services (SA, 2008b). The patients visiting theses facilities are mainly treated by nurses trained in PHC. Patients that can not be treated at this level are referred to
the district hospitals. The PHC activity increased remarkably in the Eastern Cape from 2004-2005 (Burger, 2006/07).
DPAH is a district hospital and offer services such as emergency services, medical and surgical services, X-Ray, obstetrics/gynaecology, paediatrics and maternity services as well as Anti-Retroviral treatment. The hospital serves about 15 000 people and is to 90% subsidized by the province (EC, 2009).
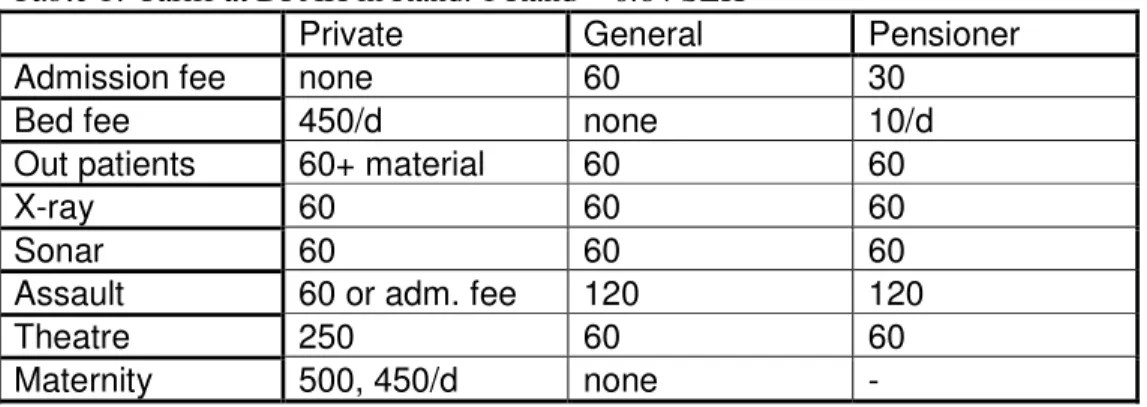
The tariff for admission at the public hospitals varies depending on the service offered. The patients pay for admission and treatments. The public hospitals also offers service to the medical aid cover and those have to pay the actual cost of the treatment (Burger, 2006/7). At DPAH the fees look like following according to posters at the hospital (table1):
Table 1: Tariff at DPAH in Rand. 1 Rand = 0.84 SEK
Private General Pensioner Admission fee none 60 30
Bed fee 450/d none 10/d Out patients 60+ material 60 60
X-ray 60 60 60
Sonar 60 60 60
Assault 60 or adm. fee 120 120
Theatre 250 60 60
Maternity 500, 450/d none -
Nurses in South Africa
South Africa Nursing Council (SANC) is a member of the International Council of Nursing. SANC registers all nurses, which are compulsory to be allowed to work. SANC’s task is to set and maintain standards for nursing education and practise in South Africa regulated by the Act No 45 of 1944 and the Nursing Act from 1978. The SANC is approving the training programs at the Nursing
Education Institutes around South Africa. It takes four year at a college or university to become a nurse. Year 2006 there were 101 295 registered nurses in South Africa. The nursing profession represents more than 50% of the total people working in the health services. The salary for a nurse is 79 407 rand / year
(SANC, 2008). In South Africa there are approximately 2 nurses/ 1000 citizens (SANC, 2009) compared to Sweden’s 10 / 1000 (WHO, 2008). In Eastern Cape there are in total 13 227 registered nurses (SANC, 2009).
At the hospital different professional groups are working. The ones in focus for this study are the registered nurses, or professional nurse as they are also called and the nursing assistants that also will be mentioned during the study.
According to the job description available at the hospital the purpose of the
nursing assistant (NA) is to “being a member of the nursing team, caring and
ensuring elementary and clinical care of patients”. Some of the tasks the NA is responsible for is to maintain personal hygiene of the patients, recording and charting observations e.g. pulse and blood pressure, to observe patients constantly by doing regular rounds and report any change in conditions, carry out order from senior staff, to work as a team with other health care workers.
This is all in accordance to the regulations SANC is providing according to the regulations of the course to be an assistant nurse where one has to be willing to cooperate with other team members, accept ethical and moral codes in nursing, and have respect for the human dignity and worth of man (No. R. 2176). One of the conditions for being registered as a nurse according to SANC is to have received 4 years of education at an approved nursing school. The curriculum shall “provide for personal and professional development of the student so that, on completion of the course of study” the nurse e.g.; shows respect to the patients, can diagnose health problem and provide appropriate nursing care, will regard the ethics, can cooperate with all in the nursing team etc. Also they must be able to “direct and control the interaction with health service consumers in such way that sympathetic and emphatic interaction takes place” and to “delineate personal practise according to personal knowledge and skill, practise it independently and accept responsibility therefore” (No. R.425)
There is a document called the Scope of nursing which regulates the responsibility the nurses have. According to this, the nurses shall, e.g.; diagnose health need and provide adequate nursing or refer to a registered person, to execute prescribed medicine, prevent disease, perform medical technical things, support the patient to maintain nutrition, exercise, elimination and other vital things. As for the midwife the scope also include the health of mother and child, to give local anaesthetics and to suture on first and second degree (No. R. 2598).
The nurses’ work regarding HIV/AIDS is regulated by a policy from the SANC to make sure the patients gets the care they deserve. The patients have the right to; confidentially, effective nursing with no judgement, empathy and the unborn child has the right to life (SANC, 2009).
Health among South Africans
The life expectancy at birth in South Africa is 48 years and the under-five mortality rate is 67/1000. Among the 50 million inhabitants more than 5.7 millions of the people have HIV/AIDS and only 1/5 of theses are receiving adequate treatment (UNAIDS 2008). Since 2003 there has been a plan to make antiretroviral treatment publicly available. By that time R330 milions were spent on HIV/AIDS programme,compared to todays R2,4 billion (Burger, 2006/07). Half of all death in South Africa is caused by HIV/AIDS (WHO, 2008). Year 2003-2004 the department of health in South Africa performed a demographic health survey among 10,000 households showing, among other things, that Easter Cape have the highest under-five mortality rate, 79/1000 and 18 % of the adults are HIV-positive (SA, 2008a). Apart from HIV/AIDS and sexual transmitted infections the most common diseases in South Africa are tuberculosis, where Eastern Cape is one of the worst-effected provinces and malaria which mainly affects the provinces in the north (Burger, 2006/07).
But South Africa is also a country having resources and moving forward. The immunization among 1-year olds for example, is more than 90 % 2005 (WHO, 2008). These efforts are paying off; it is more than 20 years since the last case of polio was confirmed, and ten years since the last case of measles (Burger, 2006/07).
Earlier research
There are not many studies to be found describing nurses daily work in South Africa. There are though studies to be read concerning nurses experiences of their daily work. These are interesting to read to get some picture of what to expect from the daily work.
A qualitative study was made by Greeff et al (2008) in South Africa, concerning HIV-positive peoples experience regarding the fact whether to disclose their HIV status or not to nurses involved in their care. The study revealed a general attitude among the HIV-positive not for the health care workers to know their status. There was a general distrust towards the nurses and other health care workers since many patients experienced a change in attitude towards them after disclosure and also since the health care workers occasionally told other in the staff about their status. Some also felt the nurses didn’t respect their privacy when giving the test results in the presents of others. The study shows the importance of information, counselling and education from health care workers but also the importance for these not to push a disclosure. The findings were also, that the nurses must be more aware of wishes of the patient, where disclosure is not always a good thing (ibid).
According to Azwihangwisi et al (2007) nurses working with HIV testing and counselling in South Africa experience their daily work as a struggle. Interviews were conducted with 20 nurses in this area. The nurses experienced difficulties in the daily work, concerning lack of recourses both material and human recourses. They also found themselves emotionally drained and stressed regarding working with people in vulnerable situations and the lack of support in their supervisor. Finally they also experienced a great frustration in their work since they couldn’t see any progress in their work (ibid).
Another study related to nurses daily work in South Africa is one conducted by La King (2006). The aim of the study was to explore “the workplace experience that had contributed to the resignations of registered nurses” (ibid, p 70) which was done through semi-structured interview with 15 nurses in their resignation month, in the Durban area. The result gives an interesting picture of these nurses
experience of their daily work. Interesting is the experience described by the nurses regarding difference areas in their daily work. They are describing their physical environment as inadequate and with dirty facilities with not enough equipment to provide good nursing care. Other areas described are safety at work, which is poor, since they are increasingly exposed to pathogens such as HIV, TB, MRSA and so on. The working hours are not satisfying, regarding the seven to seven shifts, which are too long. The relationship at work is described as
dissatisfying with the management, since they are not listening to their employees. The relations with the doctors are generally good, and with the other nurses also good with a few exceptions. About 1/4 of the participant were reporting burnouts previously, or having a current burn-out. The conclusion the researcher present is mainly that the nurses resigning is doing this because they are “dissatisfied with their hospital workplace experience, physical conditions and environment” (ibid, p 71).
PURPOSE
The aim of this study is to explore and describe nurses’ daily work at Dordrecht Provincially Aided Hospital.
Definitions and abbreviations
As referring to the daily work, this means all situations where nurses are involved between seven in the morning and four in the afternoon. Using the word nurse, that means the registered nurse. In the field notes the nurses are some times mentioned as sister, since this is what they were called or referred to as RN. The nurse assistant will be mentioned as NA.
METHOD
The method will be described concerning ethnography, research method, sampling, data gathering, data analysis and ethical considerations.
Ethnography
The author of this paper received a Minor Field Study (MFS) scholarship to perform a field study in a developing country from the Swedish International Development Cooperation Agency (SIDA). The ethnographic design was chosen since this is suitable for fieldworks and also for the aim of this study. This study was performed as an eight week field study at Dordrecht Provincially Aided Hospital in Eastern Cape, South Africa with focus on the nurses.
This study is accomplished as an ethnographic study. The ethnographic method is often used to describe a group of people and their reality. The aim is to explore, not to find what is right or wrong. The final goal is rather to create a theory about the phenomena studied but is through one single study not possible to achieve why the goal has to be to formulate a model about the observed phenomenon and their meaning to the individuals in the study. For the ethnographic researcher the individuals are the greatest source of information (Pilhammar, 1996). The ethnographic method can be regarded as an empirical qualitative study with the aim to bring a fuller understanding to the questions asked by the researcher. Participating observations, formal and informal interviews as well as written documents are some of the methods used. Ethnography is commonly used within fieldwork, since one gets to explore the context of people’s life and experience (Polit & Beck, 2006) and is suitable for the aim of this study.
Apart from other way of doing research the ethnographic design is very flexible. It is difficult to know what exact questions to ask before coming to the field,
therefore other preparations are more important (Pilhammar, 1996). In this case, much of the background information was gathered before the departure and much literature was being studied.
Research method
The different methods being used during the fieldwork will be described under the following headings; observations and field notes, informal conversations and
self-reporting from the participants. The techniques are to be described and with a motivation why the particular technique was chosen, due to Patel and Davidsson (2003).
Observations and fields notes
Observation is the main method being used since this is the basic method within ethnography (Fife 2005). Different forms of observations can be used; in this study participating observations were chosen. The main aim with the participating observation is to be there, make continuous observations of the activity and to try to share the individuals’ view of the world (Pilhammar, 1996). There are different levels of participating, varying from only observing through a video camera to participating at the same conditions as the people observed. The ideal level of observing is somewhere in between either as participating as an observer, or observing as a participant (Pilhammar, 2008). In this study the method of being
participant-as-observer was elected. This method means that the people being
observed are aware of the researcher and allow him or her to attend (Pilhammar, 2008). The participation observation was the natural choice since the author had eight weeks to spend in the field and this was the best way to gather information regarding the aim of this study. The choice of being participating as an observer, and for the nurses to know of the author’s presence was the only way to do it, considering ethical issues. The author also thinks being allowed close contact with the participants will enable more information to reach the researcher.
During ethnographic research a long time has to be spent on the field and different models can be used. The model used in this fieldwork is the compressed time model which means intensive presence during a few weeks, and the goal is to gather as much information as possible about as many phenomenon as possible, by spending time in relevant places and talk to as many relevant person as possible in this short period of time (Jeffrey and Troman, 2004). Since the time available was limited to 8 weeks, this was the appropriate way to do it.
In this study the author has been at the field for 8 weeks and at the hospital 2-3 days a week. This resulted in about 20 observation occasions (around 80 hours) written down as field notes. The field notes were written down during the observations or just after. The situation settles which way is the better way to do it, the main interest is not to disturb or attract attention (Pilhammar, 1996). During this study notes were taken during the work and as soon as possible after
completed in a quiet place. The field notes should contain where the observation took place, when it was, what kind of activity observed, what was said and done, by whom and in what way and comments about the atmosphere and the tempo. As soon as possible these notes must be transcribes, with detailed descriptions of the phenomena observed. This work will take 3 to 4 times longer than the
observations itself (Pilhammar, 1996).
Informal conversations
The conversations are an important source of information for the ethnographic researcher. The informal conversations are based on the observed situations. It can be connected to the event, or just after the situation and you are in a better place, more secluded. Those conversations are supplementary to the participating observations (Pilhammar, 1996). In this study the author has been using the informal conversations frequently. In many situations the nurses themselves
started to explain things to the author. Practical things with no sensitive information was asked during the work, and other more sensitive issues, were often discussed at the nurses duty room (NDR) as soon as possible after the occasion occurred.
Self-reporting
The self-reporting way of gathering information is a very useful way of getting information. There are many different ways of self-reporting and the researcher can modify the way of doing it to suit their own study. Different ways can be diaries, essays, or other form of writing, all of them to find out what people think about different topics (Fife, 2005). In this study the author used a semi-structured questionnaire for self-reporting, written reflections. This way of gathering data is suitable for most fields (Desai & Potter, 2006). The informants got a paper with four open questions to answer (appendix 1) and with a few instructions. They were all told that it was voluntary and supposed to be done during working hours. The forms were handed out as they were working so they had time to do it during working hours. The participants were reminded verbally to give the questionnaire back. This way of gathering information was chosen since the researcher wanted to get some additional information in addition to the observations. This way seemed to be the more appropriate way to do it, regarding the lack of time the nurses had during the day shift to sit down and talk.
Trustworthiness
According to Polit and Beck (2006) the appropriate way of assuring the trustworthiness for qualitative data is using the four criteria credibility, dependability, confirmability and transferability.
The credibility concerns the data and the rendering of the data. To assure a high credibility prolonged and persistent engagement were used, meaning the data were gathered during a long period of time and contained many observations, which according to Polit & Beck (2006) assure extensiveness and depth in the data. Triangulation regarding both data and method were being used. The data triangulation consisted in using different informants to get different sources of information. The method triangulation was done through using different methods while gathering the data. In this study participating observations, informal conversations, documents and self reporting were used.
Member checking is according to Lincon & Guba (1985) the most important method for assuring credibility in a study. In this study an informal way of member checking were used during the data gathering through the informal conversations where the researcher had the possibility to ask the informant whether the situation were correctly understood or not.
The dependability was assign through inquiry audit, which means having an external reviewer to look at the data and document being used (Polit & Beck, 2006). In this study the supervisor in Sweden has been used for this purpose. Concerning confirmability the author has been using bracketing as much as possible. Bracketing means to put your previous knowledge aside (Polit & Beck,
2006). Also reflective memos were written. The confirmability was also
established through detailed descriptions of the performance of the study (ibid). To assure transferability enough descriptive data concerning the performance of the study as well as descriptions of the settings was provided (Polit & Beck, 2006). Also enough quotes and extract from field notes occurs in the text to assure the results presented.
The researcher’s role
The role as an ethnographic researcher is to share the individuals view of the world, but without become one of theme (Pilhammar, 1996). The role chosen here is what Pilhammar calls the supporter. This is where you can closely follow the daily work, without participating yourself.
The ability to fit in is important to the participating observer, since the researcher doesn’t want to distinguish. The clothes can be of importance, meaning choosing similar cloth to fit in. (Pilhammar, 1996
).
Sampling
According to Patel & Davidsson (2003) it is appropriate to describe the esteemed informants and the sampling technique being used (ibid).
At the hospital, many different professional categories are working such as nurses, nursing assistants, doctors, reception staff, cleaning staff etc.
According to the aim of this study the inclusion criteria’s were that the informants had to be a RN, might be male or female, of all ages, and they will be involved in the daily work at the hospital while the researcher was there. The goal was to follow at least 3 different nurses to get a full picture of the work. The nurses who didn’t want to participate were excluded as well as those whose shift didn’t coincide with the authors’ schedule.
Since there are only two or three nurses working every day, and they are working often, a convenient sampling (Polit & Beck, 2006) had to be used to be able to follow an informant every day. The number of informants was also depending on this since the nurse working, had to be observed. In the end there were eight different nurses being observed. The other nurses not being there during the researcher time there were never asked to participate. The aim was never to explore all the nurses’ daily work, but the nurses available.
The other professional categories have not been observed, only when interacting with the observed nurse in order to get a full picture of the nurses’ work. They were all working together closely so to study only the nurses out of their context was not an option.
Datagathering
According to Patel & Davidsson (2003) the performance of the study has to be described, from the first contact to the field until the analysis process starts (ibid). Pilhammar (1996) describes four stages in which the field study is made. The first two will be described as follows: The preparation phase includes practical matters such as permission’s being applied for, to establish contact, to reflect over ethics and the researcher’s role (ibid).
The contact with the hospital was established in February 2008 via email. By then the permission to perform the study at the hospital was received. This meant that the contact with the main gatekeeper as well as the supervisor was established. In December 2008 an ethical application were handed in and ethical consideration were made. The 12th of December 2008 the ethical approval from Malmö University was received. In January 2009 more preparation was done regarding practical issues concerning the trip as well as getting familiar with the literature to be used.
The second stage is the time spent in the field gathering the data. It is also the time to do the first analysis to know were to continue the data gathering (Pilhammar, 1996). This took place during eight weeks in March and April 2009. The contact with the hospital was first with the gatekeeper since she was expected to introduce the informants. She gave an introduction the first day to the nurses working and after that the author introduced herself. Every new person contacted was told the purpose of the study and asked to read the information and fill in the consent form. No one was being observed without their permission. The author was at the hospital two-three days a week. First it was strictly observational and gradually the informants were identified. During week three to five, the observations continued combined with analyses. Regarding practical things the observations were only done during day-time. Much of the analysing work was done parallel. The author was following the nurses in their daily duties, and asked questions to fully understand what was happening. The nurses often explained spontaneously what was happening. The author was carrying a small notebook to take notes during the observation which was complemented straight after and written in a full version as soon as possible at the end of the day.
During the sixth week the questionnaire started to take form according to the main theme and pattern revealed during the analyses. In the first analysis of the material the broad themes will be clear and questions will be raised due to these themes. Some of these questions were chosen so the following observations could focus more on these themes. (Pilhammar, 1996). The questions were put together and handed out to the nurses participating in the study. They were supposed to fill it in during working hours and they all had at least four days at work to be able to answer the questions. The author was there during those days, so everybody had the opportunity to ask questions. They were verbally reminded to hand it back to the author. There was no drop-out for the questionnaire. The last weeks were spent observing more concerning the theme identified and the answers from the questionnaire. Much of the last week was spent to say goodbye and thanking everybody.
Data analysis
The third stage in the study according to Pilhammar (1996) is the phase analysing and interpreting the data. This starts to some extent already during the fieldwork phase but intensify when all the data is gathered (ibid).
All the collected material in this study was analysed with the content analyse method according to Burnard (1991) called “method of thematic content analyses” (ibid p 461). The qualitative content analyse is suitable to many type of materials (Lundman & Graneheim, 2008). The aim of the method according to Burnard
(1991) is to identify themes to link these and the material together in a category system.
The method contains 14 steps:
1. Memos are written after each observation occasion according to the subject discussed.
2. Reading the material and general themes are noted.
3. Open coding of the material is made to help identify relevant facts for the study, categories are identified.
4. Categories are looked over to reduce the number by combining some of them.
5. Similar categories are removed to make a final list.
6. Two extern people are identifying categories in the material.
7. The material and the final list with categories are matched and possible changes are made.
8. The material is coded regarding to the final list of categories.
9. The coded sections are cut out from the material ant gathered together. 10. The sections are put together in appropriate headings and subheadings. 11. The extern people are controlling the categories.
12. The headings and subheadings are put together in a document. 13. The rapport is written and quotes suitable for the study are chosen. 14. The material is connecting to the literature used.
Stage 6 and 11 will be excluded since the study design will not allow these steps. Memos were written after every observation occasion regarding subjects
identified during the day. All the material, questionnaire as well as field notes, was read several times to get familiar with it. Then the material was read, and general themes were noted. These themes agree to good extend with the subjects identified in the memos.
The open coding resulted in a number of categories, which were reduced during the process and a final list of five categories with ten sub-categories was created. After this the final stages were done to complete the final text.
Stage 13 and 14 coincide with the fourth and final stage according to Pilhammar (1996) which is the writing phase; the text has to be formulated and presented and the aim of the study will be fulfilled. The results will if possible be connected to earlier research (ibid). This phase took place during May 2009 when back in Sweden.
Ethics
When doing an ethnographic research it is important to consider the ethical aspects since humans are involved (Pilhammar, 1996). The following chapter will describe the different ethical issues.
Considerations
According to Polit & Beck (2006) the risks involved for the participants must be considered compared to the benefit of the study. There can occur a stressful situation for the nurses since the author will be there during their daily work observing them. Considering that they might feel obligated to take care of the
author, but also the fact that someone is observing every move they make can be stressful. Considering this, the author still thinks the reasons discussed under future values motivate the study.
Further, also the fact that the study will be performed in a foreign country has to be considered. Fife (2005) means that it is important for the researcher to be aware of the preconceived notions we have about things and it is important to get to know the country and the conditions to be able to ask the right questions and to get a full understanding of the issue being studied (ibid).
This study is conducted in accordance to the World Medical Association Declaration of Helsinki concerning ethical principles for medical research involving human subjects (WMA).
Permission
A permission to perform the study was collected from the board at Dordrecht Provincilly Aided Hospital via Mrs Botha in February 2008 via email (appendix 2). This was confirmed again with Mrs Botha at the arrival in Dordrecht. In December 2008 an ethical permission to perform the study was obtained from the Ethical Committee of the School of Health and Society at Malmö University, diarie number HS60-08/10911.
Participating information and consent
According to Kvale (1997) possible informants will receive verbal and written information (appendix 3) about the aim of the study, the method being used, the cost/benefit of participating in the study and that it is voluntary to participate. After receiving the information, the participants will sign a consent form (appendix 4).
As mentioned before, the nurses were the key-informants for the study. They were given the verbal and written information as well as the consent form. The doctors and the assistant nurses were verbally informed about the study and gave an oral consent to the author to be mentioned in the study.
Everyone concerned by this study got information about it. That included the hospital staff and the informants as well as the patients and their relatives. The patients and their relatives were not the focus of this study but when observing the nursing staff it’s impossible not to get in touch with patients and relatives. Every person who in one way or another was concerned by this study was informed that they at any time were free to withdraw their participation.
Confidentiality
Everybody involved in the study was assured confidentiality which according to Polit & Beck (2006) means that no ones identity will be revealed, no name will be mentioned and the material will be presented in such way that the participants in no way can be recognised (ibid). Considering this, all names were replaced during analysing to ensure anonymity. All the data material has been handled
confidential and kept safe.
To be able to assure the confidentiality there is a possibility to change some facts in the descriptions of the informants. It has to be information with no relevance for the aim of the study (Patel & Davidsson, 2003). This method has been used
frequently to assure the participants confidentiality by chancing names, places, hours, days etc.
Also the confidentiality for the patients at the hospital had to be considered and assured. The information concerning the patients has in no way been passed on. To be able to describe the nurses’ work, the patients had to be mentioned. The patients described in this study is fiction and has no connection to the patients at the hospital.
This is all in accordance to the Swedish laws regarding health care workers (1980:100) (1980:11).
RESULTS
By way of introduction, an ordinary day of work at DPAH will be described followed by a presentation of the five categories and ten sub-categories identified in the material through the analyse process according to Burnard (1991). All the information will serve the aim of the study; to explore and describe nurses´ daily work at DPAH.
Quotes and extract from the field notes (FN) will be used to give example of the material, to increase the credibility and to make the description more alive to the reader. References will be given after each quote or extract as FN and date, and for the questionnaire referring to the specific nurse as RN1-8.
The following categories with related sub-categories were identified in the material: Patient relations • Impersonal • Personal • Patient responsibility Staff relations • Nursing assistant • Between nurses • Superior relations • Doctor relations Responsibility • Independency • Reliability
• Nurses experience of responsibility Nursing
HIV
The eight key informants were all registered nurses with an additional year in midwifery, they all worked at DPAH, they were female and between 30 and 55 years.
An ordinary day
This is a day at the hospital; it is all put together from the field notes and put together as typical as possible. It means, this day never took place, but most days looked like this day. Sheila is a fictive person, as well as all the other people involved in the story.
Sheila starts at seven in the morning and works until seven in the evening. Today there are two other nurses working as well. One at the HIV-reception which leaves two nurses to be responsible for the ward which has 34 beds; this also includes the maternity-patients. Some days there are only one nurse at the ward. Sheila changes to her uniform, marine trousers and a white blouse, at the changing room for the staff. Everybody has to have the uniform, that can vary a lot, but it has to be white and marine. Sheila is wearing the special shoulder strap indicating she is a registered nurse and a nameplate telling her name and position. The clothes they have to supply themselves. By seven, she is in the nurses’ duty room (NDR) with the other nurse working at the ward today and with the 4 nursing assistants that they will be working with. The nurse assistants are having the same working hours as the nurses. Before the doctor arrives Sheila is placing the patients’ charts at each bed, while walking around to say good morning the patients. The nurse assistants are busy helping the few patients that needs help with coming out of bed and clean themselves. Sheila also fills in all the patients’ names in the “doctors’ order” book, so it’s ready for the round.
At eight o’clock the other nurse is going to give one of the babies an inhalation, she prepare the medicine and the big tube with oxygen is already in the room. The baby has been here for a few days, so the nurse is pouring the medicine in the container and then the mother is starting the oxygen and giving the inhalation herself. Sheila speaks Xhosa with most patients, Afrikaans or English if needed. One NA is coming back to the NDR from maternity asking Sheila to come for an admission. She goes there and the young girl is already in the examination room. She asks the girl to lie down on the bed so she can exam her. She is expecting her baby any day soon and woke up this morning with contractions. All the controls are fine and the mother is in labour so now they must just wait. Sheila is a midwife; they have to be, to be able to work at this hospital. The girl brought her patient chart from the clinic where all the information is written regarding the pregnancy, Sheila needs to be extra careful since the mother is HIV-positive. The girl is getting clothes from the hospital to wear and Sheila tells her to walk around as much as possible. While there, the phone is ringing, it is one NA calling saying the doctor is there. The time is half past eight.
When Sheila is coming to back to the ward, the doctor and the other nurse already started to walk around to the patients. The nurses have to be prepared because there is not much time with the doctor. There are also two NA joining the round. The doctor often asks the nurses to talk to the patients, sometimes she is just asking the patients what the doctor wants to know, and sometimes the nurse has to explain something to the patient, what the doctor said. The main language with the doctor is English. Since Sheila worked yesterday as well and knows most of the patients, she is walking with the doctor. The other nurse is writing in the “doctors’ order” book what has to be done during the day with each and every patient. The round is soon over and Sheila goes to the NDR together with the
doctor. Sheila makes a few phone calls for the patients being transferred, and as soon as the doctor is done with the referrals the doctor leaves.
Sheila sits down in the NDR and immediately there comes a young boy with his father, standing waiting just outside the NDR. It is only assaults and maternity patients that are allowed to come straight to the hospital with out a paper from their clinic. The boy is having blood all over him but is standing up. Sheila takes the boy to the examination room and let him sit down on a chair. The father is left in the corridor to wait. Sheila is just going to get a few things before she helps the boy and leaves him for a few minutes waiting. When she is back with him, the boy tells her everything while being stitched. Before stitching she gives him anaesthetic, she starts him on antibiotics and gives him a tetanus injection. She is used to stitch so it doesn’t take very long to finish. The boy must stay until tomorrow to wait for the doctor to have a look. Almost every day there is someone coming that’s been stabbed; the nurses are used to stitching.
Now she can continue to do the things ordered by the doctor. There is some blood to be taken; there are some antibiotic to start and some discharged to be sent home.
The time is almost ten o’clock and the visiting hour begins, Sheila is in a hurry to take the blood tests before the relatives are coming. It is only one man that the need to take blood from, so it’s quickly done.
On the way to maternity to check on the girl in labour, she meets the nurse working at the HIV-reception in the corridor. She asks her to bring one of the patients from the ward to her office for HIV-counselling and testing, the doctors’ order. She explains where the patient is, and the other nurse promise to do it as soon as she has time. The patient came in for bad coughing and the x-ray showed tuberculosis, so now the doctor wants to know the status for the patient. At maternity the girl is still trying to walk around and not much has to be done now. When Sheila is coming back to the NDR the other nurse has arranged the
transport to the other hospital for the baby with malnutrition and for the young man that needs a blood transfusion. The ambulance is coming soon and the patient relatives are having the referral that the doctor wrote for the doctor in
Queenstown. In addition to the other nurse there are two nurse assistants at the NDR as well. Also the clerk is there, standing, looking through the patients charts. They all chat for a while, laughing. Soon everybody leaves the room to continue the doctors’ order.
It’s already 12.15 and the lunch medicines are not yet given out. Sheila takes the table with the injections and antibiotics and walks to the very end of the corridor to start off at the female ward. The other nurse is at maternity so there is a NA walking around with the medicine cupboard on wheels, administering the pills. She has already put out all the charts at the beds, so for Sheila it is just to look and see if there are some injections or infusions and she will prepare and give that. There are many patients with antibiotics, since there are many tuberculosis patients, so it takes a while to prepare everything and give it. The new patients for the day, needs PVC as well to be able to give the medicines. Sheila and the NA are talking at the same time and they leave the room together. She continues all
the way around the ward so all the patients get what they need. Today there are 19 patients at the general ward, none at the private side, and two at maternity; one in labour and one already delivered.
Soon its time for lunch, but first she has to document everything at the right place, the new admissions, the referral, the discharged patients. Everything has to be written down, for the statistics.
Just before Sheila is joining the others for lunch, the police arrive. They are looking for the boy who got stabbed. Sheila shows them and tries to answer their questions. The police leave again, because the boy’s father already left and a child can’t leave a report to the police. Now it becomes Sheila’s mission to get the father back here and then make sure the police will be there at the same time. Finally at half past one, she can go for lunch. The other nurse just got back to look after the ward.
An hour later it’s time for HIV counselling. Normally it’s another nurse doing that, but she is at a meeting so Sheila will do it. It’s a girl coming in for post-exposure prophylaxis, PEP, which is given to minimize the risks of a HIV
infection after potential exposure. The counselling starts with general information about HIV and the risks, followed by information about the medicines given and the following up.
Back at the NDR all staff working, except one NA, is listening to the middle manager who is informing them about different routines. Sheila stays and listens until the NA is calling from the maternity and Sheila excuses her self and goes there.
The young lady from before is now complaining about worse pain. Sheila takes her to the examination room. She is doing all the controls for the mother and the baby. She prepares the material needed for the delivery. Short after that Sheila is delivering the baby. Sheila is looking after the mother, making sure everything is fine, and the NA is taking care of the newborn. Soon the baby and the mother is at the ward having a rest. She discusses the antiretroviral they suppose to give the baby with a colleague, and they decide what dose to give.
Time is four o’clock and it is teatime.
Patient relations
Almost all the observations done were pervaded by the patient relations. The relations can be described in different ways.
Impersonal
The majority of the observed interactions with the patient can be described as very impersonal and short. This behaviour was observed in all kind of situations and with all kinds of patients.
“Rn is saying something, she doesn’t shake her hand or anything./…Rn is examining the mother and taking her blood pressure. There is no chitchatting./…/ it is only the important stuff” (FN, 9/4)
“the woman gets a contraction and happen to kick the chart lying in the bed, the RN is telling her something with an angry voice” (FN, 1/4)
A common behaviour was for the nurses and NA to talk to each other about personal issues while handling the patients.
“The RN is talking constantly, and the two NA answers. No one talks to the patient, he is sitting silent, no one touches him” (FN, 13/3) “she is busy stitching the hand but is constantly (RN) participating in the conversation. Now they are laughing as well. /…/ it is obvious that the conversation is not concerning him” (FN, 13/3)
Body contact is also a very seldom observed phenomenon. Often they do not put a hand on the shoulder, or tickle the baby, or hold someone’s hand.
“She takes the test on the baby and he is crying and screaming. NA is talking, but not even once, she is touching the boy”(FN, 8/4)
Personal
There were also times, when personal relations with a patient were observed, even if more seldom:
“They (RN) talk and make jokes with him (a patient), there is a more intimate atmosphere than usual /…/ I can notice a different attitude towards him, a little friendlier, little more understanding.” (FN, 9/4). “They start to talk and the young woman is crying. /… /RN/.. is looking very understanding, and listens to the young woman/../ when the woman rise to leave, the RN also stands up and gives her a long hug”. (FN, 7/4)
“The RN starts to cuddle with the baby, they are talking to the mothers and everybody is laughing” (FN, 9/4)
Patient responsibility
The relations with the patients are also characterized by the big responsibility that was laid on the patients themselves. They were expecting the patients to look after themselves more or less independent except for the medical treatment. They had to get the water themselves, they carry their own referral, and the mothers with the babies had to clean up themselves if any mess were made.
“Everybody has a bottle at the bed, that they fill themselves, or a relative./…/ they are very dependent on the relatives /…/ if they want something more than the food they are getting, the relatives has to arrange for this.” (FN, 9/4)
“The woman gets a contraction/…/ now you can take of the t-shirt the RN says, the women takes it of, with a struggle, all by herself.”(FN, 1/4)
A woman in labour is asked to get up in the bed, which is high, a small step has to be used:
“the woman is whining and struggling but she isn’t getting any help, she rather seems to get a rebuke.” (FN, 1/4)
Staff relations
The relations in general seem to be very relaxed. The NDR seems to be the heart of the ward, and where everybody gathers to have a chat or to find out something. The talking seems to be never ending. Even during the work they all keep talking. Even the author, as an outsider was allowed in the conversations with no problem. They address each other very informal, with for example, mama, my dear, love etc.
Nursing assistant
The relations between the nurses and the assistant nurses seem to be good. They all feel like they are equal to each other in terms of their personal relationship. During the work the differences is obvious though. The nurses are constantly delegating things to the NA. In a nice way, and the system seems to be well established.
“The RN wants a needle for a drip and asks the NA to do this and she disappears to get the things” (FN, 13/3).
It seems to be the NA responsibility to take the controls at all the patients, the daily ones and the new one at admission. This is never asked for, but always done by a NA. It is also the NA responsibility to keep an eye on the patient and report to the nurse.
“NA is coming in to ask the RN to come, for a admission at maternity“ (FN, 9/4).
Between nurses
In the NDR the relations between the nurses was always good. They all seem to be friends, chit chatting, knowing things about each other. Regarding the relations during the daily duties, not much has been observed in this matter, since the nurse was often alone at the ward. If there where two nurses, one was often at maternity. During one whole day though, two nurses were working together, and seemed to enjoy it. They asked each other all the time, they helped each other, and planned the work together.
“They work a lot together, asking each other a lot, they talk to each other..” (FN, 9/4)
The only relation that seemed to differ was with RN2, which seemed to be a little more responsible than the others. In the informal situations, she were one of the others, but in the working situations they all came to her about questions, they all listen when she talked and she often presented new directives or rules.
“one nurse in entering, she asks about one paper, the discuss shortly, RN2 show her and the nurse leaves. Again she seems to be the one many nurses turn to with questions” (FN, 25/3).
Superior relations
The relations seem to be very straight but also friendly. They all talk to each others as friends. The ones in the superior positions are very informal, but still come with respect. At meetings everybody listen and nothing is questioned. The superiors seem to want the relations to be like this, to be a part of the staff e.g. at a meeting:
“Call me if you are too busy, I will come and help out, don’t be afraid to call/…/ let us improve and me as well.” (FN, 2/4).
Doctor relations
With the doctor there are not much time for chit chatting, but they all seem to have a good relation to her. The doctor expects full service from the rest of the employees but in a correct way. They are helping her with everything, and it seems important that everything is in order when the doctor arrives. The preparation before the doctor is coming can be exemplified by a field note:
“she is cleaning up the room, washing all the instruments, put them back on the trolley and covers it up” (FN, 13/3).
After walking the round, the doctor sits down in the NDR to write referrals mainly. During this time, the nurse doesn’t sit down for one second, but is only doing things asked by the doctor. Often the nurse knows what to do, and thus facilitate the doctors’ work.
“RN5 hasn’t been sitting at the table once since the doctor arrived. The doctor, on the other hand, was sitting all the time” (FN, 11/4).
Responsibility
As for the hole, the nurses have a lot of responsibility. They are working most days without the doctor who is there one hour every day. Also they are
responsible for many patients every day, approximately 17-20 every day with one or two responsible nurses.
Independency
A lot of the daily work is characterised by the duties performed by the nurses very independent of the doctor.
At a hospital with no doctor available, the nurses have to be able to make their own decisions. It is explained by many of them that it is not possible in another way, because of the doctor situation. They make their decisions, and if there is doubt, they call the doctor, in every case observed, afterwards making the measures. Illustrated with the following:
“she calls the doctor immediately, telling that she stitched on the upper side, to make the bleeding stop” (FN, 13/3).
“if it really is acute, they are assigned and can stay to the following day, for the doctor to have a look. Only if it is really serious, they page the doctor, otherwise they have to wait” (FN, 12/3).
The nurses are also forced to make decision they are not qualified for, such as starting treatments. Many patients were getting antibiotics, and often that was the nurses’ decision, confirmed with the doctor the following day on the round. This was expected from the doctor saying things like,
“what antibiotic did you start him on” (FN, 13/3).
When asked by the researcher if they are allowed to do that, the nurse answered:
“since the doctor is here only between eight and nine, we do like this, what else can we do?” (FN, 11/3).
Also concerning other decision this is an issue. At a meeting talking about children care, the middle manager said:
“You know your ability, you know the doctors ability and you know the ability of this hospital. As a professional nurse, it is your responsibility to make sure a child we cant handle here will be transferred./…/ We don’t have a doctor here 24/7, so therefore it is our responsibility as a professional nurse” (FN, 2/4).
The nurses are helping the doctors a lot during the round, especially after to arrange for transfers. It was more often the nurse making the necessary phone calls to other hospital than the doctor herself. Most of the time they know what had to be done, without asking the doctor.
They are also independent towards each other. They are sharing the responsibility for all patients, but never were they questioning the other persons work. When someone is doing something, they left that person to do it, and expecting them to ask for help if needed. Even for a totally new nurse, the same principals were applied. She was expected to manage by her self, but they were all willing to help as soon as she asked for it.
Reliability
They are responsible for lots of patients, and they also remember them and keep it all in their head. Every round with the doctor, the doctor ask the responsible nurse for the problem, rather than reading the chart, every day, they are able to answer for all the patients.
“often the nurses are able to answer without reading the chart” (FN, 9/4).
The impression is that the doctor trusts the nurses, since she often asks the nurse for advice:
“what do you think sister, must I send her to East London or Queenstown?” (FN, 8/4).
Most nurses gave an impression of being very alert, many time they were answering questions at the same time as doing something else without loosing focus.
“ she is telling me about the importance of adding enough NaCl to some antibiotics, while mixing the antibiotics for the patient. At the same time the NA asks about another patient and she doesn’t seem to be confused” (FN, 14/3).
Nurses experience of responsibility
None of the nurses expressed that they had too much responsibility but all agree that they have a lot. Several nurses refer to the possibility of delegating things if the responsibility gets too much. Most of them think the responsibility is enough, and gives them a challenge.
“its a lot of responsibility, but that also makes it interesting, it is a challenge” (RN1).
Nursing
Nursing was not an issue discussed in the daily work. When asking the nurses they were all giving almost the same answer of what nursing means. It means to take care of those who can’t take care of themselves for different reasons.
“Nursing means caring for sick”… (RN 3)
“To assist those individuals who cannot help themselves” (RN2) “Rendering the care to the sick” (RN8)
Nursing also means to ensure good quality care and to teach people to take care of themselves to prevent illness.
“Keep health and prevent disease” (RN3)
“Improving the health status of the public, ensuring safe, efficient and quality care” (RN 5)
HIV
The influence HIV has on the nurses’ daily work can not be ignored. Many daily duties concerns HIV-patients and the risk involved. Some of the nurses express a frustration regarding the resources spent on the matter, like spending more time on counselling, and worrying more about cross-infections.
“all our resources is spent on HIV treatment or the consequences of HIV” (FN, 25/3)
Most of the nurses consider the HIV situation in South Africa to cause a lot of stress for them:
“Staff is getting frustrated by increasingly numbers of those infected by HIV/AIDS and they burn out” ( RN1)
Also the fear of getting infected is a factor causing stress. One of the nurses put word on her fear:
“And you know, it affects all people. It doesn’t matter if you are a nurse or a lawyer or whatever, you can still get it. It is all around us“ (FN, 7/4)
DISCUSSION
The results from this study will be discussed regarding the method being used and regarding the literature and earlier research previously presented (Patel &
Davidsson, 2003).
Method
The decision to use the ethnographic design in this study was a choice based on the fact that the study was going to be a field study and should go on for 8 weeks. Regarding this the ethnographic design were suitable since it requires the
researcher to be there (in the field) to share the participants daily life for an extended period of time (Hammersley & Atkinson, 2007). Also the aim of this study; to explore and describe nurses’ daily work, is suitable for the ethnographic design since the method attempt to study peoples life as it reveals in the daily life (Desai & Potter, 2006).
The weakness of choosing this method is that the author has no experience from before to do ethnographic research. To compensate the author studied a lot of method literature before starting the study and also used it during the study. The author also had a supervisor in Sweden very familiar with the ethnographic method who has been constantly supporting.
Concerning the performance of the study a great advantage is that the author got the scholarship already in March 2008, which sat free much time for preparations and literature studies. The contact with the gate keeper was well established, which is of great importance while doing a field study (Pilhammar, 1996). Regarding the choice of the gate-keeper this was made considering practical issues. The gate keeper should make your way into the field, introduce you to the informants, and give you information regarding practical issues (ibid).
Considering this, the gate keeper chosen, was the only possible chose since she could provide all these things, also regarding the fact that all the contact had to be done through email. Things to pay attention to regarding the choice of the
gatekeeper, is that the person must have access to the right information, not to high up in the hierarchy, so they don’t know the field, but not to low down, since the lack of access can cause a problem(ibid). The gatekeeper in this study has access to all the fields wanting to be studied, she arranges the permission for the study to be signed and she arranged the contacts with the nurses. The
disadvantage was that she was in a position of power, and even though the participation were voluntary, the participant could have been affected by her influence. Since the author was given entrance to the field, and only introduced by the gatekeeper the first day to two of the nurses, this is not considered as a major problem. The consent was collected in the absence of the gatekeeper, and she never knew which nurses participated or not.
Also the results can be affected of the fact that the gatekeeper is in a superior position, since some of the participants might have been acting and answering in accordance to make her satisfied. The researcher has been trying to avoid this by making it very clear that the gatekeeper in no way is involved in the study and will get no access to the data gathered.
The observations is only done during the day time, and regarding the working hours of the nurses, seven am to seven pm, the evening hours are missed out on. The reason for this is security reasons, since it is not appropriate to be out after dark so the researcher left the hospital at four every day to have time to walk home safely. The result was not affected from this, since the aim is to describe the daily work, not the evening, or night work.
The decision to be a participant-as-observer is related to a risk of getting to friendly with the participants, and to be one of them, to “go native” (Pilhammar, 1996). There author found it difficult to refrain from developing friendly relation with the participants, since so much time was spent together with them and also depending on the very positive reception met. This was avoid through being aware of the problem, but also through focusing on the work, and not to much on the chit chatting. The advantages with the method, such as be able to establish good contact, and the possibility to use different methods in the data gathering is enabled, such as informal conversations, (Pilhammar, 1996) justifies the choice of this method.
The participant doesn’t always look at the researcher the way the researcher wish to be seen. This is of crucial importance for the results, since the information available to the researcher is depending on the participant’s attitude. In this study the author wanted to be seen as a supporter, and fulfilled this purpose well since the daily work was closely followed without participating in it. It can only be assumed that the participants saw it the same way.
About fitting in, clothes in accordance with the staff at the hospital was worn. The nurses and nurse assistants carried a uniform, but most of the other persons had private clothes. The author had brought nursing uniform, in case this would feel necessary but there were so many people moving around that the choice of private clothes seemed natural. The feeling of fitting in was also established quickly. As for the first week the feeling of being an outsider was present but gradually faded away replaced by the feeling of being known and not much fuss was made about the author’s presence.
A lot of the information was gathered during informal conversations. The difficulties faced, were problem with getting all the information. Often the conversations were interesting and long, and to take notes from this was hard. This is a weakness for the results, since some important information can have been left out early in the process.
The decision to use a questionnaire was primary based on the idea that the questions nature needed time for reflection before answering, which is given with a questionnaire. Regarding the choice of using questionnaires instead of
interviews is based on the fact that the advantage of using as interview such as a higher respondent rate, less misinterpreting (Polit & Beck, 2006) could be