0
Exploring nurses´ experiences of working with
hypertension prevention in Vietnam
The pressure is on
SUBJECT AREA: Nursing
AUTHORSCecilia Dahllöf, Grisilda Pergjegji SUPORVISOR Anna Abelsson
1
Summary
Background: Hypertension is the biggest contributor to the global burden of disease,
and has a big impact on low-to middle-income countries. Nurses are important actors in disease preventive and health promotion which is typically used to prevent hypertension. Vietnam is a middle-income country with elaborate hypertension problems. Aim: The aim of this study isto explore nurses´ experiences of working with hypertension (HT) prevention in Vietnam. Method: This is a qualitative study using semi-structured interviews and content analysis. Result: Challenges, methods and perceptions from the experiences of working as a nurse with HT prevention were identified. Lack of equipment, methods and funds, and to help the patient change bad habits were the main challenges. Conclusion: Nurses in Vietnam experience many challenges in their work to prevent HT. The challenges include lack of education, resources and difficulties to help people change behaviour. Few opportunities were perceived by the nurses. Further research is needed to explore the situation of nurses working with HT prevention, and what needs to be done on different levels to facilitate their work.
Key words: Disease prevention, health promotion, health education, interview study, sustainable development goals (SDG).
Sammanfattning
Titel: Högtryck – Sjuksköterskors upplevelser av att förebygga hypertoni i Vietnam. Bakgrund: Hypertoni är den största bidragaren till den globala sjukdomsbördan, och
låg- och medelinkomstländer drabbas extra hårt. Sjuksköterskor är viktiga aktörer i det sjukdomsförebyggande och hälsofrämjande arbete som används för att förebygga hypertoni. Vietnam är ett medelinkomstland med uttalade problem relaterade till hypertoni. Syfte: Att utforska sjuksköterskors erfarenheter av att arbeta med att förebygga högt blodtryck i Vietnam. Metod: Detta är en kvalitativ studie som använde halvstrukturerade intervjuer och innehållsanalys. Resultat: Utmaningar, metoder och upplevelser från sjuksköterskornas erfarenheter identifierades. Brist på utrustning, metoder och ekonomiska tillgångar, samt att hjälpa patienter bryta dåliga vanor, var de huvudsakliga utmaningarna. Slutsats: Sjuksköterskor i Vietnam upplever att det finns många stora utmaningar med arbetet att förebygga hypertoni. Vidare forskning krävs för att utforska vad som behöver göras på olika nivåer för att främja detta arbete.
Nyckelord: sjukdomsförebyggande, hälsofrämjande, intervjustudie, hälsoutbildning, globala mål (SDG)
2
Table of contents
Introduction________________________________________________________1 Background________________________________________________________1
- Hypertension__________________________________________________ 1 Disease prevention and health promotion____________________________ 2 - Vietnam and Danang ____________________________________________2 - Healthcare system in Vietnam _____________________________________2 - Nurses and Health promotion______________________________________3 - Theoretical framework___________________________________________ 4 - Sustainable Development Goals ___________________________________4
Aim_______________________________________________________________4 Method____________________________________________________________5 - Research design________________________________________________5 - Participants____________________________________________________5 - Sampling_ ____________________________________________________ 5 - Pilot interview__________________________________________________ 5 - Data collection_________________________________________________ 5 - Data analysis__________________________________________________ 6 - Ethical considerations____________________________________________8 Results____________________________________________________________9 - Health education_______________________________________________9
- Methods and tools_________________________________________ 9
- Content of education______________________________________ 10
- Meeting patients 10
- The patient approach______________________________________11
- Personal interest_________________________________________ 11
- Struggles and possibilities_____________________________________ 11
- Challenges______________________________________________12 - Opportunities ____________________________________________ 12 Discussion________________________________________________________12 - Method discussion_____________________________________________13 - Result discussion______________________________________________14 Conclusion________________________________________________________15 Clinical implications________________________________________________ 15 References________________________________________________________16 Appendix 1. Interview guide__________________________________________20
1
Introduction
Hypertension (HT) is a global assassin sometimes referred to as “the silent killer” (World Health Organisation [WHO], 2013). Being one of the most important risk factors for developing cardiovascular diseases such as ischaemic heart disease and stroke, HT is calculated to cause about half of all deaths due such diseases in the world – especially in low- to middle-income countries where HT causes of 51% of all strokes and 80% of all deaths by cardiovascular diseases (WHO, 2013). Low- to middle-income countries are more extensively affected by HT due to limitations in the quality and availability of healthcare systems, and restricted access to treatment and medication (WHO, 2013). Vietnam is today considered a middle-income country (International Society for Clinical Biostatistics, 2017). In Vietnam, HT has been a known health issue for many years, and research indicates that about 48-66% in the Vietnamese population is unaware of having HT, and only about 39% of those with known HT get treatment or blood pressure check-ups. (Ha, Goldberg, Allison, Chu & Nguyen, 2013; Son et al, 2014). Nurses play an important role in the work towards gaining control over HT (Himmelfarb, Commodore-Mensah & Hill, 2016).
Background
HypertensionHT has been named the biggest contributor to the global burden of disease (Lim et al, 2012). Generally, HT is defined as the blood pressure of 140/90 mmHg or higher, and the normal blood pressure as 120/80 mmHg or lower (WHO, 2013). American Heart Association redefined HT to be 130/80 mmHg or higher in 2017 (Whelton et al, 2017), but European guidelines keep to the WHO definition of 140/90 mmHg (Williams et al, 2018). HT is typically without symptoms, and the risk factors and causes of HT are mainly life style features, such as smoking, harmful alcohol use, having a sedentary or stressful life, and having an unhealthy diet with too much salt and too little fruit and vegetables (Dickson, Blackledge & Hajjar, 2006; Kent, 2016). Inheritance, obesity, diabetes and low socioeconomic status also increase the risk of developing HT (WHO, 2013). This means that many risk factors are possible to influence. Furthermore, it is cost-effective to prevent HT because it prevents people from getting other, more complicated conditions such as stroke which would require much more resources to deal with (Moran et al, 2015).
Disease prevention and health promotion
According to WHO (2014), approximately 80% of all non-communicable diseases are preventable. Preventive healthcare has the purpose of averting diseases by identifying and reducing or eliminating risk factors. Primary prevention takes place before a disease is established and is the most effective and cost effective type of prevention. Secondary prevention aims to stop or cure a disease in its early stages, and tertiary prevention is about handling established diseases. (WHO, 2019). Health promotion is defined as “the process of enabling people to increase control over, and to improve, their health” (WHO, 1998, p.1) and includes individual, social and environmental interventions. Preventive healthcare is an important part of health promotion, and when it comes to hypertension, health promotion is disease prevention. Consequently, the terms of prevention and health promotion may be used synonymously in this paper.
2
A central part of health promotion is health education, and the terms are so tightly connected that they are sometimes used interchangeably. The terms can however be separated with the argument that health education is a method to promote health and prevent diseases. (Kumar & Preetha, 2012). Many types of interventions have been proven to be effective to prevent HT, such as giving health education, improving blood pressure monitoring and providing family-support (Lu et al, 2012). It has also been found that health education programmes seem to be more effective when they require engagement of the participants, for instance if they include workshops (Lu et al, 2015).
Vietnam and Danang
Vietnam is located in south-eastern Asia, with a surface of 331 114 km2. The country borders to China, Laos and Cambodia, and the capital of Vietnam is Hanoi, situated in the northen part of the country. Vietnam has a long history of war, since a long civil war followed shortly after gaining independence from France in 1945. The civil war ended in 1975 when the communist ruled northern Vietnam defeated the US supported southern Vietnam. This ended a 30-year long period of war and made Vietnam a single-party socialist republic (Landguiden, 2016). There were about 97 million people living in Vietnam in 2018 (Central Intelligence Agency, 2018a), and the population consists of 86% Viet (Kinh) people and more than 50 different minorities making up the remaining 14%. The official language is Vietnamese and there are about 30 other minorities languages (Landguiden, 2016). Danang is the largest city of central Vietnam and consists of seven districts with a total population of 1,444 million in 2018 (Central Intelligence Agency, 2018b). The city is situated on the coastline and has one of the largest harbours in the country. The economic development in Danang is faster than average in Vietnam, primarily in sectors such as tourism and commerce (World Bank, 2013).
Healthcare System in Vietnam
There are four administrative levels in the healthcare system of Vietnam: The central and province “higher levels”, and the district and the commune “lower levels”. The central level deals with the laws and development of the healthcare sector services (Le, Kubo, Fujino, Pham & Matsuda, 2010). This level is managed by the Ministry of Health and other ministries employed by the government (Das, 2018). On the province level, there are several hospitals, care centres and medical colleges under local provincial governance, producing healthcare services and education services (Le et al., 2010). District health centres deals primarily with delivering healthcare services, and commune-managed healthcare facilities are mainly primary healthcare centres (Das, 2018). The provincial level covers a population of 1-2 million people, the district level about 100-200 thousand people and the communes 5-10 thousand people (Takashima, Wada, Tra & Smith, 2017).
The public healthcare sector reaches across all these levels and provides higher quality care than the private sector (Das, 2018). Public healthcare is generally less expensive, especially for those with healthcare insurance (Takashima et al., 2017). Despite this, it is common for people in Vietnam to choose the private sector due to accessibility issues in the public sector, such as long waiting times and bed shortages. The Government in Vietnam has made efforts to improve the healthcare system and make it more
3
accessible and affordable. Policy reforms and refined budgeting for the healthcare system have resulted in great improvements, such as funding of the healthcare for children under six years and people with poor economy. Also, efforts are made to improve the efficiency of the use of healthcare funds. Although there have been improvements, and funding is increasing, the needs are not yet met. Furthermore, Vietnam is experiencing problems with distribution of healthcare workers. This is mainly because healthcare facilities in remote areas, and healthcare facilities of district and commune levels often entails low salaries and difficult working conditions, compared with central- and province level facilities in less remote areas. Higher salaries and better working condition also make healthcare workers leave the public sector for the private sector (International Trade Administration, 2018; Le et al., 2010). In response to the healthcare challenges, the Ministry of Health launched a plan for 2016-2020, with the objectives to implement universal health coverage, to improve the quality and effectiveness of healthcare services, and to reach a balance in the allocation of healthcare workers between regions (Ministry of Health, 2016). In 2015, health insurance covered 77% of the Vietnamese population (Takashima et al., 2017), giving access to community health care services for free or at low costs. However, doubts about the quality of these services make many people chose and pay for the more expensive central- or province level health care options (Hoa, Tam, Peersman, Derese & Markuns, 2018). The consequences of this is overcrowded higher level care facilities, were patients even may need to share hospital beds (Takashima et al., 2017).
There are four different levels of nursing education in Vietnam: primary, secondary, collegial and bachelor. The length of the education varies from one to four years, and graduates from all levels work mostly with the same responsibilities (Nguyen, Duke & Forbes 2018). Issues with lack of standardised education and licencing system was addressed with the Law on Examination and Treatment, effectuated in 2016, which meant that an education of at least two years are required for nurses (Takashima et al, 2017).
Nurses and health promotion
The International Council of Nurses (ICN) puts health promotion in the ICN
framework of competencies as one of the six key principles of care (ICN, 2008). Nurses
have many health promoting functions, such as giving individual advice, group education and they play a key role in public health management and control (All-Party Parliamentary Group, 2016). The role of the nurse in the work toward HT control is extensive. It includes detection, monitoring, medication management, patient education, referral, follow-up and community health management (Himmelfarb, Commodore-Mensah & Hill, 2016)
Although there is limited research available on how nurses in Vietnam work with HT prevention, and about their experiences from this work, there are some similarities in the results of such research. For example, the interview studies by Ng’ang’a, Byrne and Ang Ngo (2014) and Pham & Ziegert (2016), have many similar aspect of their findings. These similarities include that health education is the dominating method of health promotion, that nurses work in a relationship with the patient, and a vast amount of challenges such as difficulties with helping someone change their behaviour, not having enough resources and not having enough time. Interestingly, research on the same topic, but conducted in western settings, also share these similarities. In the interview studies by Casey (2007) and Jerdén, Hillervik, Hansson, Flacking and
4
Weinehall (2006), and the literary review by Kemppainen, Tossavainen & Turunen (2013), similar results were found, with the exception that lack of resources primarily refers to education, time and workforce in western settings, but also to material and tools in the Vietnamese context.
Theoretical Framework
There is no consensus among nurses on a theoretical framework for health promotion (Piper, 2009). However, Pender´s Health Promotion Model (HPM) (1996) is frequently occurring in the literature, hence it becomes the theory of choice for this research project. The HPM aims to explain what makes people engage in health promoting behaviours. The model is constructed by the three main parts, Individual
characteristics and experiences, Behaviour specific conditions and affect and Behavioural outcome (Arnold & Boggs, 2016). The individual characteristics, such as
prior behaviour and habits and the patients´ biological psychological and socio-cultural circumstances, are important aspects for the nurse to consider when making individual health promotion plans for patients (Arnold & Boggs, 2016). The nurse can make interventions in the behaviour specific condition-part of the model, where the nurse can motivate, educate and empower patients and influence their perceived benefits of action, barriers of action and self-efficacy. The nurse can thus be part of the patient´s interpersonal influences and situational influences which could assist the patient to commit to a plan of action, and make changes toward health promoting behaviours (Piper, 2009). This provides an example of how nurses may work with health promotion through interaction with the patient.
Sustainable Development Goals
This research is in connection with Goal 3 in the United Nations (UNs) Sustainable Development Goals. Goal 3 states that by 2030, we should: “Ensure healthy lives and promote the well-being for all at all ages” (United Nations Development Programme, 2017, p.10). Goal 3 targets include:
• “[…] reduce […] premature mortality from non-communicable diseases through prevention and treatment”.
• “Achieve universal health coverage”.
• “Strengthen the capacity of all countries, in particular developing countries, for early warning, risk reduction and management of national and global health risks”. (UN, 2017, p.10)
These targets are tightly connected to the nurse competencies, which include health promotion and illness prevention (ICN, 2018).
Understanding nurses experiences from working HT prevention is important in the process of gaining control over HT, which is a difficult challenge especially in Vietnam but also in the rest of the world. Understanding the experiences of nurses could be useful for the support and education of nurses to strengthen their important role as health promoters in the battle against HT.
Aim
The aim of this study is to explore nurses´ experiences of working with HT prevention in Vietnam.
5
Method
Research design
A qualitative study design is appropriate when aiming to describe and gain deep understanding of multiple aspects of a phenomenon, and with an inductive approach, researchers can search for information without pre-established ideas about what they might find (Polit & Beck, 2016). Hence, a qualitative design with an inductive approach was chosen as the method to reach the aim of describing nurses´ experiences. Semi-structured group interviews were used in this study.
Participants
Registered nurses with at least two years of experiences, and working with HT patients, were asked to participate. Eleven nurses participated, from four different hospital units: three from the intensive care unit, three from the out-patient clinic, one from the internal medicine ward and four from the gerontology ward. The experience varied from 2-17 years (mean eight years), and the age was 24-40, (mean 31). All participants were females.
Sampling
The nurses were recruited using purposive sampling (Polit and Beck 2016). They were first briefly informed about the study and asked to take part in the interview by the Head Nurse at the hospital. Then, the researchers met the participants at the hospital where the participants were given further oral information about the topic, the research procedure, and the audio taping, and were asked if they would like to participate. A positive answer was regarded as giving an informed consent. All respondents chose to participate.
Pilot interview
A pilot interview, with two Vietnamese nurse students as participants, was conducted before the interviews at the hospital. The students were asked questions similar to the questionsfor the nurse interviews. By doing this, the questions were tested to see if they were easily understood and if they generated the type of answers relevant to this study. In addition, the use of equipment and the collaboration with the interpreter was tested and shown to run smoothly, and the time plan for the interviews was reassessed. Research theorists such as Polit and Beck (2016) promotes pilot interviews as a method to enhance the quality of interview studies.
Data collection
The data collection was performed in February 2019 at a district hospital in Danang, by interviewing nurses. The hospital belonged to one of the smaller, urban districts. The interviews were semi-structured in order to focus the conversation to be about prevention of HT, but still get extensive, complex content. All interviews were initiated with the question “How do you work with patients to prevent hypertension?”. Attendant questions such as “When you work with health education, do you use any
method or theory?” were asked throughout the interview to ensure a correct
interpretation and to gain more information and deeper understanding of certain topics (see Appendix 1). Group interviews were chosen because it is more time efficient than individual interviews, and the nurses were busy and could not leave their work for longer periods of time or on other times during the day. Furthermore, interviewing more than one participant may be beneficial both to the interview experience of the
6
nurses, and to the amount and depth of the generated data (Polit & Beck, 2016). Pen and paper was used to take notes, and a Dictaphone, Olympus VN-541PC, was used for audio recording.
The data was collected from three semi-structured interviews with four nurses in two of the interviews, and with three nurses in one of the interviews. The interviews were 30 minutes long. The questions were asked in English, then translated by interpreter. The participants answered in Vietnamese, which was translated into English by the interpreter, so that attendant questions could be asked. In one of the interviews, one participant did not agree to be audio taped, so one of the authors took notes, using pen and paper, instead. Sound recording and gathering information about the participants was managed by one of the researchers, while the questions were asked by the other researcher.
The occasion and location of the interviews were chosen by the hospital staff. The interviews took place in a conference room at the hospital. The door to the room was closed during interviews, and there was no other person in the room but the participants, the researchers and the interpreter.
Data Analysis
The notes and audio-taped data was transcribed verbatim into text on a computer shortly after the interviews were done. Noises such as laughter, sighs, or silent pauses were left out from the transcript. The process of analysing the data was based on the Taylor-Powell and Renner (2003) method for content analysis. The Taylor-Powell and Renner-method contains five steps, beginning with reading and re-reading the transcript to get a deeper understanding of the data. This first step also includes reflections regarding the quality of the data, which should help determine an appropriate level of analysis. Because Taylor-Powell and Renner (2003) do not explain different levels of analysis, the authors applied the commonly used distinction of manifest and latent content described by authors such as Granheim and Lundman (2004). The quality of the data was judged to be impaired by language issues, time restraints and the need to use an interpreter, so it was deemed appropriate to keep the analysis on a manifest level.
The second step is where the point of focus is determined, and the data is organised in a way which allows for systematic analysis (Taylor-Powell and Renner, 2003). In this study, the research question was naturally the focus point. Since the data was organised into three interviews from the beginning, it was decided to use that system rather than, for instance, divide the content after specific interview questions. The system was only used in the first steps of the analysis procedure, since the content from all three interviews was analysed as one unit in the end.
The third step is where the key ideas in the text are identified, marked out and labelled (Taylor-Powell and Renner, 2003). These labels were used as codes, so that emerging categories could be found. To do this, the text was searched for meaningful phrases, or “key ideas” that were labelled with a heading stating its topic. These headings, which could summarise a few words or a paragraph, were the codes, but in other content analysis methods they could be referred to as condensed meaning units (Graneheim and Lundman, 2004). This process was done by both authors independently, in both digital and in printed documents, before comparing the findings, to diminish the risk of misinterpretation or overlooking something. Both authors found the same key ideas and had made similar headings. Some participants tended to speak more than others
7
in some interviews, despite efforts from the authors to give each participant equal space in the conversation. To avoid that the more talkative participants would be over-represented in the analysis, the authors made efforts to include statements from all participants.
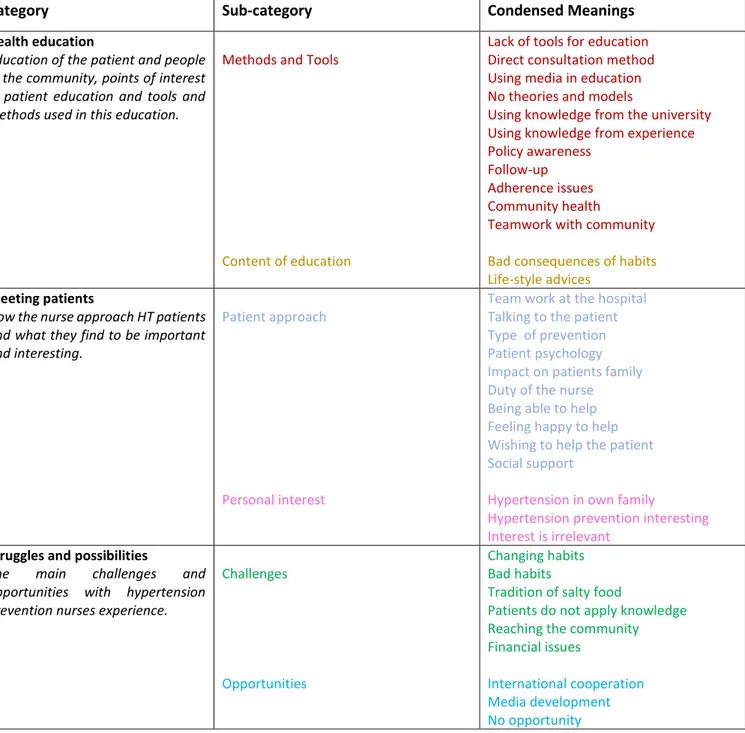
The codes from each interview were listed together, and then sorted into groups of similar topics. This was a process of sorting and re-arranging multiple times, while continuously going back to the transcript to check the context of the codes (Taylor-Powell and Renner, 2003). At first, 12 groups were formed, and in the end there were three final groups, which made the categories. The group of codes belonging to each category was then sorted into sub-categories depending on their topics. In some content analysis methods, it is common to first find subcategories that later will be used to build the categories (Graneheim and Lundman, 2004). In this method the categorization process is more dynamic, and categories are identified before or simultaneously with the subcategories: “As you categorize the data, you might identify other themes that serve as subcategories” (Taylor-Powell & Renner, 2003, p.2). This process was also itinerary and required multiple re-runs and transcript checking. In step four, the suitability of the categories are reviewed, and a deeper understanding their content, both independently and in relation to one another, is developed (Taylor-Powell and Renner, 2003). To do this, the transcripts were re-read again while each meaningful unit was marked with a different colour, depending of the sub-category it belonged to. This gave the authors indications about the prevalence of the different topics, and how they were interconnected. A short summary for each category was formulated, which was helpful to separate them and see that they do not overlap. Step five includes preparing the data for presentation. The categories are displayed and explained in connection to the result it is part of (Taylor-Powell and Renner, 2003). This is displayed in the Table 1. Each category and sub-category is presented individually in the result section.
8
Table 1. Sorting the codes into categories and sub-categories.
Ethical Considerations
In research with human subjects, when the data consists of personal thoughts, feelings and opinions, it is important to respect and protect the participants´ safety, rights and wellbeing (Polit & Beck, 2016). The four basic ethical principles, do-good, not-harm (physical or emotional), autonomy (give information and freedom of choice) and justice (about equality and respect) (Sandman & Kjellström, 2013) was taken into consideration throughout the research project. The principles were respected by providing necessary information to participants, leaving them our contact information, treating the data with concern for confidentiality and being respectful in the meetings with the participants. Moreover, principles from the Declaration of Helsinki were used to ensure an ethical conduct. These principles include risk assessment, confidentiality
Category Sub-category Condensed Meanings
Health education
Education of the patient and people in the community, points of interest in patient education and tools and methods used in this education.
Methods and Tools
Content of education
Lack of tools for education Direct consultation method Using media in education No theories and models
Using knowledge from the university Using knowledge from experience Policy awareness
Follow-up Adherence issues Community health
Teamwork with community
Bad consequences of habits Life-style advices
Meeting patients
How the nurse approach HT patients and what they find to be important and interesting.
Patient approach
Personal interest
Team work at the hospital Talking to the patient Type of prevention Patient psychology Impact on patients family Duty of the nurse Being able to help Feeling happy to help Wishing to help the patient Social support
Hypertension in own family
Hypertension prevention interesting Interest is irrelevant
Struggles and possibilities
The main challenges and opportunities with hypertension prevention nurses experience.
Challenges
Opportunities
Changing habits Bad habits
Tradition of salty food
Patients do not apply knowledge Reaching the community Financial issues
International cooperation Media development No opportunity
9
precautions, informed consent praxis and consideration regarding the general well-being of the participants (World Medical Association, 2013).
Permission from the hospitals was required in order to interview the nurses, and this was received after a written research proposal and informed consent form was submitted. These document were translated into Vietnamese. The nurses were given oral information in order for them to give an oral informed consent. Confidentiality was promised, and information was provided regarding the freedom to participate, our project and when and where it will be published. This study obtained ethical approval from the MFS-committee and Jönköping University, and received permission from the hospital before it took place.
Language issues are likely to have impacted the trustworthiness of the research, since the words of the participants has undergone two layers of interpretation, first from the interpreter and later from the authors. Sometimes long statements may have been shortened or summarised by the interpreter. When interpreting the data, the authors experiences difficulties with the abilities to consider the tones and way of talking of the participants, because of difference between the own and the Vietnamese language. The authors have no known conflicting interests or biases which would compromise the reliability of this research, and regular reflections took place throughout this project to detect any possible issues as recommended by research theorists such as Polit and Beck (2016). The pre-understandings were limited to the knowledge about HT prevention from the basic Swedish nursing programme. The authors had no preconceptions about the Vietnamese culture or healthcare system before conducting this study.
Results
The aim of this study was to explore nurses´ experiences of working with HT prevention in Vietnam. The analysis generated three categories: Health education, Meeting patients and Struggles and possibilities, each with two subcategories, which are presented below.
Health education
In the experiences of the nurses, a big part of their work with HT prevention was about giving health education. Working with health education was mentioned by all participants, and they had much to say on the topic. Health education made the largest category in the content analysis, and is divided into two sub-categories:
Methods and tools
The most common method used for health education was direct consultation with patients, and the participants frequently mentioned talking to the patient, and telling the patient what to do to prevent or manage their hypertension. The nurses also mentioned visual tools such as posters and pictures. When asked if they used any specific method or theory for talking to patient, the participants replied that they do not, but they use their knowledge and experience.
“What we often do is directly talking, another way is using poster, a picture to educate, and to use media.”
10
“We just use the knowledge from the university and the experience from working with health education. I can´t think of any theory we use”.
The nurses seemed to experience that the posters and pictures were not very helpful. Talking about methods for patient education, the nurses expressed that they experience a lack of health education resources. The participants also described that they did not experience that their work was guided or influenced by any specific policy.
“In this hospital we only use posters to educate the patient”
“It is difficult to help patients have a good diet, we have no model to follow.” “We don’t know any (policy). We have an organisation called Medical Prevention Department. In that organisation they will know about it clearly, but as staff nurses, we don’t know about it.”
The nurses talked about that they were giving health education in the community every month. This work differed from how they work with health education at the hospital, because it was done in collaboration with local organisations such as clubs for the elderly or for women. Moreover, the nurses experienced working with different tools while conducting health education for the public, compared to when educating patients at the hospital, using loudspeakers and public television to spread information.
Content of education
The participants all experienced giving similar advices to their patients. There was emphasis on the importance of taking medicines and to follow prescriptions, as well as checking the blood pressure regularly. Certain lifestyle advices were also mention in all interviews, where the participants listed healthy diet, smoking cessation, and regular physical activity. The nurses mentioned that they talk about bad beer-drinking habits with their patients, and giving the advice to reduce the salt intake from foods. Many nurses experienced that they often inform patients about the dangerous consequences of continuing with bad habits.
“We have to advise them to follow the doctor’s prescription. And to do physical activity, to have a good diet, and (…) the most important thing (…) is to do follow-up examinations. To check blood pressure regularly.”
“To help them change habits, we talk to them about negative effects of those bad habits”.
Meeting patients
Other than experiences from doing health education, the nurses talked about their experiences from meeting HT patients, and what they thought were important to keep in mind in these meetings. They also discussed whether they experience the work with such patients interesting and enjoyable or mainly frustrating and difficult. This category is divided into the following two sub-categories:
11
The patient approach
Other than performing health education when seeing patients, some nurses experience that it was important to consider the aetiology of the HT. The nurses listed reasons such as bad habits, other diseases and stress.
“First, in order to help the patient, we should know the reason why they have hypertension.”
The nurses said that they need to talk to the patient to try and help them resolve underlying issues, and consider the reason for certain behaviour. Such statements show how the nurse worked with a holistic approach to the patient, to better allow them to treat the patients´ medical condition.
“the nurse has to care about the psychology of the patient” “if they don’t follow the medication, the nurse has to know why”.
The nurses experienced that it was important to work together with the patient, and with the doctor, in their work to prevent HT. They also mentioned the importance of including family members to help patients manage HT.
“in order to work with hypertension prevention, the nurse, the doctor and the patient need to have good relationship”,
“the family play an important role in hypertension prevention”.
Personal interest
The question of whether or not the work with HT prevention was found interesting and enjoyable received different answers. The nurses said that interest was not relevant, that it was simply the duty of the nurse to do what is necessary.
“I don’t think that it is interesting or boring, I just try to work to help the patient as much as possible.”
“I don’t think that it is interesting, I feel it is difficult, but I feel it is what I should do with the duty of the nurse. I have to provide information to the patient, that is the duty, I work with my heart.”
However, some nurses talked about experiencing joy when being able to help the patient, and several nurses talked about HT prevention as something very important. Some expressed that they were pleased HT prevention was the topic of the interview.
“Yes, it is very interesting! Having interest is important. Not only for the patient, but also because people in the own family have hypertension.” “Without medication, the patient could reduce her blood pressure with the advice from a nurse! It is difficult but a lot of things make me happy to work with this.”
Struggles and possibilities
In discussions about what challenges and opportunities the nurses experience in their work with HT prevention, challenges were the dominating topic.
12
Challenges
The nurses experience many challenges when working with HT prevention. Simply put, and expressed by several nurses in all interviews:
“The big challenge is how to help patient change the behaviour.”
The participants all experienced some frustration regarding giving advice which would later be ignored. They expressed that even though they educate the patients, the patients cannot or will not apply the knowledge they receive. Reasons for this was thought to be poor education of the patient, and difficulties to change traditions and habits. The problem with salt reduction was touched upon several times, as one especially difficult factor to influence.
“The nurse gives the patient a lot of knowledge but when the patient go to their home they don’t use the knowledge.”
“Some patients listen and some don’t, even if they know the habits are bad for them.”
“In Vietnam country you know that we eat a lot of salt, so it is very difficult for us to change that habit.”
For public health education, a frequently mentioned challenge was the lack of funding. In addition to this, some participants experience that it was difficult to reach people even when they organise public health education meetings:
“We lack the finance to organise a lot of education to every commune, it is in only some of them”
“when we organise health education (in the community), a lot of people because they are busy, they cannot come to the health education meeting. So the information does not reach the people”
Opportunities
The nurses seemed to experience that there were few opportunities in their work with HT prevention. If asked about it, the answers were few and short and required some time to think. The most frequently mentioned opportunity was that the hospital had recently taken part in an educational programme about HT prevention and patient education, which was considered a big opportunity. A few nurses mentioned new means of communication through different media. Some nurse experienced a total lack of opportunities.
“another opportunity is the developing media to get information to the patient, but the patient need to use information too”.
“there are no opportunities to use health education to prevent hypertension with the salary from the hospital and do my duty – prevention of hypertension is one of my duties.”
13
Discussion
Method discussionAccording to Graneheim and Lundman (2004), the trustworthiness of qualitative research is built on the concepts of credibility, dependability and transferability. Credibility is achieved when the research measure what it is meant to measure, for instance by asking suitable questions in the interviews and by finding suitable participants. This study included a pilot interview to test the suitability of the questions, as well as conferring with the supervisors, to enhance the credibility. Furthermore, the inclusion criteria for the participants resulted in a sample from the relevant population of this study, which is proven when the result matches the research question (Polit & Beck 2016).
Dependability is about how the data is collected, whether the chosen method is suitable, and if the amount of details included by the researchers is sufficient, and it also concerns researcher bias (Polit & Beck, 2016). The possible impact of not being able to audio record one of the interviews was diminished as much as possible by allowing one researches to focus on note taking, while the other asked the questions. Group interviews were chosen so that the nurses would encourage one other and ad to each other’s statements, which would increase the richness and range of data (Polit & Beck 2016). However, the time limitation of interviewing busy nurses and language issues are likely to have limited the amount of content possible to extract from each interview. These issues are also likely to have impaired the quality of the data to some extent, as the researchers occasionally lacked the time to ask for further explanations. To deal with issues of researcher bias, the researchers have reflected on their own possible preconceptions before and after the interviews, as well as in the analysis process (Polit & Beck 2016). The analysis of the data was checked by the supervisor in Danang and the supervisor in Sweden on at least two occasions during the analysis process, to increase the chance of possible bias being detected. The supervisors were asked what they thought about the interpretations and the categories, and if it seemed appropriate and reasonable. Regular communication with the supervisors, and doing individual interpretations before a joint one, was helpful to ensure a more correct interpretation of the data. Furthermore, displaying the codes, and providing quotes to support the result may increase dependability as it demonstrated how the data is interpreted (Granheim & Lundman 2004; Polit & Beck 2016; Taylor-Powell & Renner, 2003).
Transferability in qualitative research refers to the possibility transfer the result to other settings, based on the thoroughness and detail in the descriptions of the method and the analysis process (Polit & Beck 2016). In the pursuit of transferability, the authors have attempted to supply a sufficient amount of details about the hospital and the participants, without compromising confidentiality. Moreover, a pre-existing method of content analysis was chosen and the analysis process has been described step-wise. The authors suggest that the result of this study could be applicable to other small hospitals in Vietnamese cities.
To improve this study, the researchers would consider doing individual or pair interviews instead of group interviews. By interviewing one or two participants instead of three or four, each participant would have more opportunity to speak and it could perhaps facilitate the work of interpreter. Although all participants were taking part and talking in all interviews, the oldest or most experienced nurse seemed to be expected to speak the most in each interview group. The influence of such hidden
14
power structures could perhaps be avoided in a pair interview (Polit & Beck, 2016). In hindsight, the authors also think it could be beneficial to have the audio tape translated by an interpreter after the interviews, in addition to the translation during the interviews which was necessary to get in order to ask follow-up questions. A post-interview translation could perhaps give the interpreter more time and prevent the interpreter from feeling the need to summarise or hurry like in the actual moment of the interview.
Result discussion
The main findings about the nurses´ experiences from their work with HT prevention was that giving health education was a major part of such work, and that they experienced many challenges and saw few opportunities while working to prevent HT. Previous research reinforces the notion that health education is the most common way for nurses to work with health promotion. In an interview study by Pham and Ziegert (2016) set in northern Vietnam, nurses reported that they primarily use health education to promote the health of their patients, and although it has a different approach than the present study, there are several similarities in the findings. For example, Pham and Ziegert (2016) found that the nurses experience a lack of tools and strategies to engage patients in health promoting behaviours, similar to the findings in this study. They also found that the nurses express frustration over patients that do not listen to advices. Similar topics can also be found in the result of the Irish study by Casey (2007), where nurses are found to mainly use traditional consultation methods to give health education to patients, and experience that it is difficult to help them change their behaviour. In both these studies, the nurses also mentioned the importance to include the family or social support, and how it is helpful to have a good relationship with the patient, which is also similar to the present study. This could be an indication that many nurses are in need of tools and strategies to make health education and health promotion more efficient.
The present lack of such tools and strategies may be due to structural problems and priority issues on the wards, as health promotion activities has been found to often be withdrawn in favour of more urgent tasks or to have time for a larger number of patients. This is suggested in the result of the study by Ng’ang’a et al (2014), were Vietnamese nurses are found to not have time to give much health education due to an unmanageable number of patients, and in research by Jerdén et al (2006) in which Swedish nurses are found to be torn between doing their disease-oriented work and doing health promotion communication. The priority issues in the wards can in turn be the consequence of issues on higher levels - on management levels and political levels - a conclusion drawn from the insufficient policy implementation and awareness addressed in the multi-national literary review by Kemppainen, Tossavainen & Turunen (2013), and the study by Jerdén et al (2006). Both these studies found, like the present study, that nurses are often unaware of policies, and they suggest that support from leaders is needed in order to change this. The growing burden of cardiovascular diseases in the world has resulted in a number of policies, guides and plans to be issued both nationally and globally. In Vietnam, there is a 2016-2020 national plan issued by the Ministry of Health (2016) in which one of the focal interests is preventive medicine and health promotion. Globally, there is the UNs 2030 agenda, and there are many resources and strategies for health promotion and HT prevention issued by WHO, for instance the WHO (2015) strategic cooperation strategy for Vietnam.
15
The experiences that patients did not listen and that it was difficult to evoke behaviour changes in patients was experienced as a big challenge in the result of this research. It can be discussed whether this challenge can be correlated with the apparent absence of theories and models used by the nurses when giving health education. Models such as Pender´s HPM (1996), and methods such as motivational interviewing, could perhaps be of use to make the work to prevent HT more effective and maybe help nurses see more opportunities while working with health promotion, as it could give structure and guidance in the HT prevention practice. With structures and guidelines, it could be easier to identify effective and ineffective methods and to develop useful experience and knowledge in the practice. With more time for each interview, giving the participants more time to explain further, the authors believe that aspects of these methods, as well as concepts like person-centeredness, empowerment and self-management, could have been detected, by content if not by name, in the talk about working in a relationship with the patient, understanding the reason behind poor adherence and the important role of the family.
Pender's HPM (1996) is relatable to the result of this study. The talk about working in a relationship with the patient and educating the patient shows how the nurses are part of the patient´s interpersonal and situational environment, that are displayed in the model. There were however few indications that the nurses would take into consideration or try to influence the patient's perceived self-efficacy or discuss their
perceived barriers of actions, which are other parts of the model meant to give nurses
ideas on how to help patients engage health promoting behaviours (Arnold & Boggs, 2016). The authors acknowledge that time limitations and the language barriers may have averted such topics from arising.
Conclusion
This study found that the nurses experience many challenges in their work with HT prevention, such as lack of equipment, lack models to follow, lack of techniques to use and difficulties to help patients change bad habits and live healthier lives. The nurses also experienced difficulties with inadequate funding. The opportunities were in the nurses´ experiences few and consisted mainly of new means of communication and a recently undertaken educational programme. Some positive experiences included being successful in helping patients prevent hypertension, and finding the work interesting and important. Further research is needed to investigate the situation of nurses working with hypertension prevention, and what they need in order to tackle the challenges and find new opportunities.
Clinical implications
This research aims to leadto a deeper understanding of Vietnamese nurses´ experience with HT prevention. Such an understanding may be useful to identify resources and needs among nurses in their important health promoting function, and it put emphasis on the importance of education, adequate resources and sufficient policy implementation. Health promotion and preventing HT saves lives, reduces suffering and is smart for economic reasons as well, as it saves the cost and resources of more advanced and extensive healthcare that would otherwise have been required for instance after a stroke.
16
References
All-Party Parliamentary Group. (2016). Triple Impact How developing nursing will
improve health, promote gender equality and support economic growth. Retrieved
2018-05-12 from: http://www.icn.ch/images/stories/documents/projects/nursing_ policy/DIGITAL_APPG_Triple_Impact-6.pdf
Arnold, E. & Boggs, K. U. (2016). Interpersonal relationships: Professional
communication skills for nurses. 7. Ed., St. Louis, Missouri: Elsevier
Casey, D. (2007). Nurses’ perceptions, understanding and experiences of health promotion. Journal of Clinical Nursing, 16(6), 1039-1049. DOI: 10.1111/j.1365-2702.2007.01640.x
Central Intelligence Agency. (2018a). Vietnam. Retrieved 2019-03-06 from:
https://www.cia.gov/library/publications/resources/the-world-factbook/geos/vm.html
Central Intelligence Agency. (2018b). Field Listing: Major Urban Areas. Retrieved 2019-03-06 from: https://www.cia.gov/library/publications/resources/the-world-factbook/fields/350.html
Das, K. (2018). Vietnam: Growing Demand for Healthcare Services. Vietnam Briefing. Retrieved 2019-03-08 from: https://www.vietnambriefing.com/ news/vietnam-growing-demand-healthcare-services.html/
Dickson, B. K., Blackledge, J., Hajjar, I. M. (2006). The impact of lifestyle behavior on hypertension awareness, treatment, and control in a southeastern population.
American Journal of Medical Science. 332(4),211–5. DOI: https://doi.org/10.1097/
00000441-200610000-00010
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse
Education Today, 24(2), 105-112. DOI: https://doi.org/10.1016/j.nedt.2003.10.001
Ha, D. A., Goldberg, R. J., Allison, J. J., Chu, T. H. & Nguyen, H. L. (2013). Prevalence, Awareness, Treatment, and Control of High Blood Pressure: A Population-Based Survey in Thai Nguyen, Vietnam. Public Library of Science ONE, 8(6). DOI: http://dx.doi.org.proxy.library.ju.se/10.1371/journal.pone.0066792
Hoa, N. T., Tam, N. M., Peersman, W., Derese, A. & Markuns, J. F. (2018). Development and validation of the Vietnamese primary care assessment tool. Public
Library of Science ONE, 13(1). DOI: 10.1371/journal.pone.0191181
Himmelfarb, C. R., Commodore-Mensah, Y. & Hill, M. N.. (2016). Expanding the Role of Nurses to Improve Hypertension Care and Control Globally. Annals of Global
Health, 82(2), pp.243-253. DOI: 10.1016/j.aogh.2016.02.003
International Council of Nurses. (2008). Nursing Care Continuum Framework and
Competencies. Retrieved 2018-05-12 from: https://sigafsia.ch/files/user_upload/
07_ICN_Nursing_Care_Continuum_Framework_and_Competencies.pdf
International Council of Nurses. (2018). Definition of Nursing. Retrieved 2018-05-12 from: http://www.icn.ch/who-we-are/icn-definition-of-nursing/
International Society for Clinical Biostatistics. (2017). 2017 List of Low, Lower-Middle,
2019-17
03-07 from: http://www.iscb2017.info/uploadedFiles/ ISCB2017.y23bw/fileManager/CFDC%20World%20Bank%20List.pdf
International Trade Administration. (2018). Vietnam - Healthcare. Retrieved 2019-03-06 from: https://www.export.gov/article?id=Vietnam-Healthcare&fbclid= IwAR05fGpMCZ0hPd-btOfGeN_UEnCugRNqMczkQVNfaQKqVL7DLGTOcIvdKic Jerdén, L., Hillervik, C., Hansson, A. C., Flacking, R. & Weinehall, L. (2006). Experiences of Swedish community health nurses working with health promotion and a patient‐held health record. Scandinavian Journal of Caring Sciences, 20(4), 448-454. DOI: 10.1111/j.1471-6712.2006.00427.x
Kemppainen, V., Tossavainen, K. & Turunen, H. (2013). Nurses' roles in health promotion practice: An integrative review. Health Promotion International, 28(4), 490-501. DOI: 10.1093/heapro/das034
Kent, M. (2016). Food and Fitness: A Dictionary of Diet and Exercise (2nd ed.).[Online Reader-version] Retrieved 2019-02-26 from: http://www.oxfordreference.com.proxy.library.ju.se/view/10.1093/acref/978019180 3239.001.0001/acref-9780191803239-e-896?rskey=agay8a&result=1013
Kumar, S. & Preetha, G. (2012). Health promotion: An effective tool for global health.(CME)(Report). Indian Journal of Community Medicine, 37(1), 5-12. DOI: 10.4103/0970-0218.94009
Landguiden, (2016). Vietnam. Retrieved 2019-03-04 from: https://www-ui-se.proxy.library.ju.se/landguiden/lander-och-omraden/asien/vietnam/
Le, D-C, Kubo, T, Fujino, Y., Pham, T.M. & Matsuda, S. (2010). Health Care System in Vietnam: Current Situation and Challenges. Asian Pacific Journal of Disease
Management. 4(2), 23-30 Viewed 2019-03-02, Retrieved 2019-02-28 from:
https://www.jstage.jst.go.jp/article/apjdm/4/2/4_23/_pdf
Lim, S., Vos, T., Flaxman, A. D., Danaei, G., Shibuya, K., Adair-Rohani, H. Mohammad, A.A., … Majid, E. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet,
380(9859), 2224-2260. DOI: 10.1016/S0140-6736(12)61766-8
Lu, Z., Cao, S., Chai, Y., Liang, Y., Bachmann, M., Suhrcke, M., & Song, F. (2012). Effectiveness of interventions for hypertension care in the community-a meta-analysis of controlled studies in China. BioMed Central Health Services Research, 12(1), 216. DOI: 10.1186/1472-6963-12-216
Lu, C., Tang, S., Lei, Y., Zhang, M., Lin, W., Ding, S. & Wang, P. (2015). Community-based interventions in hypertensive patients: A comparison of three health education strategies. BioMed Central Public Health, 15(1), 33. DOI: 10.1186/s12889-015-1401-6 Ministry of Health. (2016). PLAN For people’s health protection, care and promotion
2016-2020. Retrieved 2019-03-02 from: http://www.euhf.vn/upload/Strategic%
20documents/82.%20MOH%205-year%20plan%20(Eng).pdf
Moran, A. E., Odden, M. C., Thanataveerat, A., Tzong, K. Y., Rasmussen, P. W., Guzman, D., Williams, L., Bibbins-Domingo, K., Coxson, P. G. and Goldman, L. (2015). Cost-Effectiveness of Hypertension Therapy According to 2014 Guidelines. The New
18
Ng’ang’a, N., Woods Byrne, M. W., & Anh Ngo, T. (2014). In their own words: The experience of professional nurses in a Northern Vietnamese women’s hospital.
Contemporary Nurse, 47(1-2), 168-179. DOI: 10.1080/10376178.2014.11081918
Nguyen, V. N. B., Duke, M., & Forbes, H. (2017). Nurse educator confidence in clinical teaching in Vietnam: A cross-sectional study. Collegian, 25(3), 335-340. DOI: 10.1016/j.colegn.2017.09.008
Pham, L. & Ziegert, K. (2016). Ways of promoting health to patients with diabetes and chronic kidney disease from a nursing perspective in Vietnam: A phenomenographic study. International Journal of Qualitative Studies on Health and Well-being, 11(1), 30722. DOI: 10.3402/qhw.v11.30722
Piper, S. (2009). Health promotion for nurses : theory and practice, Abingdon: Routledge.
Polit, D., & Beck, C. (2016). Nursing research : Generating and assessing evidence for
nursing practice (10th ed.). Philadelphia: Wolters Kluwer.
Sandman, L., & Kjellström, S. (2013). Etikboken, etik för vårdande yrken. Lund: Studentlitteratur.
Son, P. T., Quang, N. N., Viet, N. L., Khai, P. G., Wall, S., Weinehall, L., Bonita, R. & Byass, P. (2011). Prevalence, awareness, treatment and control of hypertension in Vietnam—results from a national survey. Journal of Human Hypertension, 26(4), 268-80. DOI: https://doi.org/10.1038/jhh.2011.18
Takashima, K., Wada, K., Tra, T. & Smith, D. (2017). A review of Vietnam's healthcare reform through the Direction of Healthcare Activities (DOHA). Environmental Health
and Preventive Medicine, 22(1), p.74. DOI:10.1186/s12199-017-0682-z
Taylor-Powell, E., & Renner, M. (2003) . Analyzing qualitative data. University of Wisconsin - Extension, Program Development and Evaluation. Retrieved 2019-03-07 from: http://learningstore.uwex.edu/assets/pdfs/g3658-12.pdf
United Nations Development Programme. (2017). UNDP support to the
implementation of sustainable development goal 3. Retrieved 2018-05-12 from:
file:///C:/Users/cecil/Downloads/SDG-3%2520Health.pdf
Whelton, P. K., Carey, R.M., Aronow, W.S., Casey, D.E., Collins, K. J., Dennison Himmelfarb, C., DePalma, S. M., … Wright, T. J. Jr. (2017). 2017 ACC/AHA/AAPA/ ABC/ACPM/AGS/ APhA/ASHASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Journal of the American Society of
Hypertension. 12(8), pp.1269-1324. DOI: 10.1161/HYP.0000000000000066
Williams B, Mancia G, Spiering W., Rosei, E. A., Azizi, M., Burnier, M., Clement, D. L., … Desormais, I. (2018). 2017 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. European
Heart Journal. 00, pp.1–98. DOI: https://doi.org/10.1093/eurheartj/ehy339
World Bank. (2013). Energizing Green Cities in Southeast Asia. Retrieved 2019-03-04 from:http://www.worldbank.org/content/dam/Worldbank/document/
19
World Health Organisation. (1998). Health Promotion Glossary. Retrieved 2018-04-27 from https://www.who.int/healthpromotion/about/HPR%20Glossary %201998.pdf?ua=1
World Health Organisation. (2013). A Global Brief on Hypertension. Retrieved 2018-04-30 from: http://apps.who.int/iris/bitstream/handle/10665/79059/ WHO_DCO_WHD_2013.2_eng.pdf?sequence=1
World Health Organisation. (2014). Global status report on noncommunicable
diseases 2014. Retrieved 2019-03-06 from: https://apps.who.int/iris/bitstream/
handle/10665/148114/9789241564854_eng.pdf?sequence=1
World Health Organisation. (2015). Country Cooperation Strategy / At a glance /
Vietnam. Retrieved 2019-03-10 from: https://apps.who.int/iris/bitstream/handle/
10665/180224/ccsbrief_vnm_en.pdf;jsessionid=212DA2C5FECE00929C419D7ECD C7E066?sequence=1
World Health Organisation. (2019). EPHO5: Disease prevention, including early
detection of illness. Retrieved 2019-03-07 from:
http://www.euro.who.int/en/health- topics/Health-systems/public-health-services/policy/the-10-essential-public-health-operations/epho5-disease-prevention,-including-early-detection-of-illness2
World Medical Association. (2013). World Medical Association. Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. Journal
of the American Medical Association.310(20) pp. 2191-2194. DOI: 10.1001/jama.2013.281053
20
Appendix 1. Interview guide
Exploring nurses´ experiences of working with hypertension
prevention in Vietnam
Questions for all interviews:
How do you work to prevent hypertension?
Do you see any common challenges and opportunities in this work?
Attendant questions, examples:
What happens if you find that a patient have high blood pressure?
What do you think is important to do in order to help people prevent/manage HT? Do you have any specific method, model or theory to guide your work to prevent HT? Are there any policies which influence your work to prevent HT?